

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Infectious diseases have historically affected the development and advancement of human societies. During the early- and mid-20th century, mortality associated with infectious diseases declined dramatically due to advances in medicine and public health; however, they remain a major public health burden worldwide. Recent data presented by the World Health Organization indicated that more than a quarter of the estimated 59 million deaths that occur globally each year are associated with infectious disease (12).
Acute respiratory illnesses are the leading cause of death from infectious diseases around the world, and occasional outbreaks of particularly virulent strains are potential public health disasters. In 2002, a few cases of a life-threatening respiratory disease caused by corona virus in China (34), ultimately resulted in a global epidemic of severe acute respiratory syndrome. Recently, a large outbreak of fatal Middle East respiratory syndrome-coronavirus (MERS-CoV) occurred following a single patient exposure in the emergency department (ED) of our institution, a tertiary-care hospital in Korea, which resulted in significant public health and economic burden (56).
EDs are one of the major gateways to hospital entry and have substantial burdens associated with infectious disease-related visits (78910). Thus, accurate categorization of patients is required, and determination of the initial isolation level is one of the most difficult issues faced by ED physicians, especially when treating patients with a suspected contagious respiratory illness (111213). After the 2015 outbreak of fatal MERS-CoV at our institution (514), a febrile respiratory infectious disease unit (FRIDU) with a negative pressure ventilation system was separately constructed outside the ED; to prevent the spread of contagious diseases within the hospital, this unit triages and determines isolation levels for all emergency patients prior to their admission to the ED or hospital. However, data on the utility of such screening units are limited.
We compared patients' initial FRIDU-determined isolation level with the level associated with their final diagnosis and assessed the limitations of the screening system. We hope this study will help efforts to integrate isolation strategies into ED contagious disease management procedures.
MATERIALS AND METHODS
Study design, subjects, and institution
We performed a retrospective cohort analysis of patients with febrile illness who were hospitalized after FRIDU screening. All patients visited the emergency center were triaged outside the ED between August 2015 and July 2016. The records of 4,128 adult patients with febrile illness who entered the FRIDU after initial triage were reviewed. Finally, the 1,562 patients who were hospitalized after FRIDU screening were included in the analysis (Figs. 1 and 2).
Fig. 1
Study patients flow through the FRIDU.
FRIDU = febrile respiratory infectious disease unit, ED = emergency department, ICU = intensive care unit, GW = general ward.

Fig. 2
FRIDU and triage. (A) The outside view of FRIDU and triage. (B) The inside view of FRIDU and triage.
FRIDU = febrile respiratory infectious disease unit, ED = emergency department, A = anteroom, T = toilet, R1–R6 = room 1–room 6, Lab1–3 = laboratory 1–3, D = doctor's examination, N = nurse's triage, R = reception.

Samsung Medical Center is a modern 1,989-bed university-affiliated tertiary hospital providing referral care in Korea and about 200 patients are seen in the ED each day. In ED for adult, there are 58 beds were spaced roughly 1.5–2.0 m apart with curtains or wall in between and ambulatory zone with 24 chairs for stable patients.
Facilities in the triage room and FRIDU outside ED
The triage room is in the front of the FRIDU, which is located outside the ED (Fig. 2A), and includes an administration area, a nurses' triage area, and a doctor's examination room (Fig. 2B). There are also 6 isolation rooms with negative pressure ventilation systems, each with a high-efficiency particulate air filter with an airtight backdraft damper (15–30 air changes per hour). An anteroom is located in front of every isolation room, and the inter-room pressure difference is −4.5 to −17 Pa. Portable radiological and ultrasound examinations, blood sample kits, polymerase chain reaction (PCR) tests for respiratory viruses, and sputum examination kits were available in every isolation and laboratory room. Oxygen supply systems (nasal prong, facial mask, etc.), devices for airway management and central vascular access, mechanical ventilation, and remote vital sign monitors were also provided.
