

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Playgrounds are places that contribute to children's physical development and social skills. Many countries have introduced safety guidelines to prevent injuries associated with playground equipment and collected information of playground equipment related injuries. According to a report published in the United States, over 210,000 children under the age of 18 years are treated in hospital emergency rooms for injuries such as contusions, lacerations, and fractures caused by falls, slips, and collisions on playgrounds (123). Compared to school-aged children, preschool-aged children are more prone to accidents on playgrounds because they are not only less capable of physical control, but also unaware of risk and lack of proper judgment (4). A Korea-based report revealed that injuries associated with playgrounds accounted for 6.9% of total injuries sustained by preschool-aged children, but the hospitalization rate for such injuries was the highest at 7.7% (5).
Injuries associated with playground equipment involve various human factors, in that preschool-aged children are less physically and mentally developed, equipment factors, in that such injuries are caused by swings, slides, seesaws, and horizontal bars (67), environmental factors, like the presence of child protection devices or caregivers (89), and social factors, in that playgrounds are public facilities managed by social organizations or local autonomous entities (10). In these aspects, various researches about playground injuries in children have been reported. However, existing reports did not fully examine the mechanism related to severity of injuries, or were not large enough in scale including preschool-aged children.
Against this backdrop, this study investigated the mechanism of various injuries associated with playground equipment, the injury-inducing factors, and the severity of injuries among preschool-aged children. The objective was to examine the characteristics of injuries according to each playground equipment, as well as the frequency and odds ratio (OR) of traumatic brain injuries and upper/lower extremities fracture associated with playground equipment.
MATERIALS AND METHODS
The subjects were patients registered in the Emergency Department-based Injury In-depth Surveillance (EDIIS), which collected real-time data on patients in the emergency rooms of 20 designated local emergency medical centers from January 1, 2011 to December 31, 2014. This study focused on cases of children under the age of 7 with the playground equipment as the injury-inducing factor or direct cause of injury. The analysis excluded cases in which the playground equipment related to injuries were unidentified, cases with unknown injury mechanisms or injured body parts, and cases with unclear or unknown diagnosis. Finally, selected patients were examined by gender, age, injury-inducing factor, injury mechanism, injured body part, diagnosis, results of emergency treatment, and post-hospitalization results, retrospectively.
Previous research on injuries among preschool-aged children have found that children in 0–2 years are prone to traumatic brain injury (TBI), while those above the age of 3 are prone to upper extremity fractures, so we categorized patients by 2 years old (111213). Injury mechanism was classified into collision, slip, fall, penetrating trauma (scratch, cut, tear, penetration, stab), overuse of the body, and miscellaneous (temperature-related injuries, tracheal compression, contact with foreign substances). Playground equipment were categorized into swings, seesaws, slides, climbing equipment such as playground gyms and monkey bars, and other types of equipment (horizontal bars, tightropes, trampolines, parallel bars, rocking horses). The injured body parts were head and neck, trunk, upper extremity, and lower extremity. Based on the Korean Standard Classification of Diseases (KCD6), major diagnosis was classified into contusion, sprain, dislocation, laceration, fracture, internal organ injuries, TBI, and other injuries (crushing injury, muscle and tendon injury, burns, foreign substances). In multiple injuries, we selected more severe injuries as a major diagnosis, and if there is same diagnosis of different body parts, we selected major diagnosis as guideline in EDIIS. Results of emergency treatment were discharge, admission, emergency operation, and transfer. TBI was defined as a concussion or loss of consciousness accompanied by external head injury or cerebral hemorrhage (1415), while upper and lower extremity fractures were limited to cases involving fractures in accordance with KDC6. The analysis covered characteristics of injuries associated with playground equipment among preschool-aged children, factors influencing TBI, factors influencing upper extremity fractures, and factors influencing lower extremity fractures.
The SPSS 20 (IBM Corp., New York, NY, USA) was used for statistical analysis. Continuous variables were expressed in average and standard deviation, and categorical variables in frequency and percentage. The independent t-test was employed for continuous variables, and Pearson's χ2 analysis was used followed by binary logistic regression analysis for categorical variables. The P < 0.05 was considered statistically significant.
Ethics statement
This study was reviewed and approved by the Institutional Review Board of Inje University, Ilsan Paik Hospital (ISPAIK 2016-02-015) and satisfied requirements specified under the Ministerial Decree of Health and Welfare and passed by the National Bioethics Committee. Informed consent was waived by the board.
RESULTS
Characteristics of injuries associated with playground equipment
Among the 233,960 patients, there were 8,321 patients with injuries related to playground equipment. We excluded 1,207 patients in which playground equipment were unspecified, 142 patients with unclear injury mechanisms, and 862 patients with unclear diagnosis or body parts. The total number of included patients was 6,110 (Fig. 1).

