

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Increased serum uric acid level is proposed to be associated with adverse cardiovascular (CV) events in patients with risk factors such as hypertension, diabetes, heart failure, or metabolic syndrome (1234). However, the causal relationship remains controversial because hyperuricemia can also be caused by conditions like renal dysfunction, gout, alcohol consumption, or diuretic therapy, confounding the association between hyperuricemia and CV events. Uric acid was reported to have a role as an endogenous antioxidant in previous studies (56) and recent studies shows that low uric acid level is associated with endothelial dysfunction (457). These reports have raised questions about the impact of hypouricemia on CV events. However, no data are available on the association of serum uric acid level and VSA which has endothelial dysfunction as a possible pathophysiologic mechanism (8910).
Our hypothesis is that low uric acid level might cause adverse clinical outcomes in vasospastic angina (VSA) in connection with endothelial cell dysfunction. Therefore, we investigated the impact of serum uric acid level on clinical outcomes in VSA patients with or without significant coronary artery stenosis confirmed by spasm-provocation test.
materials and Methods
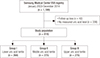
The study population was selected from the Samsung Medical Center VSA registry. Between January 2003 and December 2014, 1,199 consecutive patients with VSA were enrolled in a single center registry. VSA was defined by the Guidelines for Diagnosis and Treatment of Patients with Vasospastic Angina of the Japanese Circulation Society (11). Inclusion criteria were: 1) coronary spasm proven by coronary angiography (CAG) and spasm-provocation test, and 2) serum uric acid level measured at admission. Enrolled patients were categorized according to the admission uric acid level into group I (≤ 4.8 mg/dL, n = 268), II (4.9–5.9 mg/dL, n = 275), or III (≥ 6.0 mg/dL, n = 275) (Fig. 1). In addition, we divided patients into pure VSA or mixed angina groups using previous history or the presence of significant fixed stenosis on CAG after intracoronary nitroglycerin injection. Mixed angina was defined as: 1) fixed coronary artery stenosis > 50% in spasm-positive arteries, or 2) previous history of myocardial infarction (MI) or coronary artery revascularization. Patients who did not meet these criteria were assigned to a pure-VSA group (12).
After diagnostic CAG, intracoronary ergonovine was administered for spasm-provocation tests with starting dose of 10 µg for the right coronary artery (RCA) and 20 µg for the left coronary artery (LCA). The dose was doubled in a step-wise manner to a maximum dose of 20 µg for RCA and 80 µg for LCA. When spasm was provoked, intracoronary nitroglycerine was administered and spasm resolution was confirmed by repeated CAG. The definition of a positive result was: 1) transient, total, or subtotal occlusion of the coronary arteries, and 2) ischemic symptoms and/or electrocardiographic (ECG) changes. ECG change was defined as ST-segment elevation, depression (≥ 1 mm), or T-wave inversion in at least 2 consecutive leads (11).
Clinical, laboratory, and outcome data were collected by a trained study coordinator using a standardized case report form and protocol. If necessary, additional information was documented by contacting the principal investigators and/or by review of hospital records. The primary outcome was major adverse cardiac events (MACEs), which were defined as a composite of cardiac death, acute MI, ischemic stroke, coronary revascularization, and rehospitalization for angina. Secondary outcomes were each component of MACE and all-cause death. All deaths were considered to have a cardiac cause unless a definite non-cardiac cause could be established.
