

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
There is an unprecedented increase in the Korean older adult population, with associated increased frailty and demands on the Korean health care system. National statistics for Korea indicate that those over 65 years of age now exceeds 14% of the population, with this increasing to 21% by year 2026, and 40% by year 2050.1 This extremely aged population will present many challenges for the Korean government and society as an increasing frail and vulnerable population increases demands on the health care system, including both primary and specialty care. For the purposes of the following discussion, geriatric medicine will be considered as providing comprehensive primary and specialty care to older adults in whom independence, function, and quality of life are paramount along with management of their various diseases and specific older adult conditions.234 While the awareness of geriatric medicine as a specialty for physicians caring exclusively for older adults has improved greatly in recent decades among Korean health care providers and older adult patients, there is still great opportunity to improve training opportunities for all medical students, primary care physicians, and geriatrics specialty. Korea must also formally establish uniform geriatric medicine fellowships and certification. However, a number of barriers continue to exist to implement widespread, quality geriatric medicine in the Korean health care system.
WHY GERIATRIC MEDICINE IS NEEDED IN KOREA
Unfortunately, Korea is poorly prepared to meet the healthcare needs of its rapidly growing population of older adults, many of whom are frail.56 As they age, these older adults will likely develop at least one chronic medical condition. These conditions will often present in atypical and subtle ways that may go unnoticed by many healthcare providers.78 These patients may also develop one or more common geriatric syndromes such as falls, delirium, dementia, incontinence, polypharmacy, and frailty. Over time, these individuals will become more dependent on the fragmented Korean healthcare delivery model where services are often delivered by multiple providers without any meaningful care coordination.89
Due to the inevitability of its aging society and the exponential increase in associated medical expenses, Korea must seek ways to balance providing excellent care to its aged population, reducing the associated increasingly high medical costs, and provide efficient services to the increasing number of older adults with limited resources. Korea's 2016 national medical expenditure was approximately KRW 73.5 trillion (USD 73.5 billion), of which one-third of the cost was for the medical expenses of the aged. For example, the socio-economic costs incurred by 459,068 demented patients in 2015 exceeded KRW 1.6 trillion (USD 1.6 billion). Of these costs, direct medical expenses comprised 76.8% with a great deal of this spending occurring in geriatric hospitals.10 The development of an efficient model of healthcare for Korean older adults will require that primary care physicians be much better trained in Geriatrics, many more geriatricians be trained, and team-based care be implemented to improve healthcare delivery to the aged.
For both the United States (U.S.) and Korea, aging is an overwhelming concern for the government and society. Like the U.S., many more geriatricians will be needed in Korea to contribute to the development of appropriate older adult medical care and related services.5
Geriatric medicine must play a major role in research and healthcare system development in Korea to best care for its aging population. Geriatricians must be instrumental in introducing advanced and efficient older adult healthcare systems into Korea, as well as providing leadership in Korean policymaking initiatives for older adult healthcare.
Differences between adult and geriatric medicine
Geriatrics differs from typical adult medicine because it focuses on the unique needs of older adult patients. The aged body is different physiologically from the younger adult body, with age-related decline of various organ systems occurring. Longstanding health issues and lifestyle choices produce a different constellation of diseases and symptoms in individual older adults, with the aged population becoming increasingly more heterogeneous than homogenous.81112 The appearance of symptoms depends on the remaining healthy reserves in the older adult's organs, i.e., functional reserve or physiologic homeostasis. Geriatricians distinguish between disease states and the effects of normal aging, with the aim to treat disease and foster optimal aging. Geriatricians focus on preserving as much function, independence and quality of life as possible, as well as achieving the patient's highest health care priorities in the context of multiple chronic conditions.2412
Geriatric syndromes
Geriatric syndromes are the central focus for geriatricians in assessing and treating their patients. These syndromes can be major causes of impairment in older adults, especially as they begin to cognitively and physically decline. Important geriatric syndromes are immobility, gait instability, incontinence, depression, impaired intellect/memory, impaired vision and hearing loss.1213 Geriatric syndromes can also be synergistic; such as, hearing problems leading to social isolation, depression, and dependence as the older adult can no longer adequately communicate with other people. Another example is vision problems leading to falls, medicine being taken incorrectly, and finances being mismanaged.