Patient management, criteria for FRIDU screening, and determination of isolation level
All emergency center patients were triaged in the FRIDU triage room outside the ED. After that, patients who had any of the following conditions were screened for contagious diseases in the FRIDU before entering the ED or being admitted to the hospital: 1) fever ≥ 37.5°C (99.5°F) and respiratory symptoms including cough, sputum, or dyspnea (modified Medical Research Council ≥ II), 2) history of travel to high-risk countries within 2–4 weeks, regardless of fever or respiratory symptoms (e.g., Middle East for MERS-CoV or West Africa for Ebola) by the Centers for Disease Control and Prevention guidance, or 3) signs and symptoms suggesting airborne disease, such as chickenpox or tuberculosis. When a patient was determined to be clinically deteriorated at the FRIDU, the patient was moved to the resuscitation zone equipped with a portable negative pressure ventilation system or isolated in a single room with a door in the ED.
After FRIDU screening, patients were categorized according to the following three isolation levels based on the attending ED physician's diagnosis: 1) suspected of having a contagious disease requiring isolation (e.g., patients with influenza or pulmonary tuberculosis), 2) immunocompromised status requiring reverse isolation (e.g., patients with neutropenia), or 3) not requiring isolation (e.g., patients with a urinary tract infection). After the initial diagnostic work up, some patients requiring hospitalization were directly admitted from the FRIDU without entering the ED; some were hospitalized or discharged after entering the ED and receiving additional medical examinations; and some were discharged, referred elsewhere, or followed by the outpatient clinic without entering the ED or being hospitalized.
Statistical analysis
Data on categorical variables are presented as numbers and percentages, and data on continuous variables are presented as means ± standard deviations. Data on continuous variables were compared using a 2-sample t-test and the data were normally distributed. Data on categorical variables were compared by χ2 or Fisher's exact test. The consistency of the isolation levels assigned based on the FRIDU screening and that associated with the final diagnosis was assessed using a correlation coefficient (kappa). Univariate and multivariate analyses with logistic regression were performed to evaluate factors associated with being diagnosed with a contagious disease by the FRIDU screening. Statistical analyses were performed using PASW software (ver. 22.0; SPSS Inc., Chicago, IL, USA), and a 2-sided P value < 0.05 was considered statistically significant.
Ethics statement
The Institutional Review Board of the Samsung Medical Center approved this study and permitted the review and publication of patient records (IRB registration number 2016-08-166). The requirement for informed consent by individual patients was waived due to the retrospective design of the study.
RESULTS
Study patients
In total, 59,546 patients visited the emergency center during the one year and were triaged in the FRIDU outside the ED. After initial triage, 4,128 adult patients with febrile illness were screened at FRIDU and 1,422 patients were discharged, referred elsewhere, or followed by the outpatient clinic without entering the ED. Four hundred three patients were directly hospitalized without entering the ED and 114 patients were admitted to the resuscitation zone due to clinical instability during FRIDU screening; of these, 29 patients were later discharged or referred elsewhere. Of the 2,189 patients who entered the ED after FRIDU screening, 1,115 were discharged, referred elsewhere, or followed by the outpatient clinic without hospitalization based on the ED physician's decision. Finally, the 1,562 patients with febrile illness who were hospitalized after FRIDU screening were included in the analysis (Fig. 1).
Clinical characteristics of study patients
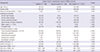
In total, 1,562 patients with febrile illness who were hospitalized after FRIDU screening were included in the analysis. Characteristics of study patients are shown in Table 1. Based on FRIDU screening, 198 patients (13%) were isolated (isolation), 194 patients (12%) were reverse isolated (reverse isolation), and 1,170 patients (75%) did not require isolation (non-isolation). More than 40% of isolation patients were relatively elderly (≥ 65 years), and they were more likely to have chronic heart disease (16%) (P = 0.001) or chronic pulmonary disease (24%) (P < 0.001) compared with the other two groups. The amount of time spent in the FRIDU was longest for the isolation group. Among reverse isolation patients, 73% had active hemato-oncologic malignancy (P < 0.001), 87% had fever (P < 0.001), and 32% had relatively severe diseases as indicated by the Emergency Severity Index score or Korean Triage and Acuity Scale (modified version of the Canadian Triage and Acuity Scale) ≤ 2 (P = 0.002) (Supplementary Table 1). Each of these indicators was the highest in the reverse isolation group.
