

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recently, early diagnosis and intervention has become an important topic. A systematic review showed that early intervention programs for high‑risk preterm infants have a positive influence on motor outcomes until 3 years of age, but not beyond (1). Given the phenomenon of neuroplasticity, interventions at an earlier stage might be beneficial; however, there are no definitive guidelines regarding the extent or intensity of treatment. When designing intervention programs, it is important to include or exclude patients on the basis of their age and other characteristics; the extent and duration of any treatment must also be taken into consideration.
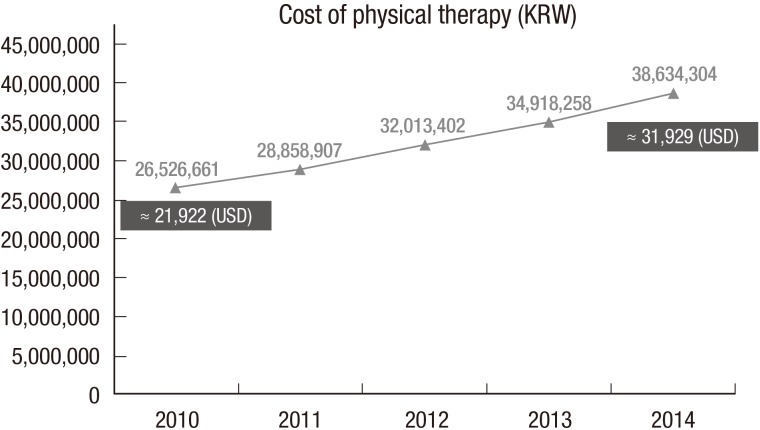
Many children with developmental delay receive rehabilitation therapy in hospitals in Korea, and intensive rehabilitation therapy is widely adopted nowadays. According to the database of Health Insurance Review & Assessment Service (HIRA) and Ministry of the Interior of Korea, the cost of physical therapy of children and adolescents (< 20 years old) is steadily increasing, from 26,526,661 in 2010 to 38,634,304 (KRW) in 2014 (Fig. 1), which is approximately 21,922 and 31,929 (USD), respectively. However, the number of population decreased from 11,584,399 (22.93% of total population) in 2010 to 10,580,278 (20.61%) in 2014 (2). The cost of physical therapy has increased about 45.6%, though the actual number of population has decreased. There is no definite analysis about the reason of this increase, however several factors might have contributed. High risk children such as prematurity have increased, importance of early intervention is widely accepted for both specialists and caregivers, and increased chance of intensive therapy as inpatient patients are possible causes of this phenomenon.
Developmental delay can occur through various etiologies. Cerebral palsy (CP) is one of the major causes of developmental delay, for which various clinical features are due to damage of the immature brain. Movement and posture impairment are common, and sensation, perception, cognition, communication, behaviour, and musculoskeletal problems are often present in children with CP (3). Chromosome abnormality, congenital anomaly, and traumatic injuries, etc. also could cause developmental delay. Various therapies are recommended for majority of children with developmental delay, although the choice is often influenced by individual socioeconomic status, accessibility to rehabilitation facilities, and national policy. Conventional rehabilitation treatment for children with CP or developmental delay includes physiotherapy (PT), such as neurodevelopment therapy, occupational therapy, and speech therapy (4). In Korea, the cost of physical therapy is covered by national health insurance, thus accessibility is relatively good from an economic point of view though patients need to pay for some of the expenses.
The effect of rehabilitation therapy may be dependent on the intensity of treatment. In a meta-analysis, intensive therapy tended to have greater effects on functional motor outcomes (with modest effect sizes) than non‑intensive therapy (5). There is no precise consensus regarding the intensity and duration of intensive therapy, or concerning ‘intensive rehabilitation.’ In addition, the form that intensive rehabilitation treatment takes may vary according to regional facilities, manpower and medical care systems. Previous studies typically specified a treatment frequency of more than 3 times a week and treatment session durations of 45 minutes to 4 hours a day, completed over several weeks as intensive programs (56789). However, there is no consensus on the optimal frequency and duration of rehabilitative therapy for children with developmental delays, including CP. In addition, indications for intensive therapy, efficacy, and factors influencing outcomes remain unclear.
The aim of this study was to explore the short‑term effects of comprehensive intensive rehabilitative therapy on gross motor function in miscellaneous developmentally delayed children, including those with CP, and to identify factors that influence the effect of intensive rehabilitative programs.