Practical concerns
Functional ability, independence and quality of life issues are of the highest priority for geriatricians in treating their patients. Older adults generally want to live independently as long as possible, which requires them to successfully engage in self-care and other activities of daily living. A geriatrician seeks to provide information about older adult care options to patients and families; including, helping coordinate referrals to home care services, skilled nursing facilities, assisted living facilities, and hospice as appropriate.
Geriatricians are trained to help patients make decisions about the realistic benefit of the many medical interventions now available. Frail older adults may choose to decline some kinds of medical care, because the risk-benefit ratio is different for the aged. For example, frail older adults would generally stop lipid screening and might stop lipid lowering medication, since hyperlipidemia-related illness is typically a slow process that would not cause them pain, functional impairment, or be life limiting before they die of another cause. Frail older adults are also assisted by geriatricians with their increased risk of post-surgical complications.14 An accurate prediction, based on validated measures, can help older patients make fully informed choices about their options. Assessment of older patients by well-informed providers before elective surgery can help accurately predict the older adult patient's trajectory of recovery.15
MEETING THE DEMAND FOR GERIATRIC MEDICINE IN KOREA
The increased demand for older adult healthcare services in Korea cannot currently be met due to an unprepared primary care workforce and dramatic shortage of geriatricians. Currently, there are no official geriatricians in Korea, though 5,048 physicians are working in geriatric hospital10 and about 7,000 physicians are entitled to be certified geriatricians as qualified by 3 geriatric societies through required learning and examination without the benefit of specific geriatric clinical trainings.5 In addition, the Elderly Welfare Law requires that there be contracted physicians in nursing homes having 10 beds. Furthermore, the Ministry of Health and Welfare have required these physicians to complete a three-hour on-site education program since 2017 to get certified, without this education widely available.16
Currently, only two dozen Korean physicians are considered geriatricians. In addition, only a few new geriatricians are graduating annually from Korean postgraduate geriatric medicine training programs.58
As in the U.S., there are a number of reasons why new Korean physicians do not choose to specialize in geriatric medicine. There are additional costs incurred with extra years of training, as well as the relatively low income compared with fields like surgery, cardiology or dermatology. The complicated nature of caring for older patients and their families may also discourage Korean medical students and residents from careers in geriatric medicine, especially if they are trained in environments that are not well equipped to deal with this population.17
However, there are many reasons why a new Korean physician should consider a career in geriatric medicine. These reasons do not differ from those in the U.S. Most importantly, geriatricians make a strong positive impact in the lives of older adult patients, as well as their family caregivers who are increasingly relied upon by the Korean healthcare system. The training provided by a geriatric medicine fellowship gives physicians the knowledge and skills to care for older adults with multiple complicated medical, psychological, and social problems. The fellows are also taught how to care for complex patients in a holistic, interdisciplinary, and system-based manner. Geriatricians learn strategies for fostering successful aging, how to manage progressive functional disability and care for those at the end of life.17
Geriatric medicine is also notable for its versatile career path. Geriatricians can practice in many different settings; including, academic medical centers, community hospitals, ambulatory care clinics, post-acute and long-term care (LTC) facilities, home care, and palliative care and hospice agencies. In addition, geriatricians can practice as a consultant, a primary care physician, or both. Geriatricians can also make valuable contributions as educators and researchers. This is a medical specialty that can provide many positive benefits for Korea, but adequate resources and mentorship must be developed for trainees to be attracted to and succeed in the specialty.
BARRIERS TO DEVELOPING AND IMPLEMENTING QUALITY GERIATRIC MEDICINE IN KOREA
There are many educational, organizational, and financial barriers to developing and implementing quality geriatric medicine in the Korean health care system (Table 1). First, more clinical expertise in comprehensive primary and specialty older adult care must be developed and maintained on a wide spread basis among individual Korean health care providers and across the continuum of care. The successful integration of training in geriatric medicine is imperative for all schools of health professions and primary care medical residencies, as well as developing more widespread and structured geriatric medicine fellowship programs. Certification as a geriatrician must also be made available to both new fellowship graduates and practicing family physicians and general internists.
