

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Suicide is a major cause of death.1 According to a report by the World Health Organization, suicide is the 15th leading cause of death globally, with about 804,000 people dying from suicide worldwide in 2012.2 In the United States, the suicide rate has increased steadily, showing an increase of about 2% each year between 2006 and 2014.3 In addition, Olfson et al.4 reported that the suicide attempt rate in adults increased from 0.62% to 0.79% when comparing a 2004–2005 sample of 34,629 individuals with a 2012–2013 sample of 34,712 individuals in the United States, respectively. Among the Organization for Economic Co-operation and Development (OECD) countries, Korea has the highest suicide rate and has maintained this position for more than 10 years, since 2003.5
The factors related with suicide are complex and diverse. In previous studies, various demographic and clinical characteristics, such as gender, marital status, unemployment, low income, retirement, and cancer diagnosis, were mentioned as potential factors.67 Studies on the factors associated with suicide reattempts have also implicated socioeconomic factors such as unemployment and low educational level, as well as clinical factors such as a psychiatric diagnosis.89 However, Bertolote10 mentioned in his study that suicide is intrinsically influenced by sociocultural factors, implying the possibility of differences in related factors according to the location of the empirical investigation. Recent reviews have suggested that additional studies are needed on this front, because the designs, sample sizes, and target groups of past studies have substantially differed, making comparison of their study results difficult.8
Previous suicide attempters are more likely to complete suicide than are members of the general population.11 According to previous studies, a past suicide attempt is a powerful risk factor of a reattempt,1213 and the risk of completed suicide ranges from 16% within 1 year to 23% within 4 years after a suicide attempt.14 Suicide reattempts are closely related to completed suicide1516; in fact, one study has even reported that individuals who complete suicide and those who have made serious suicide attempts are overlapping populations.16 Among the various methods of preventing suicide, there is more convincing evidence for the benefits of indicative prevention targeting individuals with a high risk of suicide than selective prevention targeting those with a moderate risk.1017 Accordingly, suicide attempters should be a target of indicated prevention, given their high suicide risk.1017
Case management for suicide attempters has been studied as a possible suicide prevention method. Case management is the coordination of community services by a professional or team to provide people the mental health care that is customized accordingly to an individual's social needs or health and aid them to their recovery.18 However, its reported effectiveness has varied substantially according to the study,19 which, according to a recent review, necessitates further research because it remains difficult to recommend case management as an effective suicide prevention method.20 Several studies attempted to confirm the short-term effects of case management (i.e., less than 1 year) by examining indirect indices such as improvement in psychiatric symptoms, psychiatric outpatient visits, and quality of life after case management was provided to people who have previously attempted suicide.212223 While these studies did find that these indirect indices improved following case management, they did not assess changes in suicide reattempts.2223 Furthermore, studies need to examine the effect of case management over the long-term period in order to truly assess its effectiveness.
Therefore, in this study, we identified the long-term preventive effect of a case management service on suicide reattempts among patients visiting the emergency department for a suicide attempt. Moreover, we investigated the other factors associated with suicide reattempts, besides their taking part in a case management service. We hypothesized that the case management service would have long-term preventive effects on suicide reattempts, and that certain demographic and clinical characteristics of people with a previous suicide attempt would be related with a higher risk of suicide reattempt.
METHODS
Study participants
Participants were individuals visiting the emergency department of Ulsan University Hospital from August 28, 2013 to July 31, 2017 for a suicide attempt. Among 917 attempters, 73 died due to the attempt, and thus were excluded from the study. Therefore, 844 individuals who attempted suicide were enrolled in the study. Participants were divided into the “case-managed group” who completed the case management service for 4 weeks and a “control group” who did not consent to the service or received the service for less than 4 weeks.