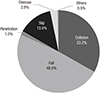
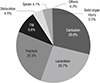
Among the 6,110 patients, 3,567 (58.4%) were males and 2,543 (41.6%) were females. The average age was 4.14 ± 1.95. The number of patients by injury mechanism was 2,966 (48.5%) for falling down, 2,026 (33.2%) for collisions, and 824 (13.5%) for slips (Fig. 2). Injuries to the head and neck were the most common, amounting to a total of 3,460 cases (56.6%), followed by the upper extremity with 1,826 cases (29.9%). By major diagnoses, there were 1,761 (28.8%) with contusions, 1,631 (26.7%) with lacerations, 1,558 (25.5%) with fractures, and 597 (9.8%) with TBI (Fig. 3). By equipment type, 2,475 cases (40.5%) were associated with slides, 1,210 cases (19.8%) with other types of equipment such as horizontal bars, tightropes, parallel bars, and rocking chairs, 953 cases (15.6%) with climbing equipment, and 370 cases (6.1%) with seesaws (Fig. 4).

The analysis of the type of equipment in relation to injury mechanism and injured body parts showed that falls were prevalent on swings (635 patients, 57.6%), which mostly resulted in injuries to the head and neck (751 patients, 68.1%). Falls were also prevalent on slides (1,087 patients, 43.9%), which mostly resulted in injuries to the head and neck (1,442 patients, 58.3%). Collisions were prevalent on seesaws (236 patients, 63.8%), mostly causing injury to the head and neck (253 patients, 68.4%). Collisions were prevalent on other types of equipment (480 patients, 39.7%), causing injury to the head and neck (599 patients, 49.5%), while falls were prevalent on climbing equipment (692 patients, 72.6%), leading to an injury to the upper extremity (419 patients, 44.0%) (Table 1).
Table 1
Characteristics of injuries by type of playground equipment

As for the results of emergency treatment, 5,502 patients (90.05%) were discharged, 27 (0.44%) were transferred, 77 (1.26%) received emergency operation, and 504 patients (8.25%) were hospitalized. Among the patients who received emergency surgery, 2 deaths occurred. The average age of 608 hospitalized patients, including those who received emergency surgery or transferred to other institutes, was 5.00 ± 1.66. This was higher than the average age of discharged patients at 4.04 ± 1.95. The most common injury mechanism was falls, associated with 500 patients (82.2%). The type of equipment involved in injuries, in descending order, were slides (206 patients, 33.9%), climbing equipment (177 patients, 29.1%), and other equipment (124 patients, 20.4%). The body parts involved in injuries were the upper extremity for 520 patients (85.5%), and the head and neck for 45 patients (7.4%). By major diagnosis, 547 patients (90.0%) suffered from fractures, 27 from TBI (4.4%), and 11 (1.8%) from internal organ injuries (Table 2).
Table 2
Comparisons of variables between discharge and admission in emergency department

Analysis of factors associated in TBI
The number of patients with TBI was 597, with no significant difference by gender. Among TBI patients, there were 221 (37.0%) children age 0–2 years and 376 (63.0%) age 3–7 years old. Injuries associated with falls were the highest at 64.7% (386 patients), and 46.9% (280 patients) were injured on slides (Table 3).
Table 3
Logistic regression for factors associated in TBI

