

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Prostate biopsy is a standard technique in prostate cancer diagnosis.123 Each year, several million prostate biopsies are taken around the world.12 Although transrectal prostate biopsy (TRPB) is well-known and safe, a certain population among the biopsied develop various acute complications within a week of biopsy.1234 The clinical significance of acute bacterial prostatitis (ABP) infection has been well evaluated, allowing clinicians to evade potentially severe infections.12345 However, lesser serious complications that are easily overlooked are still reported until 5 weeks following prostate biopsy.56
Although the pathogenesis for ABP after TRPB is not clearly defined, the main mechanism is likely direct inoculation of bacteria from rectal mucosa into the prostate tissue through inserted biopsy needles.1237 Generally, acute infection in internal organs can be initially induced by the direct inoculation of pathogens from the external environment. Furthermore, chronic infections may also be established after a single episode of acute infection or by pathogens that may have invaded through cracks or unsealed tracts in barrier layers. Indeed, a Korean group had reported that ABP had developed in 2.0% cases of post-prostate biopsy; 72.2% of cases had specific pathogens that may have originated from rectal mucosa.8 Additionally, some patients with ABP do not fully recover; 1.3% of ABP cases progress into chronic bacterial prostatitis (CBP) and 10.5% into inflammatory chronic prostatitis.9 Therefore, in certain patients, even a single episode of ABP may not be completely eradicated with prescribed antimicrobials, further progressing to CBP. Likewise, some pathogens from biopsy-associated ABP may still survive in the prostate and eventually progress into CBP.
Hypothetically, the biopsied prostates could be susceptible to infection in certain periods after TRPB, and those who had their prostate biopsied may end up with CBP or chronic inflammatory prostatitis during the follow-up period. Nevertheless, the relationship between post-TRPB infection and CBP has yet been clarified. Therefore, to detect the bacterial infection in the biopsied prostate after TRPB, we examined bacteria-free pre-biopsied prostates for the presence of new bacterial infection associated with TRPB using a modified 4 glass test. We also evaluated clinical characteristics in men with new bacterial infection in the prostate after TRPB and estimated the clinical significance of the infection.
METHODS
Study design and the participant characteristics
Three hundred seven men visiting the prostate clinic in Dankook University Hospital from September 2010 to November 2017 were selected for this study. Repeated prostate biopsy cases were excluded before the selection. They had been referred from primary practitioners because of either elevated serum prostate-specific antigen (PSA) levels or presence of palpable prostate nodule. The prostates from all men attending the clinic were sequentially evaluated with serum PSA, Korean version of the National Institutes of Health-Chronic Prostatitis Symptom Index (NIH-CPSI) questionnaire, white blood cell (WBC) counts and an ordinary culture with a pre-massaged voided urine specimen, digital rectal examination (DRE), and WBC counts and an ordinary culture with an expressed prostatic secretion (EPS) specimen.
One or 2 weeks after the initial evaluation, they underwent TRPB according to the Korean guideline for prostate biopsy. One hundred thirty men were diagnosed with prostate cancer and were excluded from this study. The remaining 177 men with benign prostate pathology in the biopsy specimens were followed for detecting missed prostate cancer. During the follow-ups, 11 men underwent transurethral resection of the prostate due to acute urinary retention (AUR) or severe obstructive voiding symptoms, and 53 cases were lost or refused the repeated lower urinary localization study through the EPS procedure. Therefore, these 64 men were excluded from this study.
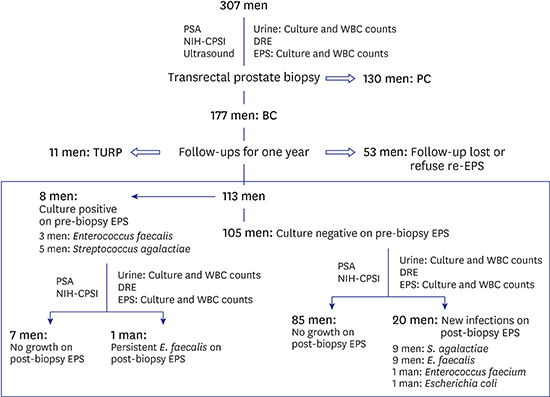
The remaining 113 men underwent one repeated EPS culture within one year of the TRPB. From them, 8 men were excluded from this study because they already harbored bacteria in the prostate in the pre-biopsy EPS culture. Finally, we enrolled the remaining 105 men with bacteria-free prostates to investigate whether TRPB could lead to new the bacterial infections, consistent with the purpose of the study (Fig. 1).