Demographic and clinical characteristics
The demographic and clinical characteristics, which were extracted from participants' medical records, were as follows: age, sex, education level, marital status, occupation, type of health insurance, suicide attempt method, psychiatric diagnosis, whether participants were admitted for a medical or surgical treatment due to the suicide attempt including general ward and intensive care unit entry, whether the participants were admitted to psychiatric department, and whether they had a cancer diagnosis. Age was categorized as < 20, 20–39, 40–59, and ≥ 60 years. The type of health insurance was classified as national health insurance, medical benefit and others (including insurance for industrial accident compensation, insurance for foreigners, and other types of insurance). Education level was divided into ≤ 6, 7–9, 10–12, 12–15, and ≥ 16 years, while marital status was classified into single, married, and others. The cancer diagnosis was made according to whether they had any code between C00 and C97 on the International Classification of Diseases, Tenth Revision (ICD-10), which indicate the presence of a malignant tumor.
Case management service
The case management service was provided for 4 weeks to suicide attempters who visited the emergency department. The case managers were certified social workers employed at the hospital. When suicide attempters visited to the emergency department, case managers performed an initial interview and asked for their consent to participate in the case management service. Case management was then provided on a weekly basis face-to-face or via telephone interviews. Following completion of case management, suicide attempters are referred to a regional mental health center for continuous management.
During case management, the case managers evaluated participants' safety and various issues related to suicide (i.e., suicide ideation and intent, and accessibility of fatal suicide methods). The general condition of suicide attempters, such as their psychiatric symptoms (e.g., depressed mood), was also examined through an interview. Case managers further evaluated participants' compliance with psychiatric outpatient treatment, encouraged their motivation for treatment, and discussed solutions to the problems faced by the suicide attempters.
Outcome
The main outcome variable was the time to revisit the emergency room due to a suicide reattempt (i.e., time to reattempt), which we compared between the case-managed and control groups. We also examined age, sex, education level, marital status, occupation, type of health insurance, suicide attempt method, psychiatric diagnosis, admission for medical or surgical treatment due to suicide attempt (including general ward and intensive care unit entry), admission to psychiatric department, and cancer diagnosis as possible factors related to suicide reattempts.
Statistical analysis
Descriptive statistics were used to identify the distributions of demographic and clinical characteristics among participants, while the χ2 test was used to compare these characteristics between the case-managed and control group. The Kaplan-Meier survival analysis was used to compare the groups in terms of the time to suicide reattempt. To assess the point prevalence of suicide reattempts throughout the 4-year observation period (median period: 19 months, interquartile range: 10–31 months), we evaluated the proportion of participants who experienced a suicide reattempt at various assessment points: namely, 6 months (24 weeks) and 1 year (48 weeks) after the suicide attempt, which was based on the procedure of previous studies.15242526 We also examined the time to reattempt for both these periods.
The event of interest in this survival analysis was a suicide reattempt after their initial visit to the emergency department for a suicide attempt. If the patient died during the observation period for any other reason, the observation ended at the date of death. The death date was confirmed by checking medical records, death certificates, and postmortem examination certificates. If these records or certificates could not be found in the electronic medical records of Ulsan University Hospital, we checked the expiration for participants' health insurance, and the observation ended at the expiration date.
