

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recently advanced neonatal intensive care markedly improved the survival rates of very low birth weight infants (VLBWIs) weighing less than 1,500 g at birth (1). Home oxygen use can facilitate early discharge of survived VLBWIs who experience frequent hypoxic events due to various morbidities, such as bronchopulmonary dysplasia (BPD), apnea-bradycardia of prematurity, and feeding related desaturation (2345). Home oxygen use in infants also enables bonding with parents in the home environment in addition to promotion of improved growth and development and reduces healthcare costs (6). Home oxygen is usually recommended in infants with oxygen saturations below 92% to 95% in room air (7). However, there is a lack of general consensus regarding home oxygen use in VLBWIs among neonatal intensive care units (NICUs). Moreover, because infants receiving home oxygen are usually expected to have frequent healthcare utilization related to their original morbidities, appropriate follow-up plans after NICU discharge must be established, with basic knowledge regarding their follow-up courses (89). However, to date, there are no actual data regarding home oxygen use in VLBWIs discharged from the NICU in Korea. Therefore, the prevalence as well as the real effect of home oxygen use in VLBWIs on health care utilization during follow-up periods after NICU discharge needs to be investigated urgently for the proper provision of their national health care monitoring.
A large national retrospective survey for health care utilization after NICU discharge in preterm infants below 33 weeks of gestation “Retrospective Study to Evaluate Rehospitalization & Health Care Utilization after NICU Discharge in Preterm Infant of < 33 weeks' gestation (RHANPI) study” in Korea has been previously conducted and confirmed that preterm infants were more prone to readmission following NICU discharge in Korea (10). Using the part of these data, we aimed to evaluate the prevalence of home oxygen use and to analyze the clinical impact of home oxygen use in VLBWIs on their healthcare utilization, readmission, and death following NICU discharge by comparison between those of VLBWI with and without home oxygen at NICU discharge.
MATERIALS AND METHODS
The study population consisted of VLBWIs who were born < 1,500 g and 22 to 32 weeks' gestation at birth and survived to NICU discharge between April 2009 and March 2010, and were followed up until April 2011. Data used in this study were collected between August and December 2011 through the national survey of the RHANPI study conducted by the Committee on Data Collection and Statistical Analysis of the Korean Society of Neonatology. The RHANPI dataset originally included 2,351 preterm infants who were born at 22 to 32 weeks' gestation and survived to discharge from April 2009 to March 2010 from 44 participating institutions in Korea (10).
Among 2,351 preterm infants 1,356 VLBWIs from 43 hospitals (1 hospital with no VLBWI was excluded), who weighed < 1,500 g at birth, were identified for this study, and 124 cases that had missing data on home oxygen use were excluded. Finally, 1,232 VLBWIs were identified and divided into groups of infants prescribed with (HO, n = 167) and without (CON, n = 1,059) home oxygen at discharge. Perinatal and neonatal outcomes were compared between the 2 groups. Clinical effects of home oxygen use in VLBWIs were analyzed by comparison of the rate and frequency of outpatient department (OPD) and emergency room (ER) visits and readmission and death rate following NICU discharge between the 2 groups. These comparisons were conducted in total and stratified gestational age (GA)-subgroups of 25 weeks' gestation or less (≤ 25w GA), of 26–28 weeks' gestation (26–28w GA), and of 29 weeks' gestation or more (≥ 29w GA).
Based on standard study formats and manual definition of the RHANPI study variables, the neonatologists at each center retrospectively collected data by reviewing charts and registered all information in a central database between August and December 2011. To improve data quality, collected data were reviewed repeatedly, and all data that had suspected errors or missing information were referred to the corresponding neonatologist for correction. A central database of the electronic case reporting system of Oracle Korea (Oracle Corporation, Seoul, Korea) was created in collaboration with the Clinical Research Center of Samsung Medical Center.
GA at birth was determined by the best obstetric estimate, using the last menstrual period or early ultrasonographic examination (11). Small for GA was defined as birth weight less than the 10th percentile for GA compared with the intrauterine preterm growth chart (12). Grade III or IV intraventricular hemorrhage (IVH) was diagnosed using cranial ultrasonography and classified in accordance with the grading system of Papile et al. (13). Necrotizing enterocolitis (NEC) was defined as Bell's stage II or greater (14). BPD was defined as the need for supplemental oxygen at 36 postmenstrual weeks or discharge, whichever came first (15).
Home oxygen was recorded when the infants were discharged home with oxygen use of any type of support. At discharge, whether the infants required a home pulse oximetry (monitor) or G-tube or gastrostomy tube feeding were also recorded. Duration of home oxygen use was recorded.
