

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Preterm delivery, defined as a delivery occurring at less than 37 complete weeks of gestation, is the leading cause of infant morbidity and mortality.123 The incidence of preterm birth is currently about 10%; and the recent incidence of preterm delivery has gradually increased, likely due an increase in iatrogenic preterm births.14 Preterm labor is generally known to be a complex syndrome induced by multiple mechanisms, such as inflammation, uteroplacental hemorrhage, uterine overdistension, and other stressful environmental stimuli.5 Although, obvious cause cannot be identified in most cases, it is believed that multiple factors create a synergic effect.
Preterm delivery is known to be the most important risk factor for preterm birth in a subsequent pregnancy.6 However, in a population-based study, a history of preterm birth could predict only 10% of the preterm delivery in the consecutive pregnancy.7 Similarly, a preterm birth has a low attributable risk for a subsequent preterm birth; the risk of preterm births was three-fold higher following a previous preterm birth, and six-fold higher following two previous preterm births.8 In practice physicians should consult with third pregnant women for the risk of preterm delivery who had experienced preterm birth once or twice. Nevertheless, little is known about the recurrence rates of a preterm birth in a third or more pregnancy for mothers with a history a preterm delivery more than once before.
Multifetal gestations have been reported to comprise 15% to 20% of all preterm births though they account for only 2% to 3% of newborns.6 Twin pregnancies have been associated with numerous risks such as preeclampsia, placental abruption, gestational diabetes, and preterm birth.910 Although the incidence of twin pregnancies has been rising in most developed countries, there are still controversies about the interrelationship between singleton preterm births and twin preterm births.7111213
Defining the recurrence risk of preterm birth is important in order to determine risk-specific treatment and provide insights about mechanisms of preterm births.14 We aimed to evaluate the recurrence risk of premature births for subsequent pregnancies including third pregnancy as well as second pregnancy among women with a history of a preterm birth.
METHODS
Health care delivery system in Korea
Information on pregnancy and birth was obtained by linking the Korea National Health Insurance (KNHI) claims database and data from a national health-screening program for infants and children. The KNHI claims database has been mentioned in other studies.15
Almost all Koreans are covered by the health insurance policies of the KNHI, except for 3% of the population which are covered by the Medical Aid Program. Thus, the KNHI claims database contains information on all claims for approximately 50 million Koreans, and nearly all information about the extent of disease can be obtained from this centralized database, except procedures not covered by insurance, such as cosmetic surgery. The database contains information on the incidence of almost all diseases occurring in Korea. Using the KNHI claims database, all mothers who delivered between January 1, 2007 and December 31, 2014 were identified and the detailed information such as primiparity vs. multiparity, and singleton vs, multiple pregnancy were confirmed.
As a part of the National Health Insurance Corporation (NHIC) health-care system, a national health-screening program for infants and children, for which children aged 4 to 80 months are eligible, began in 2007 and is composed of seven consecutive health exams according to age groups (4–9, 9–18, 18–30, 30–42, 42–54, 54–66, and 66–80 months). The national health-screening program consists of history taking, physical examination, anthropometric examination, developmental screening, visual acuity, anticipatory guidance, and oral examination based on the child's age at the time of the visit. Using a data from a national health-screening program for infants and children, gestational age (GA) at birth was identified.
The rate of preterm birth in the third pregnancy was the primary outcome of interest and was analyzed in relation to the outcome in the previous two pregnancies. The secondary outcome was the recurrence risk of preterm birth including both singleton and twin pregnancy. In addition, we set the cut-off of GA as before 37 and 34 weeks and analyzed the risk of recurrence in each preterm birth.
