

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Environmental tobacco smoke (ETS) is defined as tobacco smoke produced by smokers and inhaled by non-smokers, irrespective of their own will.1 ETS is composed of mainstream smoke exhaled by a smoker and sidestream smoke emitted from the lighted end of a cigarette.2 ETS consists of around 15% of mainstream smoke and 85% of sidestream smoke.3 Studies have shown that inhaled sidestream smoke is four times more toxic per gram of particulate matter than mainstream smoke. Moreover, because sidestream smoke contains more harmful substances than mainstream smoke, damage caused by ETS occurs mostly in sidestream smoke.4 Tobacco smoke is composed of more than 4,000 chemicals, of which 250 are known to be harmful and more than 50 are known to cause cancer.5 In addition, third-hand smoke refers to the residual tobacco smoke pollutants that remain on surfaces and in dust after tobacco has been smoked and are re-emitted into the gas phase or react with oxidants and other compounds in the environment to yield secondary pollutants.6
Children are exposed to considerably more environmental pollutants in water, food, and air than adults.7 Exposure to tobacco smoke at home during the fetal and childhood developmental periods is probably the most common and dangerous environmental factor that can affect children.8 During infancy and childhood, children spend much time at home,9 and the home is often the most important site for ETS exposure.10 ETS exposure is a risk factor for sudden infant death syndrome and is known to cause bronchial asthma and otitis media in children.11 Infants of smoking parents are more likely to be hospitalized due to bronchitis and pneumonia than infants of non-smoking parents.12 In addition, exposure to ETS during pregnancy and early childhood is linked to childhood behavioral problems.1314 ETS exposure during pregnancy was associated with anxiety scores,15 and children's ETS exposure was associated with increased risk for both internalizing and externalizing behavior problems.16 Since the National Health Promotion Act of 1995 was enacted in Korea, public facilities have been designated as smoking cessation areas.17 However, the home is still a private space that cannot be controlled by legal measures for public spaces and may be the last place reachable by the public control measures for ETS exposure.
Thus, this study aimed to examine the current status of ETS exposure at home in Korean children and adolescents and to estimate the magnitude of contribution of ETS exposure to the behavioral problems in children and adolescents.
METHODS
Study participants
The study subjects were participants in the Korean Environmental Health Survey in Children and Adolescents (KorEHS-C), a research project that examined the environmental exposure and health status of a representative sample of children and adolescents in Korea.18 A total of 1,820 children and adolescents aged between 6 and 18 years were randomly sampled at 120 schools stratified based on the five regions nationwide, school grade (elementary, middle, and high schools), and sex from 2012 to 2013. A total of 1,602 children and adolescents aged 6–18 years were included in the study, while those aged 19 years or older (n = 3), reported as active smokers (n = 163) among adolescents aged 12–18 years, and who had missing ETS data or Korea-Child Behavior Checklist (K-CBCL) (n = 52) were excluded. A total of 577 children aged 3–5 years were sampled from 62 child care centers and kindergartens stratified by five regions, age, and sex in 2014.19 After excluding children with missing information in ETS exposure and K-CBCL assessments (n = 12), 565 children were analyzed. In the analysis, the participants were divided into three age groups: 3–5, 6–11, and 12–18 years.
ETS exposure
The following ETS exposure data were obtained from the parents' responses to the questionnaires, which were answerable by a “yes” or a “no”: “Is your child being exposed to smoke that someone smoked at home?” (current exposure to ETS at home), “Were there someone who smoked at home during pregnancy?” (exposure to ETS during pregnancy), “Were there someone who smoked at home from your childbirth to first birthday?” (exposure to ETS for the first year of life), and “Were there someone who smoked at home from your child's first birthday to the present?” (exposure to ETS from the first year to the present).
Behavior problem assessment
Behavioral problems were assessed using the Child Behavior Checklist (CBCL), originally developed by Achenbach (1991).20 We used the Korean version of CBCL in assessing children aged 1.5–5 and 4–18 years old.21 The CBCL is a clinical tool used in many countries to assess the social adaptation and emotional behavioral problems in children and adolescents. It consists of the social competence scale and the problem behavior scale. In this study, we used the parent report form in assessing problem behaviors. The problem behavior scale has three summary measures: internalization problem, which evaluates the internalized and overcontrolled behaviors; externalization problem, which evaluates the externalized and undercontrolled behaviors; and total problem behavior. As subscales, internalized problems include 6–9 subscales, i.e., emotional reactivity (only for 5 years old and below), anxious/depressive, somatic complaints, withdrawn/depressive, and social and thought problems (only for 6–18 years old). The externalized problems include attention, aggressive problems, and rule violations (only for 6–18 years old). Subscale each item is scored on a 3-point scale: 0 for not at all, 1 for occasionally visible or not severe, and 2 for frequent or severe. A total of 117 questions are possible from 0 to 234 points. When the internalizing, externalizing, and total problem behavior standard score was ≥ 60 or the subscale each had a standard score was ≥ 65, the child was classified as having problem behavior.