Fig. 1
Schematic drawing of the study design. Three hundred seven men underwent basic prostate cancer evaluation tests including lower urinary localization test before TRPB. One or 2 weeks later, they underwent TRPB with prophylactic fluoroquinolones coverage. From pathologic reports, 177 men were diagnosed with BC, while 130 men with PC. All men with histological BC were strongly recommended to be prospectively and clinically followed up for one year for detecting missed PC. During that follow-up, 113 men underwent the repeated basic PC evaluation tests as the previous tests. From them, 8 men revealed presence of bacteria in the prostate on pre-biopsy EPS. Of the remaining bacteria-free men, 20 men revealed new bacterial infections in their prostates after TRPB.
TRPB = transrectal prostate biopsy, PSA = prostate-specific antigen, WBC = white blood cell, NIH-CPSI = National Institutes of Health-Chronic Prostatitis Symptom Index, DRE = digital rectal examination, EPS = expressed prostatic secretion, PC = prostate cancer, BC = benign prostate condition, TURP = transurethral resection of prostate.

Clinical information, including the participant's age and patient-specific risk factors for biopsy-related infectious complications were collected from the individuals; recent history of AUR and fluoroquinolone exposure were also considered as risk factors, as well as the presence of diabetes mellitus.
Lower urinary tract localization tests
All participants had discontinued antimicrobial administration 4 weeks prior to the localization test. Culture specimens for diagnosing bacterial infection in the prostate were obtained by using a modified Meares-Stamey method.10 Each pre-massaged urine and the matching EPS samples were sequentially collected and incubated aerobically onto plates containing 5% sheep blood agar for 2 days. To be considered as bacterial infection, the concentration of bacterial colony in EPS specimens was to be increased at least 10-fold compared to the concentration of colonies in the pre-massaged urine specimen.10
WBC counts in voided urine and EPS
The pre-massaged urine samples were delivered to the central laboratory office for automatic urine analysis with Sysmex UF-1000i (TOA Medical Electronics, Kobe, Japan). EPS was collected by digital rectal massage into a sterile 1.5-mL tube. Using a micropipette, 5 µL of the collected EPS were placed on a glass slide and covered with a 22-mm2 No. 1 cover glass. The slide was then examined with a model BX40F microscope (Olympus, Tokyo, Japan) by one urologist (GL). We counted the dispersed WBCs in at least 15 fields and averaged them to determine the mean WBC count per high power field (HPF). The results of the WBC counts in the EPS were classified into 3 categories: 0–4, 5–15, and ≥ 16 WBCs per HPF.11
Serum PSA, prostate volume, and PSA density
Serum PSA levels were determined with a PSA kit (PSA-RIACT; CIS Bio International, Gif Sur Yvette, France). Prostate volume was determined through a transrectal ultrasound (HD7 Ultrasound System; Philips, Chenyang, China). The PSA density was defined by the ratio of the pre-biopsy serum PSA level to the matching prostate volume determined by the transrectal ultrasound.12
Procedures for prostate biopsy
Oral fluoroquinolones were prescribed from the day of TRPB as an antimicrobial prophylaxis for 5–7 days. Additionally, all men underwent cleansing enema prior to biopsy. Under local anesthesia, participants underwent ultrasound guided 12 to 14 core TRPB on an outpatient basis.
Follow-ups to benign prostate pathology in the biopsied specimens
According to the pathologic results from TRPB, men with benign prostate pathology were strongly recommended with one more follow-up within a year of the initial TRPB. Similar to their initial visits, men underwent one repeated serum PSA, DRE, NIH-CPSI questionnaire, as well as lower urinary tract localization tests in follow-ups.