To analyze factors related to suicide reattempts, we used the Cox proportional hazard model. In addition to demographic and clinical characteristics, completion of case management was included as an independent variable in the model. We first performed a univariate analysis using this model, and the multivariate analysis was conducted including only the variables with P values of less than 0.2 in the univariate analysis (although completion of case management was included in the multivariate analysis regardless of its P value). All statistical analyses were performed using SPSS statistics 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
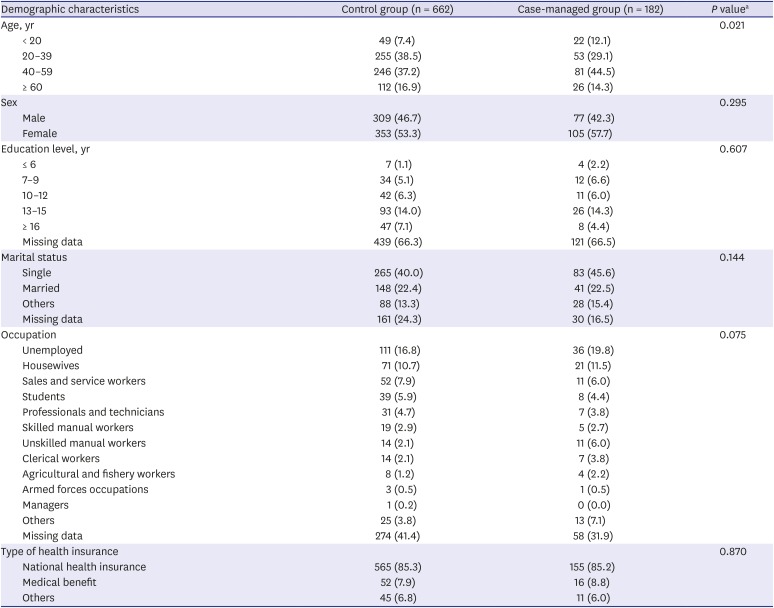
Among the 844 suicide attempters enrolled in the study, 182 (21.6%) were formed the case-managed group and 662 (78.4%) the control group. The mean age of participants was 42.8 ± 17.1 years, and 386 (45.7%) out of the 844 were male. When comparing the demographic characteristics of the case-managed and control groups, we found that the proportion of participants aged 20–39 years was higher in the control group than in the case-managed group (case-managed group, 29.1%; control group, 38.5%; P = 0.021). None of the other demographic characteristics differed between two groups (Table 1).
Table 1
Demographic characteristics of participants classified by groups
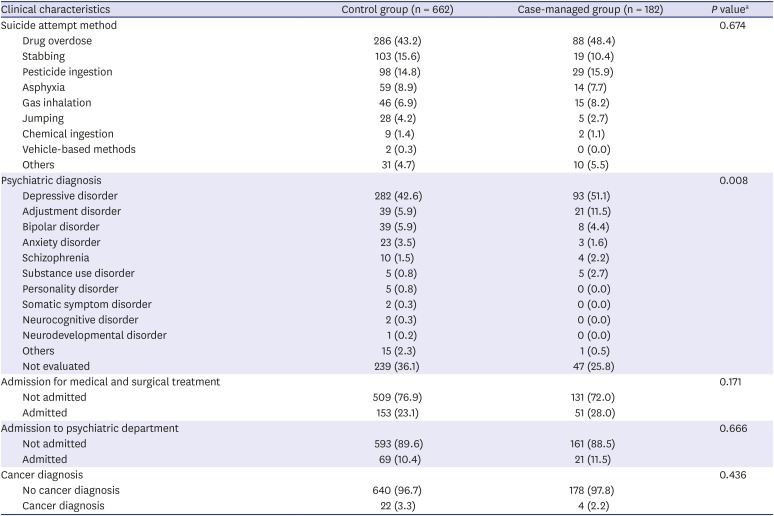
The most prevalent suicide attempt method was drug overdose (44.3%, n = 374), followed by pesticide ingestion, stabbing, asphyxia, gas inhalation, jumping, chemical ingestion, and vehicle-based methods. The psychiatric diagnoses represented in our sample included depressive disorder (44.4%, n = 375), adjustment disorder (7.1%, n = 60), and bipolar disorder (5.6%, n = 47). Among all participants, 33.9% (n = 286) were not evaluated for a psychiatric diagnosis. Two hundred four (24.2%) suicide attempters had been admitted for medical or surgical treatment including general ward and intensive care unit entry, while 90 had psychiatric department admission (10.7%). Comparing clinical characteristics between two groups, we found that the proportion of participants with depressive disorder (case-managed group, 51.1%; control group, 42.6%; P = 0.008) and adjustment disorder (case-managed group, 11.5%; control group, 5.9%; P = 0.008) was higher in the case-managed group than in the control group. There was no significant difference in other clinical characteristics between two groups (Table 2).