Population-attributable fraction
The contribution of risk factors for disease or death is quantified using the population-attributable fraction (PAF%). We calculated the PAF% of the case having problem behaviors due to ETS exposure using the following formula.22 The relative risk (RR) can be obtained via the odds ratio (OR) using the formula RR = OR/{1 − p + (p × OR)}, where p represents the ETS exposure rate in the control group.23 The ORs were obtained from the present study, and the Pe value is the proportion of population exposed to ETS:
In order to calculate the number of problem behaviors due to ETS exposure, the information on the total population of the age group was obtained from the Korean Statistical Information Service.24 For the 6–18 age group, the population recorded in 2012 and 2013 was used. In the 3–5 age group, the population recorded in 2014 was used to match with the years the survey was conducted.
Confounders and covariates
We obtained the information on the factors affecting neurobehavioral problems in children and adolescents through parent-administered questionnaires. The area was classified into Seoul metropolitan, urban, and rural. The household income for one month were categorized as “low” for incomes: < 3 million Korea Won (KRW), “middle” for incomes: 3 ≤ and < 5 million KRW, and “high” for incomes ≥ 5 million KRW. The parental educational levels (for father and mother each) were classified as follows: < 16 years and ≥ 16 years. We considered area, age, sex, household income, and father's education as covariates in the multivariate analyses.
Statistical analysis
Reflecting the sampling frame of the KorEHS-C, we considered the hierarchical, cluster, and sample weights in all data analyses. For each complex sample of children of 3–5 and 6–18 years of age, different strata, clusters, and sample weights were applied. A linear regression analysis was used to examine the association between ETS exposure at home and behavioral problems in children and adolescents. The following four ETS exposure variables, answerable by a “yes” or a “no,” were used in this model: current exposure to ETS at home, exposure to ETS during pregnancy, exposure to ETS during infancy, and exposure to ETS after infancy to date. To examine the validity of the ETS exposure information obtained from the parents' report, the data from the pilot study KorEHS-C (2011) were used to analyze the urinary cotinine concentration in accordance with the ETS exposure information reported by the parents.18 The difference was evaluated using the Wilcoxon rank-sum test and presented in the supplementary materials. Data were analyzed using the SPSS (ver. 23; IBM Corp., Armonk, NY, USA) and R 3.2.4 (Comprehensive R Archive Network: http://cran.r-project.org).
RESULTS
This study involved 565 participants aged 3–5 years old, 782 participants aged 6–11 years old, and 820 participants aged 12–18 years old. Majority of the children on all age groups are residing in the city. The percentage of participants from middle-income families were 43.5%, 44.1%, and 38.4% in the 3–5, 6–11, and 12–18 age group, respectively. The parents of the younger age group had higher educational level (Table 1).
Table 1
Characteristics of study population of KorEHS-C, 2012–2014
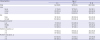
The rates of ETS exposure at home were 20.4%, 28.3%, and 39.2% in the 3–5, 6–11, and 12–18 age groups, respectively, with the youngest age group having the lowest ETS exposure rate. ETS exposure during pregnancy, infancy, and after infancy to date were similar in 3–5-year, 6–11-year, and 12–18-year age group and a bit higher in the 12–18 age group with a range of 33.8%–44.3%. The mean score of problem behavior was higher in children exposed to ETS than those not (Supplementary Table 1). Children having problem behaviors have higher ETS exposure rates than those without problem behaviors (Table 2). ETS exposure during pregnancy and infancy showed the highest agreement, with the kappa values of 0.89–0.93, while ETS exposure currently at home and during pregnancy had the lowest agreement, with the kappa values of 0.29–0.32 (Supplementary Table 2).
Table 2
Prevalence of ETS exposure in children with and without behavioral problems, KorEHS-C, 2012–2014
Values are presented as ETS exposure%b (95% CI).