MATERIALS AND METHODS
All participants in this study received voluntary intensive rehabilitation therapy for 8 weeks in the rehabilitation department of St. Vincent's Hospital. Our program included a total of 2 hours of therapy conducted by a therapist (with a break every 30 minutes) and 1 hour of self-therapy programs, such as ergometer exercises or standing at a stander, etc.; the self‑therapy was also supervised by therapists in a hospital setting. Therapy sessions took place daily for 8 weeks. Indications for our intensive treatment program were an age of less than 7 years plus developmental delay requiring both physical and occupational therapies. The decision to participate in the program was made on the request of a caregiver or the recommendation of a physician after sufficient discussion.
Intervention programs were individualized according to the patient's development and condition; however, there were also several common principles.
● Principles of the rehabilitation program
1) Functional goal‑directed training, focusing on specific activities that are important in the developmental milestones of each child.
2) During the first week of treatment, parents were asked about their overall goals during the 8 weeks of therapy, and this information was shared with the pediatric rehabilitation team. Patients' goals, ongoing therapies, and any change in, or new information pertaining to, the patients were shared and discussed weekly among physicians and therapists.
3) Application of neurodevelopmental therapy encompassing motor learning concepts.
4) Standing at the standing frame, or exercising on the cycle ergometer, daily.
Clinical information was collected during the treatment course, including age and sex, as well as birth, seizure, medication, and botulinum toxin injection histories. Measurements of gross motor functions were performed using the Gross Motor Function Measure-88 (GMFM-88) and Gross Motor Function Classification System (GMFCS), and were obtained at the start and end of the course. GMFM-88 is a reliable tool to detect changes in gross motor function in children with CP (10). The GMFCS is validated and reliable tool that categorizes individuals with CP into one of 5 levels based on each child's motor function, from I (mildly affected) to V (severely affected) (1112). To check general developmental status, we applied the Bayley Scales of Infant and Toddler Development (3rd edition, Bayley-III) or the Gessell Developmental Test, depending on developmental age.
Statistical analysis
Statistical analyses were performed with R (R Foundation for Statistical Computing, Vienna, Austria) and SPSS for Windows software (ver. 21.0; SPSS Inc., Chicago, IL, USA). Participants were classified into 3 groups according to the cause of the developmental delay: CP, genetic disorder, or unknown etiology. All patients were evaluated using the Bayley-III and developmental quotient (DQ) was calculated as developmental age/chronological age (corrected age) × 100 based on the cognitive and language scales (receptive communication) that are the subscales of Bayley-III.
GMFM-88 scores at weeks 1 and 8 of the therapy course were analyzed using a paired t-test. Differences between each groups' GMFM-88 score were analyzed using one-way analysis of variance (ANOVA) according to diagnosis and GMFCS level. The post-hoc tests were done to identify the pairs of means that differ. Good and poor responder groups were defined as those in the top and bottom 25% in terms of difference in GMFM-88 scores, respectively. For analysis purposes, GMFCS levels were stratified into 3 groups: levels I–II, level III, and levels IV–V. Univariable and multivariable logistic regression analysis was performed in sequence to explore the factors associated with a good or poor response to intensive treatment.
RESULTS
Of the 145 cases receiving 8 weeks of intensive rehabilitation treatment between July 2011 and November 2015, we excluded those who had poor compliance for treatment or evaluation (n = 9). For patients (n = 30) who took part in more than one session (27 patients completed the course twice, 3 patients completed it 3 times), data from the first treatment session were included, thus, 30 cases were selected among 63 cases. Finally, therefore, 103 patients' data were reviewed retrospectively.