Table 2
Clinical characteristics of participants classified by groups
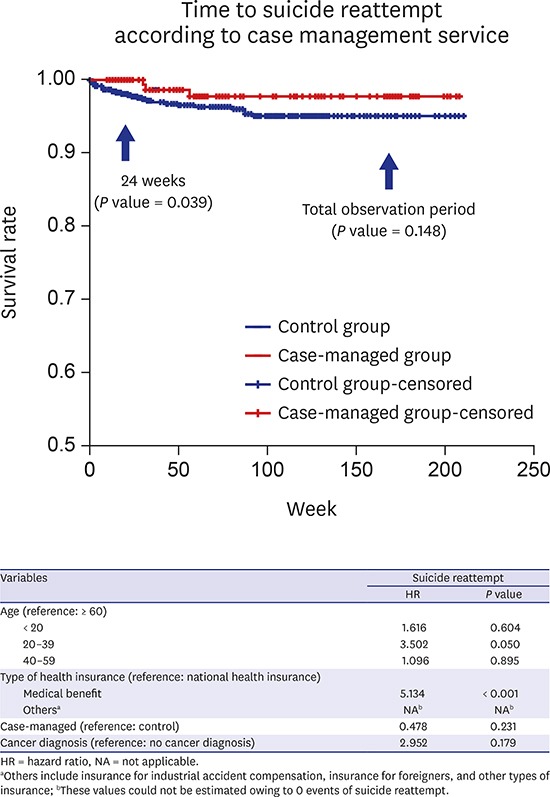
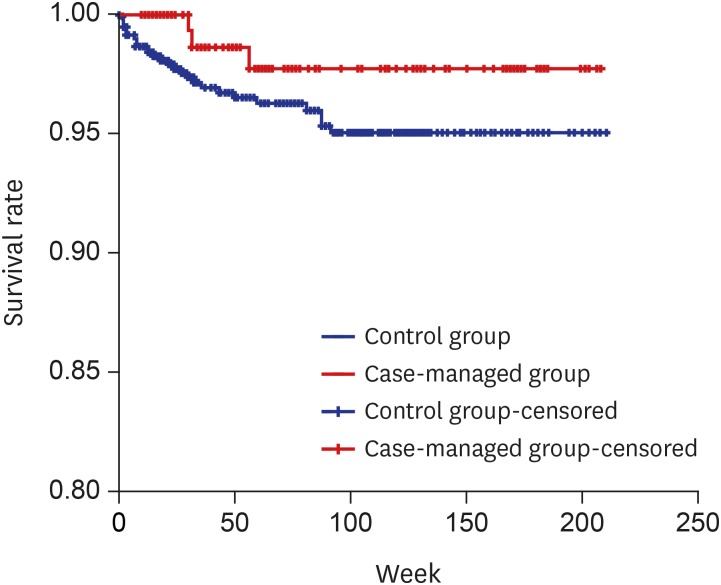
The prevalence of suicide reattempt was 3.4% (n = 29) during the total observation period, 1.8% (n = 15) during the first 24 weeks, and 2.6% (n = 22) during the first 48 weeks after the initial attempt. The Kaplan-Meier survival analysis revealed that there was no significant difference in time to reattempt between the case-managed and control groups (χ2 = 2.094; P = 0.148) (Fig. 1). However, when limiting the observation period to only 24 weeks, the survival analysis revealed that the case-managed group had a longer time to reattempt than did the control group (log-rank test = 4.243; P = 0.039). For the observation period of 48 weeks, there was no difference between two groups. In the control group, 6 participants within 1 month of the initial attempt, and 7 participants within 2 months reattempted suicide, comprising 23.1% and 26.9% of the total number of reattempts in this group, respectively. In case-managed group, on the other hand, no participant reattempted suicide within 2 months of the initial attempt.
Fig. 1
The Kaplan-Meier survival analysis showing time to suicide reattempt of case-managed group and control group.
The result of the univariate analysis of the Cox proportional hazard model revealed that the medical benefit type of health insurance was associated with a higher risk of suicide reattempt than was the national health insurance type (hazard ratio [HR], 4.666; P < 0.001). Age, completion of case management, and cancer diagnosis also showed P values of less than 0.2, and thus were included in the multivariate analysis.