Table 1
The importance of geriatric medicine and what barriers there are to it being a subspecialty in Korea

A second significant barrier concerns developing and implementing better incentives for expert older adult care in Korea. Physicians, hospitals, and health systems should receive better and more direct reimbursement for specialty older adult care by geriatricians and other health care providers. Specifically, reimbursement for the spectrum of specific geriatric conditions or syndromes must be enhanced given the complexity and time commitment required for this care.
A third notable challenge for Korea as it addresses the needs of its rapidly growing population of frail older adults will be the location of their care and death. Whereas in many parts of the world, the care of frail older adults is increasingly occurring in the clinic, at home and in nursing homes, approximately 26% of Korean older adults are primarily cared for in acute care hospitals.18 In addition to the ambulatory care clinic and home being an uncommon setting for the specialty care of older adults by geriatricians, LTC settings are also wholly underrepresented — despite a rapid increase in both the number of these facilities and their residents in recent years.1920 There were 357 nursing homes in Korea in 2004, which increased to 5,163 in 2016,21 LTC hospitals have also significantly increased, from 113 in 2004 to 1,428 in 2016.10 Therefore, it is imperative that Korean nursing homes and LTC hospitals prepare to take on the compelling mission as “specialty older adult providers.” However, the LTC health care professionals and facilities will not be ready to assume responsibility for this type of care until there are both significantly improved educational efforts and reimbursement focused on providing specialty older adult care across the continuum of care, including in LTC facilities.
Lastly and most importantly, the several Korean medical societies with significant interest in geriatric medicine are planning a geriatric medicine subspecialty individually and without a coordinated effort. While a geriatric medicine specialty program is under discussion by these medical societies in Korea, the lack of coordination and agreement by these academic societies will be very problematic for a successful development and implementation of this proposed new subspecialty. The competitive stance of these medical societies presents a very difficult conundrum to organizing geriatric medicine as a subspecialty in Korea.
ACHIEVING QUALITY SPECIALTY GERIATRIC CARE FOR OLDER KOREANS
A great challenge for providing widespread, quality older adult care in Korea is that the healthcare workforce is unprepared to provide this type of care.522 There are too few medical, nursing and social work providers trained to provide both quality primary and specialty older adult care.1020 Thus, there must be a significant focus on training all Korean medical, nursing, and social work students, as well as family medicine (FM) and general internal medicine (IM) resident physicians and current primary care providers, in geriatric care in order to provide high quality and easily accessible quality older adult care in the future. The training will need to be both profession-specific and in team-based care.
Developing geriatric competencies across the continuum of medical education
Medical schools
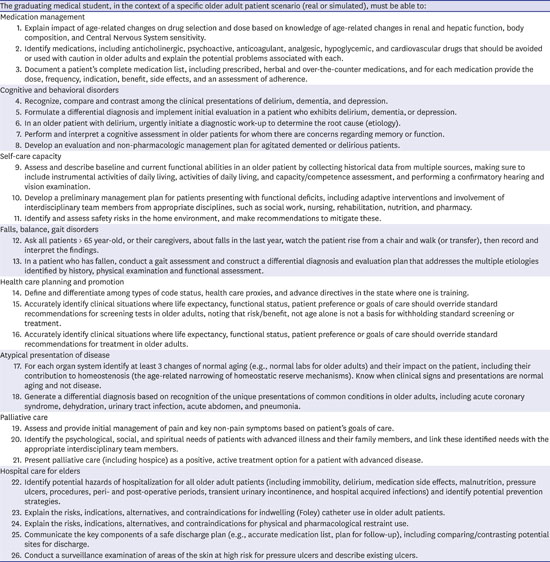
The U.S. has developed competencies for all medical students which could be adopted by Korean schools of medicine. In July 2007, the Association of American Medical Colleges (AAMC) and the John A. Hartford Foundation hosted a National Consensus Conference on Competencies in Geriatric Education where a consensus was reached on minimum competencies that graduating medical students needed to assure competent care by new interns to older patients.23 These twenty-six (26) Minimum Geriatric Competencies in eight content domains have been endorsed by the American Geriatrics Society (AGS), American Medical Association (AMA), and Association of Directors of Geriatric Academic Programs (ADGAP). As shown in Appendix 1, the domains are cognitive and behavioral disorders; medication management; self-care capacity; falls, balance, gait disorders; atypical presentation of disease; palliative care; hospital care for elders, and health care planning and promotion.23 Each content domain specifies three or more observable, measurable competencies. Requiring these competencies, or a similar set, to be achieved by all Korean medical students would be a significant advancement towards improving the primary care and specialty medical workforce to provide quality older adult care.