Statistical methods
We used nonparametric Mann-Whitney U test to evaluate the difference in the ordinal scores in a Korean version of the NIH-CPSI questionnaire. Student's t-test for continuous variables was used for association studies. Pearson χ2 test and Fisher's exact test were used to evaluate the difference in categorical data. Wilcoxon signed-ranks test and McNemar test were used to compare the changes in clinical characteristics between the pre- and post-TRPB. Two-sided null hypotheses of no difference were rejected if P values were less than 0.05. All analyses were performed using SPSS software for Windows, version 23 (SPSS Inc., Chicago, IL, USA).
RESULTS
During this study, we did not find any case of TRPB associated ABP in the enrolled 113 men (Fig. 1).
Among 105 men that were initially negative for bacterial infection in the prostate prior to TRPB, 20 men acquired new bacterial infections within one year after TRPB. Of the 20 men, 9 had Streptococcus agalactiae infections, 9 had Enterococcus faecalis infections, and the other 2 had Enterococcus faecium and Escherichia coli, respectively (Fig. 1).
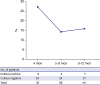
The mean follow-up period ± standard deviation (in months) for the 105 men was 7.68 ± 3.18 months (4–12 months). Splitting the samples into a culture-positive group and culture-negative group yielded non-significant difference in follow-up period (7.05 ± 3.24 months, 7.84 ± 3.17 months, respectively; P = 0.323). New bacterial infection rates during the follow-ups after the TRPB were 27.3% (9 in 33 cases) in 4 months, 14.3% (4 in 28 cases) in 5–8 months, and 15.9% (7 in 44 cases) in 9–12 months (P = 0.343) (Fig. 2).
Fig. 2
New bacterial infection rates after TRPB. Within one-year follow-ups after TRPB, new bacterial infection in the prostate occurred in 27.3% of the cases (9 in 33 cases) in 4 months, 14.3% (4 in 28 cases) in 5–8 months, and 15.9% (7 in 44 cases) in 9–12 months.
TRPB = transrectal prostate biopsy.
We could not find any significant differences in pre-biopsy characteristics between the culture-positive and negative groups, including mean age (60.90 ± 10.89 years vs. 62.88 ± 8.89 years, P = 0.393), serum PSA level (9.54 ± 5.70 vs. 7.89 ± 5.60 ng/mL, P = 0.240), prostate volume (47.65 ± 28.42 mL vs. 47.41 ± 21.08 mL, P = 0.966), PSA density (0.22 ± 0.12 ng/mL/cc vs. 0.20 ± 0.24 ng/mL/cc, P = 0.714), and the sum of pain or discomfort domain in the NIH-CPSI questionnaire (1.95 ± 3.80 vs. 2.09 ± 3.54, P = 0.606) (Table 1). In addition, there were no significant differences in WBC counts in the pre-massaged urine and the EPS specimen between the two groups. Furthermore, the well-known infectious risk factors for ABP after TRPB were also not significantly different in this study. Similar to the pre-biopsy characteristics, the post-biopsy serum PSA level and post-biopsy sum of pain domain in NIH-CPSI were not different between the two groups (Table 1).
Table 1
Clinical characteristics between the culture-positive and the negative groups in the prostate through lower urinary localization test after TRPB

TRPB = transrectal prostate biopsy, SD = standard deviation, PSA = prostate-specific antigen, NIH-CPSI = National Institutes of Health-Chronic Prostatitis Symptom Index, WBC = white blood cell, EPS = expressed prostatic secretion, HPF = high power field, AUR = acute urinary retention.
aNonparametric Mann-Whitney U analysis; bFisher's exact test.
The TRPB procedure increased post-biopsy WBC counts in EPS when compared with the pre-biopsy WBC counts in EPS (P = 0.031, McNemar test) in the 20 culture-positive men. The biopsy process, however, did not increase the serum PSA levels (9.54 ± 5.70 ng/mL in pre-biopsy vs. 9.63 ± 8.08 ng/mL in post-biopsy, P = 0.960) and the sum of pain domain in the NIH-CPSI questionnaire (1.95 ± 3.80 vs. 1.80 ± 2.95, P = 0.759) (Table 2).