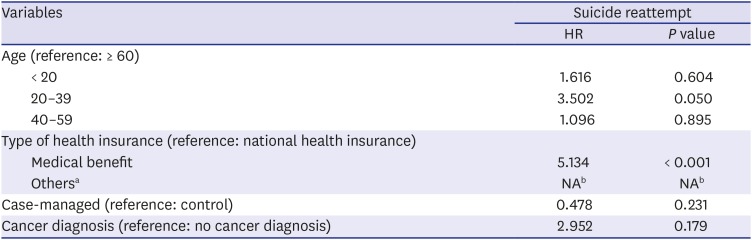
In the multivariate analysis, the medical benefit type of health insurance was associated with a significantly higher risk of suicide reattempt than was the national health insurance type (HR, 5.134; P < 0.001). Moreover, participants aged 20–39 years had a significantly higher risk of suicide reattempt than did participants aged 60 years or older (HR, 3.502; P = 0.05). Cancer diagnosis and completion of case management were not significantly associated with the risk of suicide reattempt (Table 3).
Table 3
Multivariate analysis of possible factors related to suicide reattempt using Cox proportional hazard model
DISCUSSION
No significant difference was found in the time to reattempt over the entire observation period (median period = 19 months) between participants who completed case management and those who did not. However, in the 24 weeks after the suicide attempt, suicide attempters who completed the case management service showed a longer time to reattempt than did those who did not complete it, thus confirming the short-term effect of case management service. We also found that the risk of suicide reattempt was higher among those with the medical benefit insurance type and who were aged 20–39 years.
This study did not find support for a long-term preventive effect of case management on suicide reattempts, which was in contrast to our hypothesis. One study conducted in Norway similarly did not observe a significant effect of case management on preventing suicide over a 5-year observation periods.27 On the other hand, Cebria et al.28 confirmed that case management did have an effect at 1 year after an initial suicide attempt, but also mentioned the need for additional studies to confirm this long-term effect. Although we found no long-term preventive effect on suicide, our study nevertheless has the strength of continuing the observation for more than 1 year. As far as we know, the observation period of this study was the longest among studies on this topic conducted in Asia.
As noted above, the time to suicide reattempt in the first 24 weeks after the initial suicide attempt was significantly longer in the case-managed group, which suggests that case management is effective only for a certain period. Previous studies providing regular letters to suicide attempters also reported temporary effects.29 Goldney30 suggested that the intervention period for preventing suicide must be relatively lengthy because suicide attempters tend to have a chronic history of suicide; accordingly, time-limited interventions would be ineffective because they might only have a transient effect on preventing suicide. In addition, Tidemalm et al.31 indicated that high-risk individuals such as patients with mood disorders or schizophrenia should have at least 2 years of follow-up care after a suicide attempt. Both these studies emphasized that the effect of case management is time-limited for suicide attempters, meaning that a sufficiently lengthy period of case management is required. The period of case management in previous studies varied from 2 months to 5 years,222728 but it is difficult to compare the effects of these different interventions because the study design and specific content of the management differed according to the study. Therefore, further studies are needed to evaluate the duration of the effect according to the period of case management, which could help in establishing an appropriate management period.
The content of the case management service in our study, as in previous studies,2428 included evaluation of the safety of the suicide attempters, assessment of their psychiatric symptoms and treatment compliance, and discussion of the solutions to the problems that they were facing. Several studies have suggested that case management is useful for encouraging psychiatric treatment among suicide attempters212428 and providing them with some measure of social support.2025 Furthermore, studies providing case management via letters, telephone calls, and face-to-face visits suggested that the effectiveness of case management is in part based on the feeling of connectedness to others that it induces.152932 It is possible, therefore, that the case management service in the present study played a similar role for suicide attempters.
In our study, the risk of suicide reattempt was higher when participants had the medical benefit type of health insurance, compared to national health insurance. This finding is consistent with the study of Lee et al.33, which reported that individuals receiving medical benefit insurance in Korea had a higher risk of suicide. Since the type of health insurance directly reflects an individual's socioeconomic status,33 our findings appear to suggest a relation between socioeconomic status and suicide reattempts. In fact, according to a 2013 review study, suicide reattempts were more related to specific socioeconomic factors, such as a high unemployment rate and low educational level, than was the initial suicide attempt.19 Although we could not find specific factors related to the suicide reattempt because of the limited data, the results still correspond well with those of earlier studies9 supporting an association between a risk of suicidal reattempt and low socioeconomic status.