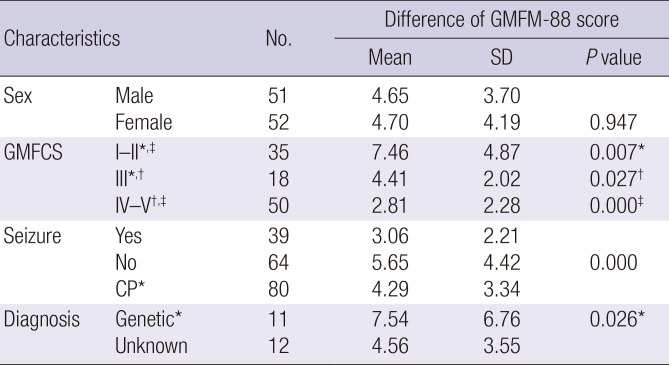
The mean age at treatment initiation was 32.62 ± 14.56 months and the mean corrected age was 31.09 ± 14.53 months (range: 5–65 months). In total, 51 of the 103 patients were boys; 80 patients were diagnosed as CP, 11 had genetic abnormalities, and 12 had developmental delays of unknown etiology. In total, 58 patients were born prematurely, 39 had combined seizure disorders, and 19 of 73 spastic patients had received a botulinum toxin injection during, or 1 month before, the treatment course. Demographic characteristics of patients and mean differences in GMFM-88 scores are shown in Table 1.
Table 1
Characteristics of patients and the difference in GMFM-88 score among groups (n = 103)
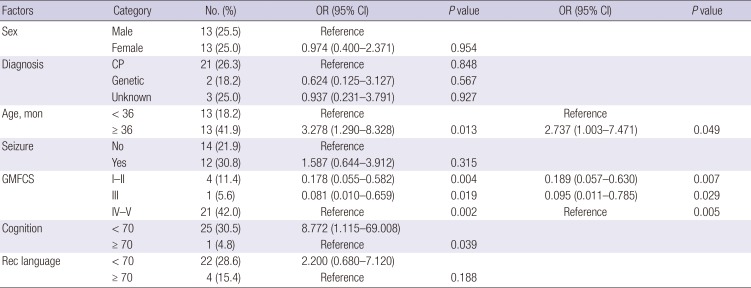
The mean difference in GMFM-88 score after 8 weeks of therapy was 4.67 ± 3.93 (P < 0.001). There was no significant difference in changes in gross motor function according to diagnosis (P > 0.05). There were 16, 19, 18, 23, and 27 patients categorized as GMFCS levels I to V, respectively. The mean differences in GMFM-88 score, pre- vs. post-8-week treatment course, were 5.80 ± 3.59, 8.86 ± 5.43, 4.41 ± 2.02, 3.46 ± 2.72, and 2.26 ± 1.69 for patients categorized as GMFCS levels I to V, respectively (Fig. 2). Children with a GMFCS level of II showed the greatest changes in GMFM-88 scores; the magnitude of change was statistically significantly larger compared to those with GMFCS levels of III (P = 0.001), IV (P < 0.001), and V (P < 0.001). Concerning the good vs. poor responders, a mean change in GMFM score of 6.18% or more represented the top 25th percentile, and a mean change of 2.24% or less represented the bottom 25th percentile. In the univariable analysis, absence of seizure disorder (P = 0.002), a GMFCS level of I–II compared to IV–V (P < 0.001), and absence of cognitive impairment (cognition DQ ≥ 70, P = 0.030) were the factors significantly associated with a good response to intensive treatment. In multivariable analysis, only GMFCS level (I–II vs. IV–V; odds ratio [OR] = 7.763, 95% confidence interval [CI] = 2.177–27.682, P = 0.002) was significantly associated with a good response (Table 2). In the poor responders group, univariable analysis showed that older age (≥ 36 months; P = 0.013), GMFCS level (IV–V vs. I–II or III; P = 0.002) and cognitive impairment (cognition DQ < 70; P = 0.039) were significantly associated with a good response (Table 3). In the multivariable analysis, older age (≥ 36 months; OR = 2.737, 95% CI = 1.003–7.471, P = 0.049) and GMFCS level (I–II vs. IV–V; OR = 0.189, 95% CI = 0.057–0.630, P = 0.007; and III vs. IV–V; OR = 0.095, 95% CI = 0.011–0.785, P = 0.005) were significantly associated with a poor outcome (Table 3).
Fig. 2
Differences in GMFM-88 score after 8 weeks of intensive therapy according to the GMFCS level.
GMFM = gross motor function measure, GMFCS = gross motor function classification system.
*,†,‡,§The post-hoc tests to identify the pairs of means that differ, P<0.05.