OPD visits were defined as pediatric outpatient clinic visits and comprised regular and irregular visits. Regular visits were prearranged visits to monitor growth and development or for vaccination, and irregular visits were unscheduled visits for a check-up for various health issues including respiratory problems. Readmission after NICU discharge was defined as readmission to any hospital as stated in the patient's medical records. Visits to emergency centers and outpatient clinics were confined to events at the participating hospitals.
Statistical analysis
Continuous data were presented as means and standard deviations and categorical data as actual numbers and percentages. For between-group comparisons, the Student's t-test was used for continuous variables and the χ2 test for categorical variables. The Pearson correlation was analyzed between the proportion of home oxygen use and number of VLBWIs discharged alive in each hospital. The Kaplan-Meier estimation was used to estimate the cumulative readmission rate after NICU discharge, and the log-rank test was used to compare the readmission rate following NICU discharge between the 2 groups or among GA sub-groups. To analyze the risks for readmission or death rate, we used the time-dependent Cox proportional hazard model with the following covariates: home oxygen use, GA and follow-up duration. The hazard ratios (HRs), 95% confidence intervals (CIs), and P values were reported. All P values < 0.05 were considered statistically significant. All analyses were performed using the SAS (version 9.4, SAS Institute Inc., Cary, NC, USA).
RESULTS
Home oxygen use and institutional variation
The proportion of HO in the VLBWIs clearly showed significant institutional variation (Fig. 1). Of 43 hospitals enrolled, the proportion of HO in VLBWIs was 0% in 14 hospitals and ranged from 2.9% to 36.4% in 29 hospitals. The mean number of VLBWIs discharged alive from the enrolled 43 hospitals was 28.7 ± 22.0 (range, 7–121), and the mean proportion of home oxygen use in each hospital was 10.6% ± 11.2%. There was no significant correlation between the proportion of home oxygen use and the total number of VLBWIs discharged alive in each hospital (R2 = 0.1412; P > 0.050) (Fig. 1).
Fig. 1
Correlation of number of VLBWIs discharged alive with the proportion of home oxygen use. Correlation of number of VLBWIs discharged alive with the proportion of home oxygen use in each hospital, which showed no significant correlation (R2 = 0.1412; P > 0.050). Fourteen hospitals showed 0% home oxygen use in VLBWIs discharged alive and 29 hospitals showed the proportion of home oxygen use ranged from 2.9% to 36.0%.
VLBWIs = very low birth weight infants.

Clinical characteristics and follow-up duration
Comparisons of the clinical characteristics and follow-up duration after NICU discharge between the HO and CON in total and in each GA subgroup were described in Table 1. The proportion of the HO infants was 13.7% in total, 37.1% in the ≤ 25w GA (49/132), 17.5% in the 26–28w GA (87/497), and 5.5% in the ≥29w GA subgroup (44/431).
Table 1
Clinical characteristics, outcome, and follow-up duration of VLBWIs with and without home oxygen use
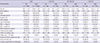
Data shown are number (%) not otherwise specified.
VLBWIs = very low birth weight infants, ≤ 25w GA = gestational age-subgroup of 25 weeks' gestation or less, 26–28w GA = gestational age-subgroup of 26–28 weeks' gestation, ≥ 29w GA = gestational age-subgroup of 29 weeks' gestation or more, HO = home oxygen use at discharg, CON = no home oxygen use at discharge, GA = gestational age, NEC = necrotizing enterocolitis, IVH = intraventricular hemorrhage, BPD = bronchopulmonary dysplasia.
*P < 0.050 vs. HO.
The mean GA and birth weight were significantly lower in the HO infants than in the CON infants in total and in all GA subgroups, respectively. The proportion of male infants among the enrolled infants was higher in the HO infants than in the CON infants in total and in ≥ the 29w GA subgroup. Antenatal steroid use was higher in the HO infants than in the CON infants in total, but not in all GA subgroups. There were no differences between the 2 groups in the proportion of SGA and of having elder siblings. More use of surfactants and higher rates of high grade IVH and blood culture-proven sepsis were observed in the HO infants than in the CON infants, in total. The HO infants comprised more infants diagnosed with BPD than the CON infants in total and in all of GA subgroups.
The follow-up duration was not equal between the 2 groups. The mean follow-up duration of infants after NICU discharge was slightly longer in the HO infants than in the CON infants. However, follow-up loss during the relatively early period (less than 12 months after discharge) was frequent in the HO infants, especially in subgroups of 26–28w GA and > 29w GA.