ETS = environmental tobacco smoke, KorEHS = Korean Environmental Health Survey in Children and Adolescents.
aProblem behavior measured by the Korean version of Child Behavior Checklist, where children who showed scores ≥ 60 were defined as case having problems in total, internalizing, or externalizing behaviors; bWeighted percent considered the complex sampling design; cP value calculated using survey χ2 test considered the complex sampling design.
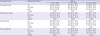
In the 12–18 age group, ETS exposure was associated with increase in total, internalizing, and externalizing behavioral problem scores within the entire exposure period, with a score range of 2.04–3.49 (Table 3). With regard to the subscales anxious/depressed, somatic complaints, social problems, aggressive behavior, and violating rules, a significant association between ETS exposure and increase in behavioral score was observed in the 12–18 age group (Supplementary Table 3). A significant association between ETS exposure and increase in total and externalizing behavioral problems but not internalizing problems was observed in the 6–11 age group (Table 3), while the scores in subscales of thought, attention, and aggressive problems significantly increased in relation to ETS exposure currently at home (Supplementary Table 2). The total and externalizing behavioral problem score in children aged 3–5 years significantly increased in relation to ETS exposure from infancy to date (Table 3). The subscales anxious, attention, and aggressive behavioral problems in 3–5 year-old children were associated with ETS exposure currently at home or from infancy to date (Supplementary Table 3).
Table 3
Association between ETS exposure at home and problem behavior, KorEHS-C, 2012–2014

Values are presented as β (95% CI)b for ETS exposure (vs. no ETS exposure).
ETS = environmental tobacco smoke, KorEHS-C = Korean Environmental Health Survey in Children and Adolescents, K-CBCL = Korean version of Child Behavior Checklist, CI = confidence interval.
aProblem behaviors measured by the K-CBCL; bβ and 95% CI calculated by using survey linear regression models adjusted by age, gender, area, household income, and father's education, considering the complex sampling design.
About 69,240 (6–11-year-old) and 123,522 (12–18-year-old) children and adolescents with problem behaviors (10.66%–11.62% of total problem behaviors) were attributed to ETS exposure at home. Problem behaviors attributed to ETS exposure currently at home are greater in children with externalizing problems (15.85%) than those with internalizing problems (11.92%) and showed the largest impact to the 12–18-year age group (Table 4).
Table 4
Population attributable fraction of problems behaviors attributed to ETS exposure currently at home, KorEHS-C, 2012–2014

ETS = environmental tobacco smoke, KorEHS-C = Korean Environmental Health Survey in Children and Adolescents, OR = odds ratio, CI = confidence interval, PAF% = population attributable fraction, RR = relative risk (%).
aProblem behaviors measured by the Korean version of Child Behavior Checklist (K-CBCL) and case defined by the K-CBCL scores ≥ 60; bOR and 95% CI estimated using survey logistic regression model adjusted for region, age, gender, household income, and father's education, considering the complex sampling design; cRR calculated by RR = OR / {1 - p + (p × OR)}, where p is the proportion of ETS exposed population among children without problem behavior; dNumber of population was the number of residents registered in 2014 for 3–5 years and those averaged in 2012–2013 for 6–18 years; ePAF% = {Pe × (RR − 1) / Pe × (RR − 1) + 1} × 100; where Pe is the proportion of exposed population.
DISCUSSION
In Korea, 20.4%–39.2% of the children and adolescents were exposed to ETS at home and showed a significant association with problem behaviors. This ETS exposure currently at home accounted for 2.7%–11.6% of the total problem behaviors in children and adolescents, particularly to externalizing problems and in the 12–18-year age group.
The rate of ETS exposure in households more than once a week in the 12–18-year age group was reported to decrease by 39.6% in 2011, 30.7% in 2013, and 29.0% in 2015 in Korea.25 This is in line with the ETS exposure rates in the present study, which reported that the rate of ETS exposure at home decreased as the age of the child became younger. Given that smoking at home is mostly driven by parental smoking, this suggests that more parents tended to quit smoking at home when they have younger child.
Pregnant women's smoking may increase the risk of early child behavioral problems.2627 In addition, ETS exposure during pregnancy was associated with increase in total and externalizing behavioral problem scores measured by K-CBCL in children.1328 A postnatal child's exposure to ETS was linked to the development of antisocial behaviors, immature problem behaviors,29 as well as internalizing and externalizing behavioral problems.30 Furthermore, a dose-response relationship between postnatal ETS exposure at home and hyperactivity/inattention and conduct problems in preschool children was found.14 The present study showed that total problem behaviors in the 6–11-year age groups and the total, internalizing, and externalizing problems in the 12–18-year age groups were significantly associated with ETS exposure at home. This result is consistent with that of the previous studies showing significant effects of postnatal ETS exposure on problem behaviors in children and adolescents.