Table 2
Changes in clinical characteristics in 20 patients who acquired new bacterial infection in the prostate after TRPB

TRPB = transrectal prostate biopsy, PSA = prostate-specific antigen, NIH-CPSI = National Institutes of Health-Chronic Prostatitis Symptom Index, WBC = white blood cell, EPS = expressed prostatic secretion, HPF = high power field.
aWilcoxon-signed ranks test and bMcNemar test were used for comparing the changes of clinical characteristics between the pre- and post-TRPB.
DISCUSSION
Generally, only 5%–10% of men with symptoms of chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) have CBP by the lower urinary tract localization test.10 Our study also revealed a similar result; 8 of 113 men (7.08%) already had bacterial infections in the prostate before the TRPB procedure (Fig. 1). The biopsy associated new bacterial infection in the prostate (19.05%; 20 out of 105 men) after TRPB might be too high an estimate of incidental occurrence when compared with general incidence of CBP in CP/CPPS patients.10 Furthermore, higher bacterial infection rate, 27.3% (9 in 33 cases), in the early follow-up period after biopsy strongly suggests that new bacterial infection might have occurred after the TRPB procedure (Fig. 2). In addition, newly infected prostates revealed increased WBC counts in the post-biopsy EPS specimen, suggesting bacteria associated chronic prostate inflammation (Table 2).
The prostate harbors multiple bacteria.13 Furthermore, acute inflammatory reactions may be induced in the prostate through interactions between the host and exogenous bacteria.14
TRPB-related ABP is routinely reported after execution of TRPB, and the clinical characteristics of ABP are relatively well documented around the world.1234567815 From the patient's blood or urine specimens, gram-negative pathogens such as E. coli are often isolated. The isolated E. coli strains frequently exhibit high rates of fluoroquinolone resistance and sometimes even resistance to multiple drugs.1234 A probable mechanism for ABP is the inoculation of fluoroquinolone resistant bacteria from rectal mucosa to the biopsied prostate that were not completely eradicated with empirical fluoroquinolone prophylaxis during the TRPB procedure.
Alternative route of ABP also includes infections by uropathogens through the ascending route.916 ABP without prior history of TRPB can progress into CBP or chronic inflammatory prostatitis.9 Similar to patients with ABP without biopsy, some patients with post-biopsy ABP may develop CBP or chronic prostatitis. Furthermore, in contrast to ABP, some cases of CBP present mild or atypical clinical symptoms with stable serum PSA levels.17 Therefore, mild symptomatic CBP patients post-TRPB may be unexposed, easily forget symptoms, or not be tested for CBP.
We found that the TRPB procedures are potentially associated with new bacterial infection in the biopsied prostate within one year of biopsy. Interestingly, there were no differences in the assumed biopsy-related risk factors between the culture-positive and negative groups.
We found that mean age, serum PSA level, prostate volume, PSA density, and sum of pain or discomfort domain in the NIH-CPSI questionnaire in pre-biopsy characteristics were not significant risk factors for new bacterial infection in the prostate after TRPB (Table 1). In addition, recent exposure of fluoroquinolones and history of AUR were also not related with the occurrence of post-biopsied bacterial infection in the prostate, as well as cases of diabetes mellitus. Furthermore, WBC counts in the EPS during pre-biopsy were not associated with new bacterial infection in the prostate within one year of TRPB, suggesting that inflammatory prostatitis was unlikely to be a risk factor for acquiring new bacterial infection in the prostate after TRPB (Table 1).
Except for one gram-negative bacterium, the cultured pathogens were mostly gram-positive bacteria. S. agalactiae, E. faecalis, and E. faecium are gram-positive bacteria that commonly inhabit the genitourinary and gastrointestinal tracts.1819 Although they are commensal in the gastrointestinal tracts, these bacteria can sometimes cause life-threatening infections in human.1819 The detection of these bacteria in the biopsied prostate is somewhat anticipated because these newly found bacteria in the prostate may have transferred during the TRPB procedure or its related complications. In contrast to antibiotic-resistant profiles of bacteria from biopsy related ABP, all isolates of S. agalactiae and E. faecalis in this study revealed fluoroquinolone-sensitive characteristic.1234
Eight men were excluded during the pre-enroll phase because they already had bacterial localization in the pre-biopsy EPS cultures. All 8 gram-positive bacteria demonstrated fluoroquinolone-sensitivity in the pre-biopsy EPS cultures. Interestingly, except for one persistent E. faecalis infection, the five cases of S. agalactiae and two cases of E. faecalis did not grow in the repeated EPS cultures after TRPB. Because fluoroquinolones can effectively treat CBP caused by these susceptible pathogens,20 the negative culture results in our post-biopsy EPS cultures may suggest that the fluoroquinolone-sensitive bacteria were eradicated with the empirical fluoroquinolone prophylaxis during TRPB.