The mean duration of home oxygen use in the ≤ 25w GA subgroup was longer than that in the 26–28w GA subgroup, which was longer than that of in the ≥ 29w GA subgroup. The proportion of home pulse oximetry use and G-tube/gastrostomy feeding at discharge was higher in the HO infants than in the CON infants in total and in all of the GA subgroups.
Medical service uses and death during follow-up after NICU discharge
We compared the follow-up courses by focusing on use of medical services, such as pediatric OPD visits, ER visits, and readmission, and on death following discharge between the 2 groups (Table 2).
Table 2
Medical resources used and death between VLBWIs with and without home oxygen use
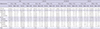
VLBWIs = very low birth weight infants, ≤ 25w GA = gestational age-subgroup of 25 weeks' gestation or less, 26–28w GA = gestational age-subgroup of 26–28 weeks' gestation, ≥ 29w GA = gestational age-subgroup of 29 weeks' gestation or more, HO = home oxygen use at discharge, CON = no home oxygen use at discharge, SD = standard deviation, OPD = outpatient department, ER = emergency room.
*P < 0.050 vs. HO.
Because the total mean follow-up duration after discharge was longer (743 ± 179 vs. 715 ± 120 days; P < 0.050) and the GA was lower in the HO infants than in the CON infants, adjusted odds ratios (ORs) or HRs for medical service use or death of the HO infants compared to the CON infants were calculated by correction of the follow-up duration and GA of the infants (Table 3).
Table 3
Risks of medical resources used and death between VLBWIs with and without home oxygen use
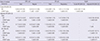
VLBWIs = very low birth weight infants, OPD = outpatient department, ER = emergency room, HR = hazard ratio, OR = odds ratio, HO = home oxygen use at discharge, CON = no home oxygen use at discharge, CI = confidence interval, ≤ 25w GA = gestational age-subgroup of 25 weeks' gestation or less, 26–28w GA = gestational age-subgroup of 26–28 weeks' gestation, ≥ 29w GA = gestational age-subgroup of 29 weeks' gestation or more.
*Unavailable due to 0 events in CON.
Most of the VLBWIs visited a pediatric OPD after NICU discharge. The proportion of the infants who visited pediatric OPD regularly more than once was significantly lower in the HO infants than in the CON infants in total (85.2% vs. 95.7%; P < 0.001; adjusted OR, 0.26; 95% CI, 0.44–0.60) and in all GA subgroups. However, the HO infants more frequently went to regular OPDs for check-ups on growth and development and for vaccinations compared to the CON infants (12.7 ± 7.5 vs. 9.5 ± 6.6 times; P < 0.010). The total percentage of infants who visited an ER for any reason after NICU discharge was not significantly different between the HO and CON infants (37.3% vs. 31.9%; P > 0.05; adjusted OR, 1.25; 95% CI, 0.89–1.75); the proportion of infants with ER visits owing to respiratory problems was higher in total (22.8% vs. 19.1%; P < 0.050; adjusted OR, 1.47; 95% CI, 0.99–2.16), with modest significance, and with a significance in the 26–28w GA subgroup. Furthermore, ER visits owing to respiratory problems were more frequent in the HO infants than in the CON infants in total (2.5 ± 2.2 vs. 1.8 ± 1.4 times; P < 0.050).
The overall rate of readmission for any reason in the HO infants was significantly higher than that in the CON infants in total (53.3% vs. 35.7%; P < 0.010) and in ≥ 29w GA subgroup. The overall death rate was also significantly higher in the HO infants than in the CON infants in total (3.0% vs. 0.6%; P < 0.050) and in the ≥ 29w GA subgroup (6.1% vs. 0.7%; P < 0.05). The adjusted HR for death in the HO infants was 7.40 (95% CI, 2.06–26.50) in total, 4.75 (95% CI, 0.67–33.71) in the 26–28w GA subgroup, and 8.94 (95% CI, 1.64–48.79) in the ≥ 29w GA subgroup respectively.
Cumulative readmission rate
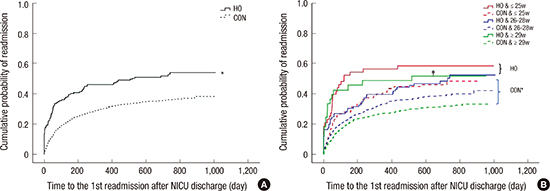
The cumulative readmission rates at the time-point after discharge from the NICU are shown in Table 4. In the first 360 days after discharge from the NICU, 46.1% of the HO infants readmitted cumulatively in total, 56.3% in the ≤ 25w GA subgroup, 39.5% in the 26–28w GA, and 48.5% in the ≥ 29w GA subgroup; 30.6% of the CON infants readmitted in total, 41.0%, 33.4%, and 27.1% in each GA subgroup, respectively. Consequently, the HO infants showed a significantly higher probability of total readmissions compared to the CON infants in total (Fig. 2A) (log-rank test for trend < 0.05) and in any GA subgroups, except for the ≤ 25w GA subgroup (Table 4). In addition, the HO infants did not show significant differences in the cumulative readmission rate calculated by log-rank among the GA subgroups, whereas the CON infants showed significant differences (Fig. 2B). Consequently, the degree of prematurity proportionally increase the risk for readmission in the CON infants; this trend was not observed in the HO infants.