Study population
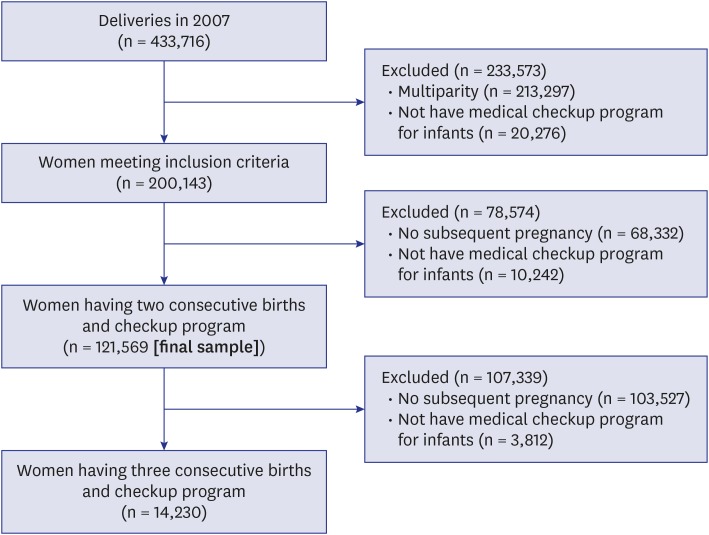
Fig. 1 illustrates the inclusion and exclusion criteria of the study participants. We identified all women who had their first delivery between January 1, 2007 and December 31, 2007 and a subsequent delivery before 2014. A total of 433,716 women who had deliveries in 2007 were identified. Of these, 213,297 women were excluded because of multiparity; 20,276 women were excluded because they did not follow a medical checkup program for their infants. There were 200,143 women who met the inclusion criteria and of these, 68,332 women did not have a subsequent pregnancy and 10,242 women did not follow a medical checkup program for their infants; thus, a total of 121,569 women satisfied the inclusion criteria of having two consecutive births with children followed by subsequent checkup program. Of these, 14,230 women were selected for analyzing third pregnancy and also they underwent a medical checkup program for their infants. Preterm birth was defined as delivery at < 34 or < 37 weeks of gestation and was derived from databases of the national health-screening program for infants and children.
Statistical analysis
The Student's t-test was used to compare the continuous variables between groups and the categorical variables were compared using the χ2 test. A multivariate logistic regression analysis was performed to evaluate the risk of preterm delivery in a subsequent pregnancy as the final result for the entire study population. Statistical significance was defined as having P value < 0.05. Statistical analysis was performed using SPSS software version 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
In women with two consecutive singleton pregnancies, the risk of a subsequent preterm birth at < 37 weeks and < 34 weeks of gestation is shown in Table 1. Of the 117, 067 women who had a term delivery at ≥ 37 weeks, 2,525 women (2.2%) had a subsequent preterm birth, and of the 2,994 women who had a preterm delivery at < 37 weeks, 558 women (18.6%) had a subsequent preterm birth. As expected, the delivery of preterm singleton birth was associated with a significantly higher risk of preterm birth in a subsequent singleton pregnancy (relative risks [RR], 8.64; 95% confidence interval [CI], 7.94–9.40).
Table 1
Recurrence risk of preterm birth in singleton pregnancy

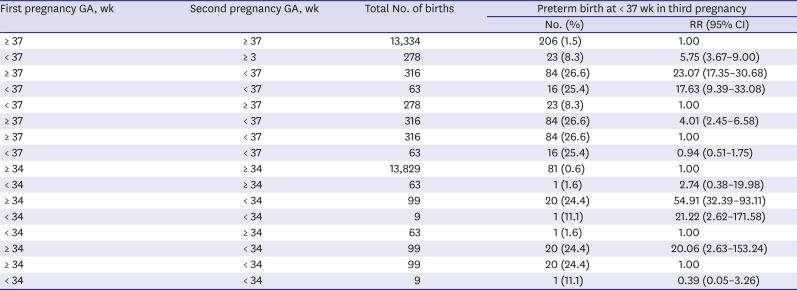
We then investigated the subsequent preterm birth risk of a singleton birth in a third pregnancy, stratified into four categories based upon the mothers' previous two pregnancy delivery outcomes, i.e., at either 37 weeks (i.e. ≥ 37 or < 37) or 34 weeks (≥ 34 or < 34) gestation (Table 2). Compared to women who delivered a term birth first followed by preterm birth with women who delivered a preterm birth first followed by term birth, the history of the pregnancy preceding preterm birth delivery was the most relevant factor for the recurrence of a preterm delivery in a subsequent pregnancy (cut-off 37 weeks: RR, 4.01; 95% CI, 2.45–6.58, cut-off 34 weeks: RR, 20.06; 95% CI, 2.63–153.24; Table 2). Among women with a history of preterm delivery in the second pregnancy, there was no significant difference in outcome of the third pregnancy based on whether or not their first pregnancy was preterm (cut-off 37 weeks: RR, 0.94; 95% CI, 0.51–1.75, cut-off 34 weeks: RR, 0.39; 95% CI, 0.05–3.26).
Table 2
RR for recurrent delivery less than 37 and 34 weeks in the third pregnancy according to the outcome of previous delivery
Of the 307 women who delivered term twins (after ≥ 37 weeks gestation) at the first pregnancy, 4 women (1.3%) had a preterm birth in the subsequent singleton pregnancy; and of the 168 women who delivered preterm twins at the first pregnancy, 6 women (3.6%) had a subsequent preterm birth. Therefore, birth history of preterm twins in first pregnancy did not affect the risk of preterm birth in subsequent singleton pregnancy (RR, 2.81; 95% CI, 0.78–10.09; Table 3).