Chronic bacterial presence can be a result of persistent infection through antibiotic resistance mechanisms.21 Except for one case of E. faecium, the antibiotic susceptibility profiles in 19 new bacterial isolates were fluoroquinolone-sensitive. Therefore, we may infer that new bacteria in post-biopsy EPS cultures are potentially new infections that had invaded from rectal mucosa through cracks, unsealed tracts in barrier layers, or uncharacterized routes after TRPB. Our hypothesis can be enforced with the clinical findings, in which increased numbers of red blood cells in the repeated EPS were observed within one-year post-TRPB. Furthermore, some patients in this study had increased WBC counts during the repeated EPS examination as well, suggesting that the complete healing process after TRPB took longer than what was initially anticipated.22
Persistently increased serum PSA levels are an important indicator for repeating prostate biopsy in men with benign prostate pathology in previous biopsies.23 In addition, serum PSA levels can be also elevated as a result of inflammatory conditions of the prostate.1724 Therefore, hypothetically, serum PSA levels in some patients with biopsy-associated CBP may influence on determining the repeated prostate biopsy. However, we could not find any differences in serum PSA levels and clinical symptoms between pre- and post-biopsy in 20 men with new bacterial infection in the prostate after TRPB (Table 2). Therefore, bacterial infection in the prostate after TRPB is not an important consideration factor for re-biopsy.
Patients with CP/CPPS report pain as the most common and serious symptom. Such symptoms can usually be evaluated with items in the pain domain of the NIH-CPSI questionnaire.25 We could not find a difference in sum of pain or discomfort domain in the NIH-CPSI questionnaire in the 20 patients during the pre- and post-biopsy period (Table 2). According to the responses to NIH-CPSI questionnaires, the sums of pain or discomfort items have remained the same in 13, decreased in 3, and increased in 4 men during follow-ups. In addition, the differences in sum of points in pain between the 2 questionnaires among 4 men that reported symptom aggravation were 1, 1, 3, and 4 points, which would be categorized as mild symptomatic changes in CP/CPPS.
Gram-negative bacteria have been well-associated with causing agents for CBP.26 In contrast, the role of gram-positive bacteria in CBP has been debated for several decades.27 Some clinicians insist that gram-positive bacteria are also pathogenic in the prostate and recommend antibiotics to resolve the symptoms.28 Furthermore, E. faecalis and S. agalactiae infected prostates reveal increased prostatic 18F-fluorodeoxyglucose (FDG) uptakes in positron emission tomography/computed tomography (PET/CT), suggesting their pathogenicity in the prostate.29 In contrast, others maintain that gram-positive bacteria are nonpathogenic because they are not the exact causes for CBP-associated symptoms.27 Our study reveals that new bacterial infections in the prostate, which were mostly caused by gram-positive bacteria, did not change the follow-up serum PSA levels, not exacerbate symptoms related to CP/CPPS, or rarely cause bacteriuria during one year after TRPB. In contrast, the finding of increased WBCs in EPS in CBP patients suggests that the infected bacteria may be responsible for newly developed prostate inflammation. Therefore, we did not prescribe antibiotics for men with new bacterial infection in the prostate after TRPB, but observed the clinical courses closely.
In conclusion, we found that the TRPB procedure is significantly associated with new bacterial infection in the biopsied prostate. However, such infections were not directly related to the pre-biopsied patients' clinical characteristics. Furthermore, post-TRPB bacterial infection in the prostate did not influence on serum PSA levels and clinical symptoms within one year after biopsy. Therefore, we do not consider post-TRPB bacterial infection in the prostate as a critical factor for deciding for re-biopsy. Furthermore, these results suggest that the localized bacteria are not likely to be persistent pathogens in rectal mucosa during TRPB, but are rather newly infected microbes that were obtained some time post-TRPB.
 XML Download
XML Download