All values are presented as mean ± standard deviation or median with interquartile range. Comparisons between continuous variables were made using a t-test or Wilcoxon rank-sum test when applicable. Categorical data were tested using Fisher's exact test, χ2 test, or Kruskal-Wallis test as appropriate. For outcome analysis, event-free survival was estimated by the Kaplan-Meier method and compared with the log-rank test. Cox proportional hazard model was used to compare relative risk among uric acid groups and to determine prognostic factors for clinical outcomes. Variables that showed significant differences in baseline characteristics were included for deriving adjusted hazard ratios (HRs) for each clinical outcome. Variables of which the P value was < 0.200 in univariate analysis were included in multivariate analysis for prognostic factors. A P value < 0.050 was considered statistically significant. SPSS version 23 program (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
Results
Of the 1,199 patients in our VSA registry, 818 were included in final analysis (Fig. 1). Baseline clinical characteristics are in Table 1. Median age of the patients was 57 (50–63) years and 693 (84.7%) were men. Most patients (94.3%) were treated with a calcium channel blocker (CCB) and more than half were prescribed aspirin or a statin as discharge medication. Three hundred ten patients (37.9%) of total population received both CCB and nitrate, while 479 patients received monotherapy (CCB, n = 462; nitrate, n = 17). Median uric acid values were 4.1 mg/dL for group I, 5.4 mg/dL for group II, and 6.7 mg/dL for group III. Patients were followed for a median 49.2 months (22.7–83.9 months) and no significant difference was observed in the median follow-up duration among the 3 groups (50.1 for group I vs. 49.3 for group II vs. 48.7 months for group III, P = 0.312). Group I had significantly more women and higher high-density lipoprotein (HDL) cholesterol levels than the other 2 groups. The prevalence of smoking, body mass index (BMI), and serum creatinine levels were significantly lower in Group I patients than the others (Table 1). No other characteristics showed significant differences among the groups. In the overall population, group II had a significantly lower incidence of MACE compared to group I and a tendency of lower incidence of MACEs compared to Group III (Table 2). Survival curves were generated for VSA patients with or without significant fixed lesions and according to uric acid level. For pure VSA, group II patients showed significantly higher MACE-free survival compared to patients in the other groups (group I, 80.7%, P = 0.037; group II, 91.7%, reference; group III, 80.1%, P = 0.023). In contrast, no significant differences in MACE-free survival were seen according to uric acid level in patients with mixed angina (P = 0.314) (Fig. 2A-C). MACE-free survival was also compared according to use of nitrates by uric acid groups (Fig. 2D-F). In group I, patients who received nitrate therapy had a higher incidence of MACE than patients without nitrate therapy (P < 0.001) (Supplementary Table 1).
Table 1
Baseline characteristics of patients according to uric acid level
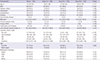
Values are expressed as the median (interquartile range) or No. (%). Patients were categorized according to tertiles of uric acid level: group, I ≤ 4.8 mg/dL; group II, 4.9–5.9 mg/dL; and group, III ≥ 6.0 mg/dL.
BMI = body mass index, PAOD = peripheral arterial occlusive disease, CV = cardiovascular, HDL = high-density lipoprotein, LDL = low-density lipoprotein, VSA = vasospastic angina, CCB = calcium channel blocker.
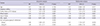
Table 2
Clinical outcomes of the total population according to uric acid level

Values are expressed as No. (%). Patients were categorized according to tertiles of uric acid level: group, I ≤ 4.8 mg/dL; group II, 4.9–5.9 mg/dL; and group, III ≥ 6.0 mg/dL. Group II was used as a reference group for analysis.
HR = hazard ratio, CI = confidence interval, MACE = major adverse cardiac events, MI = myocardial infarction, BMI = body mass index.
*Adjusted covariates were sex, smoking, BMI, serum creatinine level, and statin use. †Adjusted covariates were sex and serum creatinine level. ‡MACE was a composite of cardiac death, acute MI, ischemic stroke, revascularization, and rehospitalization for recurrent angina during follow-up.
Fig. 2
MACE-free survival curves of total (A), pure VSA (B), and mixed angina (C) patients according to uric acid tertile and MACE-free survival curves of group I (D), group II (E), and group III (F) patients according to the use of nitrates.
MACE = major adverse cardiac event, VSA = vasospastic angina.

Cox proportional hazard model analysis identified 6 prognostic factors in univariate analysis. Seven variables were included in multivariate analysis. Family history of CV disease, lower uric acid tertile, low HDL cholesterol level, mixed angina, and prescription of nitrates at discharge were significant prognostic predictors of MACE incidence (Table 3).
Table 3
Prognostic factors for MACEs
Discussion
In the present study, we investigated the association of serum uric acid levels and clinical outcomes in VSA patients with or without significant coronary artery stenosis confirmed by spasm-provocation test. The major findings of our study were: 1) patients in group II (middle tertile) showed a higher MACE-free survival than the other 2 groups, 2) this pattern was observed for only pure VSA, not mixed angina, and 3) patients who received nitrate therapy at discharge had worse clinical outcomes than those without nitrate therapy in group I (lower tertile), but not in group II or III.