Primary care postgraduate geriatric medical education
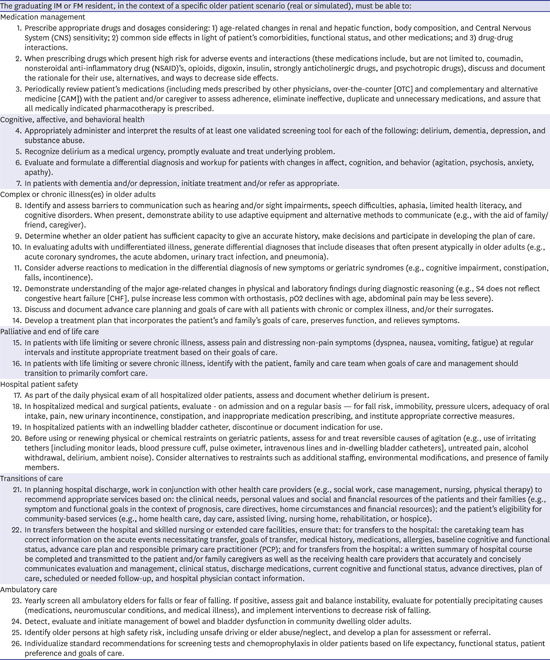
All FM and general IM residency training programs in the U.S. are required to provide specific training in the care of older adults since these physicians provide the majority of primary care for older adult Americans.2425 With only 7,300 geriatricians in the U.S., they are a scarce resource, with their role being to care for the frailer, more complex, and severely ill older adults, rather than those that are relatively healthy.26 This latter group of patients could be well cared for by primary care providers. However, for all American family physicians and general internists to be capable of providing quality primary care to older adults, they must attain specific competency in the care of these patients through their residency training and subsequent continuing education. Appendix 2, provides the competencies endorsed by the AGS, AMA, and ADGAP.27 However, the amount and quality of education is currently quite variable and dependent on the initiative and resources of each U.S. residency program. Thus, the training of the primary care physician workforce has been inadequate to meet the primary care needs of older adult Americans.28 This is an important lesson for Korea to consider as it structures its training of primary care physicians to care for the rapidly increasing number and frailty of its older adult population. This issue also has important implications for Korea's development of fellowships in geriatric medicine. Are these fellowships intended to train enough providers to care for the primary or specialty care needs of Korean older adults, or both?
Geriatric medicine fellowships
Globally, there are several models of specialty training to become a geriatrician. In the U.S., there are 151 institutions now offering formal fellowship training.29 Doctors of Medicine (MD) or Doctors of Osteopathic Medicine (DO) Physicians, who have completed residencies in either FM or IM, can train in any of these one-year clinical fellowships. It is important to note that the fellowships are sponsored both by Departments of Family Medicine and Internal Medicine, with the fellows being able to train in either type of department, regardless of their primary certifications. These fellowships offer the same fellowship training regardless of departmental sponsorship, which was designed to encourage cooperation between the two specialties in providing geriatric medicine training to as many physicians, as possible.
Certification has been available through the American Academies of Family Practice and Internal Medicine since 1988 as collaboration between their two certification boards.30 After acquiring the one year of additional training, family physicians obtain a Certificate of Added Qualifications (CAQ) in geriatric medicine, while internists receive a subspecialty certificate in geriatric medicine, by passing the same specialty examination. In the U.S., collaboration in providing geriatric medicine certification by these two boards was deemed important for the success of geriatric medicine as a specialty by recognizing the contribution of each primary care specialty to advancing expertise in the care of older adults. However, despite this collaboration, there are currently only 7,300 U.S. geriatricians, with the need being at least triple that number.26 The reasons for this significant shortfall in the geriatrician workforce in the U.S. have been previously described in this paper.