Table 4
Cumulative readmission rate after discharge from NICU between VLBWIs with and without home oxygen use
NICU = neonatal intensive care unit, VLBWIs = very low birth weight infants, CI = confidence interval, HR = hazard ratio, HO = home oxygen use at discharge, CON = no home oxygen use at discharge, ≤ 25w GA = gestational age-subgroup of 25 weeks' gestation or less, 26–28w GA = gestational age-subgroup of 26–28 weeks' gestation, ≥ 29w GA = gestational age-subgroup of 29 weeks' gestation or more, GA = gestational age.
*P value was adjusted for the GA and the duration of follow-up.
Fig. 2
Cumulative probability of readmission of enrolled infants after NICU discharge. Cumulative probability of readmission of enrolled infants depicted by time to the first readmission after NICU discharge in total (A) and according to GA subgroups (B). In total (A), the HO subgroup significantly higher probability of readmission than that of the CON subgroup in VLBWIs discharged alive from NICU. In subgroup analysis (B), whereas there were significant differences in cumulative probability or readmission among CON subgroups, no differences were found among HO subgroups.
NICU = neonatal intensive care unit, GA = gestational age, HO = home oxygen use at discharge, CON = no home oxygen use at discharge, VLBWIs = very low birth weight infants, ≤ 25w GA = gestational age-subgroup of 25 weeks' gestation or less, 26–28w GA = gestational age-subgroup of 26–28 weeks' gestation, ≥ 29w GA = gestational age-subgroup of 29 weeks' gestation or more.
*P < 0.050 by log-rank test; †P < 0.050 by log-rank test between the HO and the CON in ≥ 29w GA subgroup.

DISCUSSION
The present study has demonstrated that 13.7% of total VLBWIs identified nationally have been discharged from the NICU, with home oxygen showing significant institutional variations in Korea. These infants were more likely to be born at a younger GA and to need more a G-tube or gastrostomy at discharge. The VLBWIs with home oxygen visited regular pediatric OPD and ER owing to respiratory problems more frequently and had the increased the risk of 1.6 times for re-admission and 7.4 times for death compared to VLBWIs without home oxygen. However, these increased risks in the VLBWIs with home oxygen were not significantly related to their degree of prematurity. Consequently, home oxygen use in the VLBWIs increased the risks for their readmission and the use of medical services as well as for death following discharge from the NICU, which necessitate the proper provision of a more carefully planned health care monitoring.
Recently, the prevalence of home oxygen use by preterm infants at NICU discharge is increasing, as evident in the study from Australia showing that the percentage of home oxygen use in preterm infants increased from 2.3% in the 1980s to 10% in the early 2000s (16). In a study from the United States, 16.6% of preterm infants with 23–31 weeks of GA used home oxygen after discharge, which is consistent with our results. In that study, the rate ranged from 59.2% of those with GA < 25 weeks to 7.3% of those with ≥ 29 weeks (17). The EPICure study showed that of the 283 survivors born at ≤ 25 weeks' gestation, 36% were discharged home on oxygen (18), which is also consistent with the rate of 37.1% of the infants born at ≤ 25 weeks' gestation in the present study. The rate of home oxygen use in the VLBWIs was inversely proportional to GA, which ranged from 37.1% in the infants born at ≤ 25 weeks' gestation to 5.5% in the infants born at ≥ 29 weeks in the present study. In summary, these findings suggest that a certain proportion of immature preterm infants necessitate HO as these infants tend to survive more.
Institutional variation might be the most important factor for the determination of home oxygen use in preterm infants (17). In the present study, the rate of home oxygen use ranged from 2.9% to 36.4% in 29 NICUs as well as even 0% in 14 NICUs. A German study reported that NICUs admitting > 50 VLBWIs annually significantly and more frequently prescribed home oxygen and aimed for SpO2 levels closer to the physiological range than those admitting fewer VLBWIs (19). However, in the present study, we could not find any correlation for NICU size and prescription rate of home oxygen at discharge in the VLBWIs. Further studies are needed to elucidate the exact effect of institutional variation on the rate of home oxygen use in preterm infants in Korea.