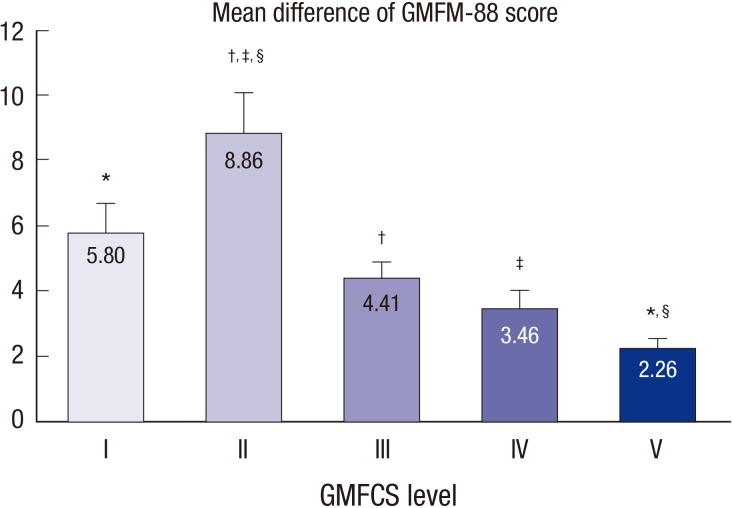
Table 2
Prognostic factors associated with a good response to intensive therapy in terms of gross motor function (n = 25)
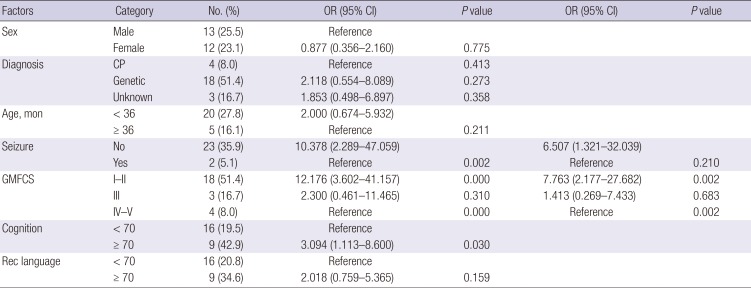
Table 3
Prognostic factors associated with a poor response to intensive therapy in terms of gross motor function (n = 26)
Botulinum toxin injection, during or 1 month before the intensive rehabilitation program, was not associated with a better GMFM-88 score among 73 spastic CP children, with a mean difference in score, pre- vs. post-treatment course, of 3.89 ± 2.36 and 3.85 ± 3.22 in the injection (n = 19) and non-injection groups (n = 54), respectively (P = 0.962).
DISCUSSION
Previous studies have shown that intensive PT can have an effect in developmentally delayed children, including CP patients (5678913141516). Our results showed a significant change in GMFM-88 score, of 4.67 ± 3.93, after 8 weeks of therapy. However, there is no absolute value of GMFM score change by which to define the success or failure of the treatment. According to the GMFM user's manual, mean score changes of 5.2% and 7.0%, according to the ratings of parents and therapists, respectively, on the GMFM-88 correspond to a moderately positive functional change. Concerning gross motor function change, parents judged a small positive change with a mean of 2.7% and therapists judged a small positive or no change with a mean of 1.3% (17). In one study, a ± 4% change in GMFM score was considered a clinically significant change (6). Therefore, in the present study, good and poor response groups were defined by GMFM-88 change score quartile: those in the top 25th percentile were considered good responders and those in the bottom 25th percentile were considered poor responders. The mean difference in GMFM-88 scores, pre‑ vs. post‑intervention, in the good response group was 6.18%, which exceeded the threshold for a moderately positive change (according to parents' ratings) described in the user's manual. The mean change in GMFM-88 scores in the poor-response group was 2.24%. A change of less than 1.3%, indicative of a small positive or no change (according to therapists' ratings), was observed in 16 children (15.6%). The majority (93.8%, 15/16) of these patients had a GMFCS level of IV or V; the remaining patient was GMFCS level III.
Our results consistently showed that ambulatory children had a better response to the intensive treatment program compared to non-ambulatory children. This indicates that the main factor affecting the impact of intensive therapy on gross motor function is GMFCS level. Children with GMFCS levels of I–II were significantly more likely to be good responders, and less likely to be poor responders, compared to those with GMFCS levels of IV–V. In an individualized analysis, children with a GMFCS level of II showed the best outcomes, followed by those with levels I, III, IV, and V. Children with a GMFCS level of I showed a significantly better response compared to those of level V, but no significant difference compared to those with levels of III and IV. Because of a measurement ceiling effect, GMFCS level I children may have showed less change compared to those of level II.