While in short supply, geriatricians in the U.S. serve an important role in providing primary and specialty care to older adults in ambulatory care clinics, hospitals, LTC facilities, at home, and through palliative and hospice care organizations. The model of care practiced by U.S. geriatricians is heavily focused on working closely with other disciplines such as nurses, pharmacists, therapists, and social workers to provide team-based care. This model of training is the focus of this paper and recommended for consideration by Korea.
Geriatric medicine training strategy for Korea
As a discipline, geriatric medicine in the U.S. has been fortunate to have received significant philanthropic and governmental funding over the last 4 decades, resulting in career development for clinician — educators, incorporation of geriatrics training into undergraduate and graduate medical education, and development of curricula and geriatric subgroups within many medical specialties.31 As a result, many educational materials have been produced and are freely available on curriculum websites such as the Portal of Geriatrics Online Education (www.pogoe.org).27 Nearly all U.S. medical students are now exposed, if not well grounded, in geriatric topics based on the twenty-six Minimum Geriatric Competencies.23 There are also now many well-trained medical educators with access to turn-key educational products, as well as specialty and subspecialty geriatrics champions.31 However, these efforts and resources have not translated into an increase in U.S. board-certified geriatricians, as previously cited in this paper.
Training needed to ensure competence in the primary care of older adult Koreans
Based on the U.S. experience with geriatric medicine, it is recommended that Korea adopt a systematic and comprehensive approach to training its primary care workforce in the care of older adults through a national curriculum. For example, the web-based Geriatrics Education Modules (web-GEMs) based on the 26 medical student competencies in geriatric medicine, is a readily available national on-line geriatrics curriculum.27 This curriculum, or a similar one, would provide a unifying and uniform foundation for educating medical students and resident physicians in FM and IM. However, these learners must also receive practical clinical training in order to become competent in the care of older adults. A predefined clinical skill set requires deliberate practice with observation and feedback by trained faculty in sufficient numbers.31 This must be done at every training site caring for older adults, so each site would need at least one skilled, experienced assessor. Thus, a cadre of geriatric medical educators must be developed in both the Korean schools of medicine and primary care residency programs in order to teach a defined set of core geriatric medicine competencies to their learners. It will be important for the learners to have onsite clinical preceptors who can role model the appropriate assessment and approach to older adult patients, as well as provide learner-specific feedback based on observation of the clinical care provided.
An important lesson concerning competency-based geriatric education of all medical students and primary care resident physicians can be gained from the U.S. experience. Korean medical education societies and regulators should require all learners achieve an agreed upon set of competencies, which would provide the greatest opportunity to reach the goal of excellent primary care for all Korean older adults. In contrast, the meaningful adoption of a set of geriatric medicine competencies by all U.S. medical schools and primary care residencies was merely recommended and not required by the national U.S. medical education societies and regulators. As a result, there has been a great deal of variability in both the quality and degree of implementation of the competencies across the schools of medicine and residencies, which does not portend well for widespread quality primary care of older Americans.