Home oxygen use enables early discharge from the NICU and reduces the risk of exposure to an adverse environment resulting from a prolonged hospital stay; this also reduces medical expenses, allows efficient use of medical resources, and is beneficial for a closer parent-infant relationship (162021). In contrast, home oxygen therapy increases parental stress from the use of medical equipment at home, and home care of the infant may increase the risks of various aspects such as vulnerable lung function (222324), which necessitate careful monitoring and follow-up plan.
Therefore, the present study has attempted to examine how the follow-up courses after NICU discharge were affected by home oxygen use among the VLBWIs by comparison with the VLBWIs without home oxygen use. Unexpectedly, even after adjustments of the different follow-up durations and GA of the 2 groups, the percentage of infants who visited regular outpatient clinics in the HO infants was significantly lower than that in the CON infants. This might be resulted from more early follow-up loss in HO group than in CON group, which was demonstrated that the proportion of the infants with follow-up loss within 12 months for discharge was significantly higher in HO group than in CON group. Our study retrospectively surveyed NICU of various sizes. Therefore, at smaller NICU, some infants with more complicated courses such as development of severe retinopathy of prematurity (ROP), complicated surgical, or respiratory problems, who probably comprised a higher proportion of the infants in the HO group than in the CON group, might have been transferred to larger hospitals during follow-up after NICU discharge. Furthermore, since visits to OPD were confined to events at the participating hospitals in the present study, inconvenience for moving due to oxygen supply in HO group might have been a factor for impeding regular visits to participating hospital and thus for favoring visits to their vicinity hospital. This lower rate of regular pediatric OPD visits in the home oxygen group needs to be re-examined via prospectively designed studies in the future.
On the other hand, in the present study, the frequency of regular outpatient visits was greater in the HO group, whereas the frequency of irregular visits, including those for respiratory problems, was not different between the groups. This is probably because the proportion of the patients with BPD was significantly higher in the HO group than the CON group, and they were main candidates for respiratory syncytial virus (RSV) prophylaxis, which needed regular follow-up at least once a month during RSV seasons (232526). In contrast, Spiegler et al. (27) reported that in a follow-up of VLBWIs for a year after discharge, the difference in the number of outpatient visits was smaller than expected because the schedule of vaccinations and regular check-ups during the first year was tight for all VLBWIs.
Our study demonstrated 1.6 times higher risks for readmission in the HO group compared to that in the CON group without significant correlation between the readmission risks and degree of prematurity in the home oxygen group. This result was consistent with that of a prospective study on respiratory outcomes following extreme preterm birth in England, which demonstrated that children discharged with home oxygen were at an increased risk for readmission in the first 30 months (18).
Furthermore, in the present study, 3.0% of the HO group (5/169) died after discharge during the follow-up period; this group also had a higher risk of death by 7.4 times following NICU discharge than the CON group. Although we were unable to collect data on the causes of death, the main causes of death for these high-risk newborn infants might include respiratory infection, respiratory failure, and cor pulmonale during home care (28), which can be confirmed in further prospective studies in the future.
Notably, in the present study, the degree of prematurity did not correlated with increased risks of readmission or death in the VLBWIs with home oxygen. Therefore, we must carefully consider the decision for discharge with home oxygen in these high-risk infants and require meticulous education of parents regarding home cardiopulmonary monitoring as well as planned and careful health care follow-up.
There are several limitations in our study. A retrospective nature has major drawbacks. With data collected for the cases prior to the design of this study, detailed information regarding home oxygen use and weaning during follow-up up as well as heterogeneous underlying diseases, was unavailable. The number of visits and duration of follow-up after discharge were different among the infants. The effects of institutional variation, such as prescription guidelines for home oxygen use and follow-up schedules in preterm infants, could not be analyzed because of the lack of information. Despite these several limitations, the strength of our report would be that it is the first large-scale, nationwide report on VLBWIs with home oxygen and their follow-up courses in Korea.
In conclusion, approximately 13% of all survived VLBWIs require home oxygen at discharge from NICUs in Korea. Less mature infants are more prone to be prescribed with home oxygen at discharge. Home oxygen use in VLBWIs increased the risks for more use of healthcare facilities following NICU discharge, such as regular OPD or ER visits owing to respiratory problems, as well as for readmission and death during follow-up, regardless of the GA. Therefore, meticulous healthcare monitoring of VLBWIs who require home oxygen after discharge from the NICU is needed, and if possible, development of a special national healthcare program for these patients is required.
 XML Download
XML Download