Table 1
Characteristics of patients hospitalized with acute febrile illness via ED after FRIDU screening
Isolation level by final diagnosis
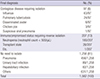
The appropriate isolation levels for the final diagnoses confirmed during hospitalization are shown in Table 2. Of 1,562 patients, 97 (6%) were confirmed to have a contagious disease requiring isolation, such as influenza (n = 63), pulmonary tuberculosis (n = 24), disseminated zoster (n = 6), chicken pox (n = 3), or suspicious viral pneumonia (n = 1). An additional 207 patients (13%) with immunocompromised status required reverse isolation, mainly due to neutropenia (n = 180) or transplant status (n = 26). The remaining 1,258 patients (81%) did not require isolation. Among these, pneumonia (n = 456) was the most common diagnosis, followed by urinary tract infection (n = 89), and hepatobiliary infection (n = 82).
Table 2
Isolation levels according to final diagnosis confirmed during hospitalization of study patients
Consistency of isolation levels based on FRIDU screening and final diagnosis
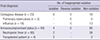
We compared the isolation levels based on the initial FRIDU screening with that associated with the final diagnosis to evaluate their consistency, as shown in Table 3. The isolation level was consistent for 1,309 (83%) patients; of these, 74 required isolation, 143 required reverse isolation, and 1,092 did not require isolation. The correlation coefficient for isolation consistency was 0.565 (P < 0.001).
Table 3
Consistency of isolation levels based on FRIDU screening and final diagnosis

The remaining 253 patients were inconsistently isolated. Of these, 166 did not ultimately require isolation but were initially isolated (n = 120) or reverse isolated (n = 46). Of the other 87 patients, 23 had contagious diseases but were inappropriately reverse isolated (n = 5) or not isolated (n = 18), and 64 patients had immunocompromised status but were inappropriately isolated (n = 4) or not isolated (n = 60) (Table 4).
Table 4
Patients who were confirmed to have contagious disease requiring isolation or immunocompromised status but, who were applied inappropriate isolation level after hospitalization
We additionally categorized study patients into 2 groups (isolation vs. reverse isolation and non-isolation), the sensitivity and negative predictive value (NPV) of FRIDU screening for diagnosing contagious disease requiring isolation are 76% (confidence interval [CI], 67%–84%) and 98% (CI, 97%–99%), respectively.
Risk factors for predicting contagiousness at FRIDU screening
We additionally used univariate and multivariate analyses with a logistic regression model to determine the factors related to being diagnosed with a contagious disease at the initial FRIDU screening (Supplementary Table 2). The variables used were old age (≥ 65 years), gender (male), chronic kidney disease, transplant history, fever (≥ 37.5°C), and leukocytosis (>10,000/μL). Transplant history (odds ratio [OR], 2.294; P = 0.003), fever (OR, 0.616; P = 0.030), and leukocytosis (OR, 0.315; P = 0.005) were significantly associated with an initial diagnosis of a contagious disease.
Deterioration during FRIDU screening
Of 4,128 patients who were screened in the FRIDU, 114 patients were admitted to the resuscitation area due to clinical instability during FRIDU screening; three of these patients died in the ED. One of the 3 underwent cardiac arrest in the FRIDU and was moved to the resuscitation zone in the ED while cardiopulmonary resuscitation was performed. Twenty-nine of the 114 patients were discharged or referred elsewhere in the resuscitation area (Fig. 1) and were excluded from the analysis due to limited clinical and laboratory data. The 85 hospitalized patients who deteriorated during FRIDU screening are described in Table 5.
Table 5
Characteristics of patients who deteriorated during FRIDU screening

Of the 85 patients, 17 (20%) had contagious diseases and 37 (44%) were male. Most patients had fever (n = 64, 75%) and/or dyspnea (n = 66, 78%). Twenty-seven patients (32%) had septic shock, 33 (38%) had respiratory failure, 10 (12%) had heart failure, and 15 (18%) had an illness with an unknown cause.