Faculty development of the needed Korean clinical preceptors could use train-the-trainer models and mini-fellowships to ensure general older adult clinical competency of the faculty across schools of medicine, primary care residencies, and practice sites. Every older adult clinical preceptor does not need to be a geriatrician. The schools of medicine and primary care residencies, aided by career development awards supported by their specialty societies and the Korean government, could develop a cadre of geriatric care champions who take responsibility for teaching their trainees how to best provide quality care to older adults. These geriatric care champions could be excellent role models in the care of older adults, as well as assessing and providing feedback to trainees in supervised geriatric care.31
As is the case in the U.S., busy Korean primary care physicians are responsible for providing care to the majority of older adults5 yet many received little specific geriatrics training. One effective model for training U.S. primary care physicians in practice has been the American Board of Post-Acute and Long-Term Medicine (formerly the certified Medical Director curriculum), which combines specific continuing education requirements and practical medical direction experience.32 Another way to reach practicing Korean primary care practitioners would be to adapt the web-GEMs curriculum to target practicing clinicians, who could complete web-based cases on their own time and earn Continuing Medical Education or Maintenance of Certification credit.31
THE IMPORTANCE OF A MID-CAREER TRANSITION TO CERTIFICATION AS A GERIATRICIAN
The pressing need to improve the care of older adults in the U.S., along with the modest number of U.S. geriatric medicine fellowship graduates, has led to an increasing emphasis on allowing mid-career family physicians and general internists to transition to become geriatricians through an alternate pathway of training.33 This arrangement should also be considered in Korea. Career options for dedicated U.S. physicians are plentiful in geriatric medicine; including, consultative hospital-based, ambulatory, post-acute and long-term, home, and palliative care opportunities. However, formal training and certification in geriatric medicine has been limited to the obligatory one-year fellowship for the past twenty years.26 While this certainly seemed to be the best option for recognition and professionalism of the specialty, it has left many mid-career family physicians and general internists without a formal pathway to desired training and certification. These physicians have provided care to many older adults as part of their practices and some would definitely be interested in better caring for older adults by transitioning solely to geriatric medicine as a career path.
In the U.S., fellowship training is believed to be the ideal route for obtaining the requisite skills to competently practice geriatric medicine.34 As a result, more U.S. geriatric medicine fellowship programs are offering a mid-career option that is affordable for well-established primary care physicians. The barrier has been economic for these physicians who would like to transition to provide older adult care full time as a certified geriatrician, but are usually at the height of their earning potential and responsible for the care and well-being of spouses and dependent children. Generally, they would have to reduce their salary to one fourth to one half of their usual income to train as a geriatrician, which is an economic hardship for most of them. As such, an affordable mid-career pathway for primary care physicians to certification as geriatricians is being provided through an enhanced subsidy, in addition to the usual salary of a geriatric medicine fellow, to these primary care providers. The providers might receive as much as twice the standard fellowship salary for the one year of training, which is usually about half of their salary as a family physician or general internist. More of these providers are finding this an attractive option for transitioning to becoming a geriatrician. After their one year of training, they resume about the same salary as they had as a primary care physician, but with many more opportunities and greater professional satisfaction as a geriatrician. The mid-career geriatric medicine fellowship-training pathway is becoming an increasingly important collaboration by U.S. universities, hospital systems and the government to increase the number of U.S. geriatricians.33
In addition, other alternate pathways to certification as a specialty geriatrician should be considered in Korea for mid-career primary care practitioners. Technological innovations could combine on-line content with intermittent in-person coaching, supervision, and assessment of competency.3133 For example, the American Board of Post-Acute and Long-Term Medicine model combines content in geriatrics, post-acute and LTC medicine, and palliative care with on-line and in-person clinical training through the Attending Physician Core Curriculum.32 As the move is made to competency-based training, it is likely that the amount of time in training will become less important. Long-distance methods of conducting clinical audits, as well as providing education and feedback can be used for nonresidential fellows, with them spending minimal time onsite at an accredited fellowship program.31 These types of programs in Korea could offer a flexible approach to attainment of the skill set needed to be a geriatrician, while drawing on the advantage of prior clinical experience caring for older adults as a family physician or general internist.
GERIATRIC MEDICINE FELLOWSHIP TRAINING
The curricular milestones (CM) for U.S. geriatric medicine fellows have become the foundation of geriatric medicine fellowship training.3536 They were developed to determine what every graduating geriatric fellow should be able to demonstrate to ensure that they will be able to practice effectively and safely in all care settings and with different older adult populations. Three major domains were identified: caring for the elderly patient, systems-based care for elder patients, and geriatric syndromes. These CM are intended to assist geriatric fellowship directors as they develop curricula and assess their fellows.