However, the present study reported that there was no significant relationship between problem behaviors in children aged 3–5 years. Given the fact that the current exposure is sufficiently correlated with the past exposure (Supplementary Table 2) and the risk of having behavioral problems tends to be increased as children age, behavioral problems may occur prominently in periods of pubertal development after a certain period of latency or accumulation of ETS exposure since early childhood, which should be examined in future longitudinal studies. Furthermore, considering that there were 163 (16.6%) active smokers in the original data in the 12–18-year age group, there might be an additional exposure to ETS at public space such as schools for youths. Urinary cotinine levels were higher in the 12–18-year age group than that in the 6–11-year age group (Supplementary Table 4), which may reflect the additional exposure to ETS.
An animal study showed that the norepinephrine levels in the brains of rat offspring exposed to nicotine during pregnancy were significantly decreased, suggesting that exposure of the fetus to nicotine may cause problems with noradrenergic responsiveness and cause behavioral and neuroendocrine abnormalities.31 Nicotine, as well as other tobacco components, crosses the placenta32 and acts as a neurotransmitter on nicotinic receptors.33 The cholinergic nicotinic receptors are found in the fetal brain, including both serotonergic and dopaminergic neurons, and excessive stimulation of these receptors during the period of development can alter their sensitivity,34 leading to impaired neural growth and circuit formation.27 The deficits may be seen in the early life; however, the deficits may not fully appear until childhood or adolescence, once the brain circuits regulating behavioral control have matured.3536 Postnatal ETS exposure in rhesus monkey showed a potential damage to the neuronal projections accompanied by reactive sprouting.37 Aside from the teratogenic effects of tobacco smoke on the developing brain, the hypoxic effects on the fetal-placental unit and the young child's brain via reduction of blood flow, increase in the carbon monoxide levels, and adverse consequences of low birth weight and perinatal problems caused by ETS exposure were also considered indirect effects.
The results of this study can be generalized to the Korean children and adolescents based on the representativeness of the data. To our knowledge, this is the first study to estimate the PAF% of ETS exposure on problem behaviors in Korean children and adolescents. However, the present study has some limitations. First, this is a cross-sectional study and has a limited interpretation of the causal relations between ETS exposure and behavioral problems. However, considering that the relationship between exposure to ETS and children's behavior have been reported consistently in the previous studies and there was little possibility of recall bias in the present study because of sufficient correlations between periods of ETS information and its similar pattern between children with and without problem behaviors (Supplementary Table 2), we can assume that the association found in the present study would be causal and the interpretation reasonable. Second, although we considered potential confounders such as region, age, sex, household income, and father's educational level, it is unclear whether parental genetic factors could affect the children and adolescents' behavior due to lack of information. In addition, residual confounding factors such as parental attitude of child raising, psychosocial factors of children and adolescents may affect the behavior, which were not considered in the present study. However, the repeated analysis after excluding those reported ever-drinking alcohol did not show a materially changed results (Supplementary Table 5). Third, we did not use cotinine measurement data, an objective indicator of exposure to ETS, but used the questionnaire information that parents answered. Parental responses on the child's ETS exposure may be biased, especially if the child has a health problem associated with the exposure of interest. However, the urinary cotinine levels obtained from pilot surveys on 340 children and adolescent data are actually showed that the exposed group determined by parents' responses was higher in urinary cotinine than unexposed group (Supplementary Table 4). Furthermore, the consistent pattern of ETS information between periods is not that different between children with and without problem behavior (Supplementary Table 2), the ETS information provided by parents in the present study may not be considerably biased.
In conclusion, the results suggest that exposure to ETS at home is associated with an increase in behavioral problems, with an 11% contribution to the total problem behavior in the Korean children and adolescents. Therefore, reducing the ETS exposure at home to pregnant women, infants, children, and adolescents is necessary. The victims of ETS exposure at home are mainly children. The anti-smoking law in Korea, which is mainly applied to public places, does not apply to those smoking inside the house where children stay most of the time. Thus, a policy to improve parental awareness about the importance of smoking cessation at home is necessary.
 XML Download
XML Download