DISCUSSION
The most important findings of our study were that the isolation levels determined based on initial FRIDU screening were moderately well correlated with the isolation levels required by the final diagnoses. And FRIDU screening had high NPV for diagnosing contagious disease requiring isolation, demonstrating the utility of pre-hospitalization screening units. Of 97 patients diagnosed with contagious diseases requiring isolation, 74 patients were isolated and 5 patients were reverse isolated, and all of the 5 patients had had both neutropenia and influenza. Of 18 patents who were non-isolated, 16 had a negative result of influenza antigen test at initial FRIDU but they subsequently were confirmed to have respiratory virus infection during hospitalization by PCR test. Additionally, 143 of 207 immunocompromised patients were reverse isolated based on FRIDU screening. Actually, more than two-thirds of the 60 immunocompromised patients, who were categorized into non-isolation based on FRIDU screening, were observed in their own bed with curtain and reverse isolation notice, due to the lack of revere isolation room. Of them, patients who had respiratory symptoms such as cough, sputum mandatorily had to wear a surgical mask and were thoroughly trained for respiratory etiquette in our hospital. Moreover, given that no serious nosocomial outbreaks occurred during the study period, pre-hospitalization screening systems for contagious diseases could be a viable strategy for preventing nosocomial infections (1516).
We additionally evaluated risk factors for predicting contagious diseases at the screening level. Patients who were diagnosed with contagious diseases were more likely to have a transplant history, but, oddly, they were less likely to have fever or leukocytosis. These results imply that commonly used clinical parameters, such as fever or leukocytosis, may not be enough to accurately discriminate between contagious and non-infectious diseases. In our study, only 62 of 97 (64%) patients with a contagious disease had a fever and 89 (92%) had leukocytosis. Both of these proportions were significantly lower than those for the remaining patients with non-contagious diseases (P = 0.031 for fever, P = 0.008 for leukocytosis). However, a more general interpretation of these findings is limited in that our institution is one of the largest tertiary-referral centers in Korea, and our patients generally have relatively severe or complicated conditions.
There have been very few studies conducted on pre-hospital triage. During the 2009 influenza pandemic, an influenza-like illness scoring system was used to triage 1,840 ED patients with acute respiratory illness treated at a Mexican hospital (17). In a study conducted in Qatar, a surveillance system protocol reduced the number of patients who needed to be tested for MERS-CoV at an ED (18). However, to date, no data on the utility of screening systems outside the ED of tertiary medical centers have been collected at the pre-hospitalization stage, especially for all emergency center patients; thus, our study is unique and significant.
During the study period, we found several problems regarding the maintenance of our screening system, and these could be critical if inappropriately managed. The greatest concern was that some patients deteriorated during FRIDU screening, and 3 of the 114 patients who were moved to the resuscitation zone during our study period died in the ED. Although the medical facilities in the FRIDU are well established, special medical resources, such as computed tomography, were not available or applied late, and the screening process is focused on contagious diseases; hence, critically ill patients are at risk of clinical deterioration during the screening process.
The other major problem is that maintaining a separate screening system outside the ED requires considerable personnel and financial resources. During the study period, an average of 12 patients were screened daily in the FRIDU, which means that the screening process was activated every 2 hours, and the FRIDU required staffing 24 hours a day. For these reasons, the ideal tertiary hospital ED isolation system still may not be enough—although most hospitals are still far from the ideal. A study conducted in the United Kingdom in 2007 found that only 24% of 203 hospitals reviewed had isolation facilities available in the ED (19). A recent evaluation of 48 infectious disease isolation facilities in 16 European countries found that only 18 facilities fulfilled the definition of a high-level isolation unit, and only 34 had all essential equipment for negative pressure (20). Given that disasters such as the recent outbreak in Korea (5) can affect not only public health but the economy (6), we believe that a more efficient screening process is needed.
The present study had several limitations. First, the screening criteria for contagious diseases were not validated, especially regarding the definition of fever, which was very low (≥ 37.5°C). Second, mainly due to the retrospective design, we could not evaluate the degree to which the screening system was more effective than the previous system at preventing nosocomial outbreaks. Third, we analyzed just patients who were hospitalized after screening, so we could not know final diagnosis of the patients such as discharged, referred or followed by the outpatient clinic. Forth, our study population was not representative in terms of baseline clinical characteristics, such as comorbidity, because our study was conducted at a large tertiary-referral center.
To the best of our knowledge, this is the first study to demonstrate the utility of a contagious diseases screening unit outside an ED and hospital. We showed that the isolation level determined based on the FRIDU screening system was moderately well correlated with the isolation levels required by the final diagnosis, and no serious nosocomial outbreaks of contagious diseases occurred during the study period. However, the problems of clinical deterioration during screening and the financial and personnel costs remain. Therefore, further system-level studies on triage strategy are needed.
 XML Download
XML Download