The geriatric medicine competencies were developed as part of the larger movement in the U.S. towards competency-based medical education (CBME) and training.35 In traditional medical education, the curriculum is developed based on faculty and institutional expertise and needs, with training activities designed around them. In CBME, the needs of the population and health system are considered, with learner outcomes identified that will assure high-level performance in the workplace.31 Once identified, these learner outcomes or CM are used to develop curricula and provide a road map for learners to gauge their progress and for faculty to assess their trainees. The geriatric medicine fellowship CM are specific and summative, with a focus on outcomes and performance to ensure that fellows are competent and ready for independent practice upon graduation.35
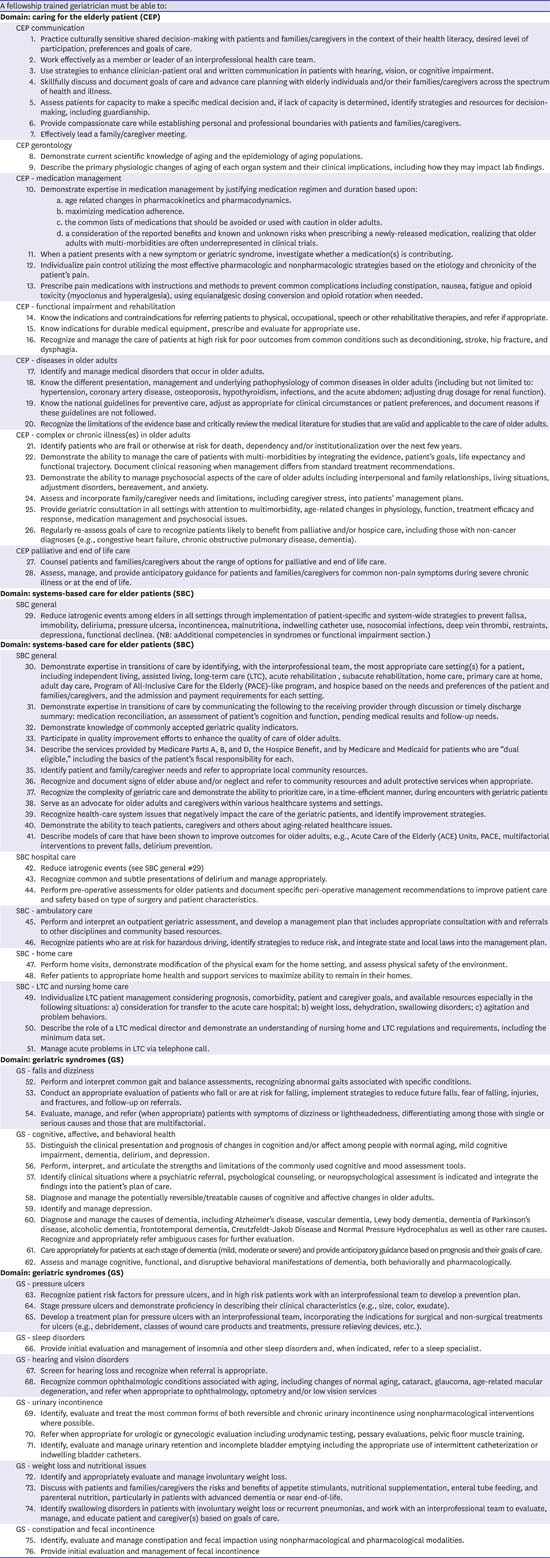
The geriatric medicine fellowship CM were designed to build on the medical student and the IM and FM residency competencies2327 and reflect the scope of practice of a geriatrician — able to practice in all settings and with all populations. It is assumed that competency in these CM can be attained by the completion of a 12-month Accreditation Council for Graduate Medical Education (ACGME)-accredited fellowship program. The CM for each fellowship are required to be behaviorally written and for faculty to able to assess them.35 The milestones fall into three domains, with 20 sub domains and a total of 76 geriatric CM are shown in Appendix 3.3536 The final set of 76 milestones has been endorsed by the ADGAP Board, AGS Board, and ADGAP/AGS Education Committee.