It has been reported that hyperuricemia is associated with CV disease as a risk factor or disease consequence. Because the association can be readily confounded by other CV risk factors, several studies have published conflicting results (1231314) and a number of researchers tried to elucidate the underlying mechanisms of the relationship between hyperuricemia and CV disease. The mechanisms include a compensatory uric acid increase as an antioxidant, stimulated inflammation and vasoconstriction by hyperuricemia, and activation of the renin-angiotensin system in response to elevated uric acid (2515). On the other hand, a J-shaped relationship between serum uric acid and CV events, which could be explained by hypouricemia-induced endothelial dysfunction, were reported (47); and previous studies reported that uric acid administration restored endothelial function or increased serum antioxidant capacity (1617).
Unlike the relationship between obstructive coronary artery disease and serum uric acid level, the impact of uric acid on clinical outcomes in VSA has not been evaluated to date (123). We investigated if low or high serum uric acid levels would adversely affect clinical outcomes in VSA because endothelial dysfunction is known to be the main pathophysiology of the disease. To the best of our knowledge, this is the first study to analyze the association between uric acid level and clinical outcomes in VSA. Our results showed that patients in group II (middle uric acid tertile) had higher MACE-free survival than the other 2 groups. This pattern was consistent only in patients with pure VSA, not with mixed angina. Differing results for VSA according to the presence of a significant fixed lesion might be explained by the relative contribution of endothelial dysfunction as the main pathogenesis of each type of VSA. It is comprehensible that group III (upper uric acid tertile) showed worse outcomes, taking into account the known relationship between hyperuricemia and CV events. Worse clinical outcomes in group I (lower uric acid tertile) patients may be predictable as well considering the link between hypouricemia and endothelial dysfunction (71617). We also performed survival analysis according to use of nitrate for each uric acid group. Interestingly, in the lower uric acid group, patients treated with nitrate had worse clinical outcomes than patients treated without nitrate; no difference was seen for the middle and upper uric acid groups. A possible explanation for this result could come from a study that investigated low uric acid level in women with type 1 diabetes in conditions of oxidative stress represented by increases in oxidative stress metabolites. The study found that increased oxidative stress was linked to reduced plasma uric acid level that is probably caused by nitric oxide (NO) overproduction (18). Accordingly, we assumed that additional nitrate therapy might harm VSA patients with low uric acid levels by impeding production of the antioxidant uric acid further in a situation in which NO level is already increased. This process could enhance oxidative stress, resulting in poorer clinical outcomes, particularly rehospitalization due to recurrent angina, in VSA patients with low uric acid level.
This study had several limitations. First, this was a retrospective, observational study with a single-center cohort. There could be missing confounders that we could not assess from retrospective data collection. And the choice of antianginal medication was left to each physician's discretion. Second, the proportion of women was significantly higher in group I than the other groups. This might be the consequence of sex differences in baseline uric acid levels, which are usually lower in women (192021). The lower prevalence of smokers, BMI, and serum creatinine levels in group I might be explained in the same manner. Though we performed multivariate analysis to overcome this limitation, a prospective study is needed to investigate the causal relationship between uric acid level and clinical outcomes in VSA. Third, previous studies investigated prognostic role of uric acid in CV disease by only using uric acid level at admission (2223). Similarly, we could not assess the association of follow-up uric acid level with clinical outcomes because routine follow-up of blood test was not mandatory. Finally, our results cannot be simply explained by a single specific mechanism. The pathophysiology of VSA is not fully understood and hypouricemia-induced endothelial dysfunction has not been proven in the coronary artery. Despite these limitations, we believe our results have clinical implications as the first study suggesting an association between serum uric acid level and clinical outcomes in VSA.
Low or high uric acid level seems to be related with adverse clinical outcomes in pure VSA patients. In particular, patients with low uric acid level had higher incidences of adverse clinical outcomes driven by revascularization compared with those with other uric acid levels. Furthermore, use of nitrate was associated with increased rehospitalization rate due to recurrent angina in patients with low uric acid level. Therefore, it requires careful use of nitrate in VSA patients with low uric acid level.
 XML Download
XML Download