Table 3
Risk of recurrent preterm birth by the number of fetus

Of the 965 women who had delivered a term singleton (≥ 37 weeks gestation) at first pregnancy, 302 (31.3%) had a preterm birth with a subsequent twin pregnancy, and of the 28 women who had delivered preterm singleton at first pregnancy, 16 (57.1%) had a subsequent preterm twin birth. Different from the effect of history of twin pregnancy, a delivery of a preterm singleton was significantly associated with the risk of a subsequent preterm twin pregnancy (RR, 2.93; 95% CI, 1.37–6.24; Table 3).
DISCUSSION
We evaluated the risk of recurrence of preterm delivery in women with a history of preterm delivery in singleton and twin pregnancies. Our data showed that the recurrence rate of a preterm birth in a third pregnancy among singletons was more closely associated with women having a history of preterm birth in the second pregnancy rather than in the first pregnancy. When we defined the GA of preterm birth at < 34 weeks, the results were more remarkable.
Furthermore, we found that the preterm delivery of twins was not associated with a recurrence of preterm delivery in a subsequent singleton pregnancy, whereas the preterm delivery of a singleton was associated with a significantly increased risk of preterm delivery in a subsequent twin pregnancy. It is widely known that the rate of preterm births is higher in women who have had a prior history of a preterm birth among singleton deliveries.816 Little is known about the recurrence rates of preterm birth in a third pregnancy. Therefore, we focused our attention on the comparison of women who had delivered a first preterm birth followed by second term birth and women who had a first term birth followed by second preterm birth. Carr-Hill and Hall8 analyzed the rates of previous preterm deliveries on the third birth outcome. The authors compared 214 women, who had delivered a preterm birth, either on their first or second pregnancy. The RR of a recurrent preterm birth compared to a single preterm birth was 5.0 in women whose first pregnancy outcome was a term birth and the second was a preterm birth; instead, a RR of 2.6 was reported for women who had had a preterm birth on the first pregnancy followed by a term birth on the second pregnancy. However, the differences in each group were not statistically significant due to the small number of women satisfying these criteria in the study.
We identified that the recurrence risk of preterm delivery at third pregnancy was not significantly different between women with one preterm births at second pregnancy and two consecutive preterm births, which was inconsistent with previous study.7 We suggest the following possible hypotheses for why a preterm birth on a first pregnancy did not affect the risk of a preterm birth on a third pregnancy, while a preterm birth on a second pregnancy did. First, a short interpregnancy interval may have increased the recurrence rate of a preterm birth in the subsequent pregnancy. Women who have delivered a preterm birth usually tend to wait a shorter time before the next pregnancy.6 Although we did not consider the interpregnancy interval as a compounding factor, this tendency might exist in our study group. The uterus needs sufficient time to recover to its pre-pregnancy state, however it cannot make a sufficient recovery of inflammatory uterine nor can it return the enhanced contraction-related proteins to normal range if the pregnancies interval is too short.1718 Second, residual or recurrent infections of the uterus that had caused the preterm delivery in the preceding pregnancy could also likely explain these results.19 Whereas a previous infectious status may have recovered completely in women who delivered preterm birth on a first pregnancy and then term birth in second pregnancy, those women who also delivered a preterm birth on the second pregnancy may still have had an underlying unresolved uterine infection.
Our findings also suggest that women whose first singleton birth was preterm were more likely to deliver a subsequent preterm birth of twins, although women whose first delivery consisted of preterm twins showed no correlation with a subsequent preterm singleton birth. Our results are in close agreement with previous studies showing a correlation between a previous singleton preterm birth and the rate of subsequent twin term births. Schaaf et al.13 investigated 4,071 nulliparous women with a singleton delivery followed by a subsequent twin delivery. The RR for preterm birth in the subsequent twin birth was 5.0 (95% CI, 3.8–6.6) for women with a preterm singleton delivery compared with women with a term singleton delivery. Our results are also consistent with those presented by Ananth et al.,20 who investigated 2,329 women with a first singleton birth followed by a twin birth in the second pregnancy. The hazard ratio for preterm birth in the twin pregnancy was 1.8 (95% CI, 1.6–2.1). Our result indicating that a previous singleton preterm birth might increase the risk of a subsequent twin preterm birth was inconsistent with only one previous study.21 However, this previous study showed a lack of precision, due to the few women examined and the statistical analysis resulted to be not significant (P = 0.52).