These AGS/ADGAP geriatric CM explicitly define the “product” of a geriatric fellowship.36 They are intended to assist fellowship programs as they develop curricula and assessments consonant with CBME. It is not expected that trainees will be assessed on each of the 76 CM. Rather, just as the National Board of Medical Examiners (NBME), the American Board of Internal Medicine (ABIM), and the American Board of Family Medicine (ABFM) test a sample of the entire content one is expected to learn in medical school or residency, the same is true for fellowship directors as they decide which CM they will formally assess.31
ENTRUSTABLE PROFESSIONAL ACTIVITIES (EPAS) FOR GERIATRICIANS
EPAs describe the core work that constitutes a discipline's specific expertise and provide the framework for fellowship faculty to perform meaningful assessment of U.S. geriatric medicine fellows.37 They are derived from the CM described in the previous section. The geriatrics EPAs describes a geriatrician's fundamental expertise and how geriatricians differ from general internists and family practitioners who care for older adults. They are critical, observable, measurable tasks and responsibilities that practicing specialists can be trusted to perform proficiently, consistently, and unsupervised by the end of their training.38
Beginning with the geriatric CMs, an AGS/ADGAP Geriatrics EPAs working group was formed in 2011 to develop a set of EPAs that represent the essence of the critical activities of geriatricians enumerated in the milestones.38 The working group drafted an initial list of EPAs and used an iterative process to garner input from clinical geriatricians, geriatric clinician-educators, and medical societies. Subsequently, The AGS and ADGAP boards approved the final list of 12 geriatrics EPAs in 2013.39
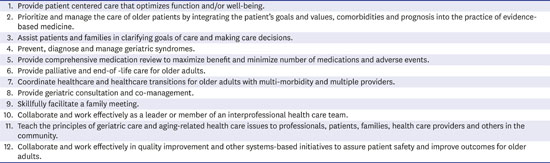
An expanded working group then developed overviews to describe each EPA from the observable tasks identified. The 12 EPAs for geriatrics, along with an overview and a description of the tasks that should be observed to determine that a physician can be entrusted to perform each EPA without supervision, are shown in Appendix 4.39 The EPAs highlight the activities that are the core of a geriatrician's practice. They encompass all of the geriatric CMs and all settings of geriatric care. The EPAs define the “product” of a geriatric fellowship — a physician prepared to care for older adults across all settings.38 Once in practice, individual geriatricians may choose to concentrate on specific EPAs or settings.
The EPAs emphasize the complexity of geriatric care and the greater likelihood of adverse events in those who are old, frail, or have multiple chronic conditions.38 Such complexity in turn requires prioritizing care with the individual and family and recognizing that the evidence is often insufficient and the individual's life expectancy uncertain.31 The EPAs recognize the need for fellows to become skilled communicators with patients, other physicians, and the healthcare team. They underscore that geriatrics is truly personalized and individualized medicine that recognizes good quality of life as one of the most important outcomes for patients.3138
CLOSING
As the average age of Koreans rises, it behooves the Korean schools of medicine, postgraduate residencies, medical societies and government to strive to meet three critical care needs for their older adults. First, they need both enough primary care providers competent to care for most of the older adults through primary care, as well as enough well-trained medical and surgical care providers to provide their specialty care needs. Second, specialty geriatricians are needed to provide care for the most-complex and frailest older adults; such as those with dementia and individuals with complex multi-morbidity. Finally, the healthcare system must embrace person-centered and team-based care, both optimizing personal goals and minimizing iatrogenic harm for older adults.31
No matter what the format of training is or who the trainees are, the teaching of geriatrics in Korea should always be centered on compassionate care of older adults experiencing the burdens of disease and disability, as well as supporting their caregivers. It should also rely on clinical decision-making amidst “subtlety and complexity,” which requires modeling by master clinicians and educators.31 By taking the essential undergraduate, residency and fellowship geriatric medical education curricula that has been identified in the U.S. and determining what can be offered in creative and broadly available ways in Korea, it may be possible to marry technology with “hands on” teaching and assessment for future generations of primary care and specialty providers of older adults and improve the care of all older adult Koreans. In addition, formally establishing uniform geriatric medicine fellowships and certification in Korea will be needed to develop a cadre of expert geriatric medicine clinicians, educators, researchers and policy-makers. Through these efforts, widespread and quality geriatric medicine can be developed and implemented in the Korean health care system.
 XML Download
XML Download