We also observed that the risk of suicide reattempt was higher among participants aged 20–39 years than among those aged 60 years and older. Jeon et al.34 similarly reported that the risk of suicide reattempt was high among young adults aged 18–29 years, which is similar to our result. In another study conducted in Korea, suicide ideation among participants in their late 20s and 30s was found to be the result of economic problems such as unemployment.35 Olfson et al.4 similarly reported that the increased prevalence of suicide attempts among individuals between the ages of 21 and 34 years in the United States related to the high unemployment rate and economic stress. These two studies indicate that suicide among young adults can be explained by socioeconomic stress. It should be noted, however, that a recent review reported that the majority of studies have not found an association between age and suicide reattempts.8 Thus, we cannot suggest a definitive relation between them based on our results. Furthermore, inferring the cause of the observed relationship is difficult. Therefore, additional studies are needed to ascertain the relationship between age and suicide reattempt, and also suggest the cause by evaluating the characteristics of age group with high risk.
We observed no association between a diagnosis of cancer and suicide reattempts. In contrast to our results, previous studies reported that the suicide rate or risk of suicide attempt was higher among individuals with a cancer diagnosis.36 The conflicting results might be explained by the fact that other studies have noted that the risk of suicide is highest within the first year after a cancer diagnosis, after which it is difficult to find an independent association between suicide and cancer diagnosis.7 In this study, we had no information on the time elapsed from the cancer diagnosis to the initial suicide attempt, as the cancer diagnosis was made merely by the presence of an ICD-10 code in their medical record. Therefore, it is possible that some subjects reattempted suicide 1 year or more after the cancer diagnosis, which might have made the relationship non-significant.
We observed no increased risk of suicide reattempts according to marital status or method of suicide attempt. Previous studies have reported that divorced, unmarried, or bereaved individuals had a higher risk of suicide reattempts,3437 and that drug intoxication was related with a higher risk of suicide reattempt than were other suicide methods.38 This discrepancy might be explained by our dependence on self-reported information. Some participants did not reveal their marital status at the initial interview, which might have biased the analysis. For the findings concerning suicide attempt method, the disagreement between our result and previous reports might be attributable to the low statistical validity due to the small number of subjects who reattempted suicide in each category of suicide method.
The present study has several limitations. First, because the study was limited to a local university hospital, generalization of the results is limited. Second, since we classified the groups based on whether participants completed 4 weeks of the service or not, participants could not be randomized. Third, this study was a retrospective cohort study, which might have limited our obtaining accurate information from the medical records. Specifically, some of the demographic and clinical characteristics might have been biased due to missing data. Finally, it is possible that some participants who reattempted suicide did not visit the same hospital as for their previous attempt. An earlier study in Japan identified several risk factors of suicide reattempts, and noted the possibility that suicide attempters might visit other hospitals.38 However, the authors of that study also noted that their sample was from a specific area of the country in which there was no other hospital nearby that can deal with both psychiatric and medical problems, suggesting that the likelihood of participants visiting other hospitals is low. As the hospital of this study is also the only general hospital of its surrounding region capable of performing both medical and psychiatric care, it is unlikely that participants visited other hospitals.
In conclusion, a 4-week case management service was found to have a temporary effect on risk of suicide reattempt in the first 24 weeks after the initial suicide attempt, although it did not delay the time to suicide reattempt over the total observation period. Because case management appears to have a temporary effect, in future studies, the appropriate length of case management must be identified by assessing differences in preventive effects according to the duration of case management. We also found that the medical benefit type of health insurance and being aged 20–39 years were related to a higher risk of suicide reattempts, which indicates the need for further studies and intensive management of these population groups. Our study results can serve as basic data useful for preparing suicide prevention policies involving case management.
 XML Download
XML Download