The development of gross motor function plateaus at around 6 or 7 years of age in CP children, although their final motor abilities and exact ages of functional growth differ according to GMFCS level (1819). The participants in this study were all relatively young (aged below 7 years), and thus still had the potential for functional motor improvement. Multivariate analysis revealed that the older children (≥ 36 months) were more likely to show a poor response compared to the younger children. However, this result should be interpreted cautiously, since developmental changes in gross motor function generally occur much before 3 years of age. Because there was no control group, it is difficult to conclude that the intensive program had substantial effects on gross motor function over and above natural development, or non-intensive therapy, although a significant change in score was observed by the end of the 8‑week program. Because of ethical issue, it is difficult to conduct a randomized controlled study about intensive therapy vs. no-therapy. Most studies were conducted by comparing different programs or with cross-over design. In a study comparing 4-week intensive training programs for CP children aged between 3 and 16 years, small improvements in gross motor function were seen regardless of the program (6). In a study that included 5 infants (< 1 year of age) newly diagnosed with CP, the effect of intensive PT (two 4-week programs of daily PT separated by 8 weeks of usual PT) was inconclusive (8). Further studies may be required to ascertain if there is any additive effect of intensive rehabilitation therapy in actively developing children.
At present, botulinum toxin A is commonly used to control spasticity in children with CP, and there is sufficient evidence to support botulinum toxin A injection into spastic muscles (2021). This improves gait pattern and function by reducing spasticity in ambulatory children with spastic CP (212223). Unexpectedly, botulinum toxin injection into the muscles of the lower extremities did not have any additional effect on GMFM score improvement among the spastic CP children included in the present study. However, only 26% (19/73) of our patients received an injection; this relatively small number of patients may have contributed to the lack of effect. Furthermore, the majority of children (12/19, 63%) who underwent injections had GMFCS levels of IV–V (6 patients were level I–II [31%], and 1 was level III). In a systematic review by Pin et al. (24), most studies on the use of botulinum toxin A in children with severe CP (GMFCS levels of IV–V) were of poor methodological quality and the evidence of beneficial effects was limited. However, botulinum toxin A was found to be beneficial in terms of the ease of care and comfort of non‑ambulatory children (25). Our study evaluated only gross motor function and not pain, comfort, or ease of care. Thus, we were unable to identify any other positive effect of botulinum toxin injections.
Epilepsy is accompanied in 32.5% of children with CP, and epilepsy and intellectual impairment are common comorbidities (26). Comorbidities including seizures are more common in non‑ambulatory children; namely, those with GMFCS levels of IV–V (2627). The prevalence of epilepsy was 37.9% among all participants in the present study, rising to 48.5% in non‑ambulatory children; these data are not different to those of previous reports. Seizure itself and anti-epileptic drugs have detrimental effects on motor and cognitive function (28). In the present study, seizure disorder comorbidity had a significant detrimental effect on rehabilitation treatment effectiveness in the univariate, but not the multivariate, analysis.
This study has some limitations. First, the GMFM-88 was applied to measure gross motor function not only in patients with CP, but also in children with other genetic disorders and developmental delay of unknown etiology. Although the GMFM-88 has been applied to various groups of children with motor difficulties (2930), it has been validated for use only in children with CP and Down's syndrome. Second, there was no control group; thus, although our results indicate that the intensive rehabilitation programs improved gross motor function, we do not know how significant this improvement would have been compared to non-intensive treatment or natural growth. The patients were relatively young, with a mean age of 31.09 ± 14.53 months, and their growth curves pertaining to gross motor function showed relatively steep slopes. Third, there was no follow-up evaluation after the intensive rehabilitation program and observation period was relatively short. Therefore, the persistence of the effects and long-term effects remains unknown.
In this study, a change in the gross motor function (4.67 ± 3.93), measured by GMFM-88 was observed after 8 weeks of intensive rehabilitation therapy in children with developmental delay, including CP. However, additive impact including cost effectiveness compared to usual therapy or non-therapy is inconclusive due to lack of control group. Although there were several limitations, our results have implications with respect to prognostic factors of intensive rehabilitation therapy in children showing developmental delays. GMFCS level is the most important prognostic factor of intensive therapy for gross motor function, in children with CP or developmental delay due to miscellaneous causes. In addition, children aged more than 36 months are more prone to poor gross motor outcomes compared to children younger than 36 months.
 XML Download
XML Download