We also found that a twin preterm delivery was not associated with an increased risk of a preterm birth of a subsequent singleton infant. Rydhstroem21 concluded that a history of preterm twin births (28–30, 31–33, or 34–36 weeks gestation) was not significantly associated with the risk of a subsequent singleton preterm birth (χ2 = 3.4, P > 0.05). In another similar study, the authors also concluded that a previous twin preterm birth (< 35 weeks gestation) did not enhance the recurrent preterm birth rate for a subsequent singleton pregnancy (RR, 1.9; 95% CI, 0.46–8.14).7 However, the authors did not confine their analysis to a twin preterm birth group compared to a nulliparous group; thus they could not exclude any potential contributing factors, such as gestational number. In contrast to these reports, a conclusion similar to that of our study was reported by Schaaf et al.12 who investigated 1,057 women (55%) who delivered preterm twin versus 882 women (45%) with term deliveries. The RR for a preterm birth in the subsequent singleton pregnancy was 6.9 (95% CI, 3.1–15.2). Although they analyzed their results by distinguishing iatrogenic and spontaneous preterm twin birth rates, they also demonstrated that there was an increased risk of subsequent single preterm birth in both iatrogenic and spontaneous preterm deliveries. This study was based only in the Netherlands; therefore, the conclusions may not be generalizable to other populations. Our results are also inconsistent with those of Menard et al.22 who investigated 144 women that delivered twin preterm births followed by a singleton birth; and inconsistent with the study by Facco et al.11 who investigated a similar group of 167 women. These studies concluded that women with a previous twin preterm birth had an increased risk of preterm birth in a subsequent singleton pregnancy (RR, 2.87; 95% CI, 1.02–8.09 and RR, 5.0; 95% CI, 1.1–22.9, respectively). However, some of the women who participated in the study by Menard et al.22 could be considered to have had an amplified higher risk of preterm birth rate because they may have had a preterm birth before being enrolled as subject with a twin pregnancy.
Pathophysiological processes involved in preterm births have been known to differ between singleton and twin pregnancies. Among singleton preterm births, infections and the inflammation of the uterus are known to be important mechanisms inducing preterm labor.23 With regards to twin pregnancies, mechanical stretching or overdistension of smooth muscle cells in the uterus may have an important role in increasing the expression of oxytocin receptors and interleukin-8 that are associated with the onset of labor.24 In the case of a twin pregnancy, a significantly overdistended uterus could implicate the preterm premature rupture of membranes (PPROM) and the onset of preterm contractions.5 In most subsequent singleton pregnancies occurring after a preterm twin birth, a less distended uterus, compared to that of the prior overdistended uterus caused by a term twin pregnancy, was believed not to result in an increased risk of a preterm birth in the subsequent singleton pregnancy. In contrast, we have demonstrated that there is an increased risk of preterm birth in a twin pregnancy following a singleton preterm birth. A previous history of a twin pregnancy per se is considered to be a risk factor for a subsequent preterm birth.10 This increased risk of a preterm birth for a twin pregnancy can be further compounded if these women also had a previous history of a singleton preterm delivery because of a combination of complex mechanisms involved in this syndrome. Recurrent or untreated intrauterine infections probably explain some of this heightened risk.25
Readers should be aware of the several limitations of the present study. Our database was based on the medical check-up program for infants in Korea, which contains large amounts of population-based information. Unfortunately, we did not distinguish an iatrogenic preterm birth group from a spontaneous preterm birth group. Combining iatrogenic and spontaneous preterm deliveries might lead confounded conclusions. Furthermore, we did not consider compounding factors, such as tobacco use, the level of education, the body mass index, interpregnancy interval, a history of conization, the cervical length, the use of progesterone, and a history of cervical cerclage, all of which have been known to increase the risk of preterm birth.17262728 Nevertheless, our data would be useful for women currently pregnant who have a history of preterm birth, as our results are based on the largest sample size reported to date. Moreover, we have also excluded all women with a history of a previous pregnancy at the start of our database query, in order to prevent any potential confounding influence on our results.
Clarifying the recurrence risks of preterm birth in women with a history of preterm birth is of interest when selecting pregnant women who are at high-risk and may require prophylactic treatment. Unfortunately, there are numerous causes for preterm deliveries; thus, our data regarding recurrence risks rates for preterm births may aid in the counseling of pregnant women about the potential risks involved in a recurrent preterm birth, whether it be a singleton or twin pregnancy. Furthermore, our results might be helpful to design future studies focusing on preterm births.
 XML Download
XML Download