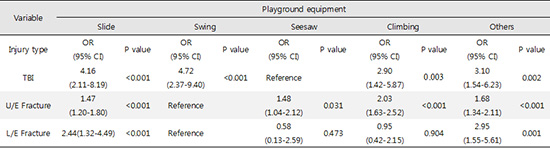
Children age 0–2 years old were 1.88 times (OR, 1.88; 95% confidence interval [CI], 1.56–2.27; P < 0.001) more likely to have TBI than those age 3–7 years old. By injury mechanism, injuries due to falls were 1.81 times (OR, 1.81; 95% CI, 1.48–2.22; P < 0.001) more likely than injuries due to collisions. Compared to injuries on seesaws, swings were 4.72 times higher (OR, 4.72; 95% CI, 2.37–9.40; P < 0.001), slides were 4.16 times higher (OR, 4.16; 95% CI, 2.11–8.19; P < 0.001), climbing equipment were 2.90 times higher (OR, 2.90; 95% CI, 1.42–5.87; P = 0.003), and other equipment were 3.10 times higher (OR, 3.10; 95% CI, 1.54–6.23; P = 0.002) (Table 3).
Analysis of factors associated in upper extremity fracture
The number of patients with upper extremity fracture was 1,285, with no significant difference by gender. Among them, there were 144 (11.2%) children age 0–2 years old and 1,141 (88.8%) children age 3–7 years old. Injuries associated with falls were the highest at 1,009 patients (78.5%), and 456 patients (35.5%) were injured on slides (Table 4).
Table 4
Logistic regression for factors associated in upper extremity fracture

Children age 3–7 years old were 3.07 times (OR, 3.07; 95% CI, 2.52–3.73; P < 0.001) more likely to have upper extremity fractures than those age 0–2 years old. Compared to injuries due to collisions, falls were 8.60 times higher (OR, 8.60; 95% CI, 6.98–10.61; P < 0.001), slips were 3.63 times higher (OR, 3.63; 95% CI, 2.78–4.75; P < 0.001), and overuse of the body was 2.18 times higher (OR, 2.18; 95% CI, 1.31–3.62; P = 0.003). Compared to injuries on swings, slides were 1.47 times higher (OR, 1.47; 95% CI, 1.20–1.80; P < 0.001), climbing equipment were 2.03 times higher (OR, 2.03; 95% CI, 1.63–2.52; P < 0.001), and other equipment were 1.68 times higher (OR, 1.68; 95% CI, 1.34–2.11; P < 0.001) (Table 4).
Analysis of factors associated in lower extremity fractures
The number of patients with lower extremity fractures was 133, with no significant difference by gender or age. Injuries associated with falls were the highest at 69 patients (51.9%), and 66 patients (49.6%) were injured on slides (Table 5).
Table 5
Logistic regression for factors associated in lower extremity fracture

Compared to injuries due to collisions, overuse of the body was 6.98 times higher (OR, 6.98; 95% CI, 3.82–12.74; P < 0.001). Compared to injuries on swings, slides were 2.44 times higher (OR, 2.44; 95% CI, 1.32–4.49; P = 0.004), and other equipment were 2.95 times higher (OR, 2.95; 95% CI, 1.55–5.61; P = 0.001) (Table 5).
DISCUSSION
In accordance with the 2007 Safety Management Act for Children's Playground Facilities, Korean Ministry of Public Safety and Security introduced ‘Facility and Technical Standards of Play Equipment for Children’ based on American Society for Testing and Materials (ASTM) F1487 of the United States, European Standards for Playground Equipment (EN) 1176–1177 of Europe, Japan Playground Facility Association Safety Standard (JPFA-S) of Japan, and domestic safety certification standards for playground facilities, thereby mandating installation inspection and regular facility inspection for all children's playgrounds (16). The Impact absorbing standards of playground floor materials is set below Head Injury Criterion (HIC) 1000 for preventing head injury. The free fall height is set below 4 meters in case of hands support and below 3 meters in case of feet support. Handrail supports, if accessible by children under the age of 36 months, must be between 1 and 2 meters from the ground (16).
This study, conducted at the time of expanding playground-related regulations, is expected to contribute to the prevention of injuries associated with playground equipment as falls accounted for 48.5% of injury mechanisms and 82.2% of hospitalization. However, the high rate of fractures (90.9%) for hospitalized patients indicates that safety regulations might have been ineffective in reducing fractures, as previous reports indicated (31718). Thus, it is necessary to make a comparative study whether fractures on the playground have been reduced after applying the playground-related regulations, and reinforce safety regulations.
The analysis of factors influencing TBI revealed a relatively high incidence of injuries for children under 2 years old, injuries due to falls, and injuries on swings or slides. According to previous studies on injuries among preschool-aged children injuries, TBI is more likely to occur among children under the age of 2 and is the result of falls because children in that age tend to have proportionately heavy heads and are less physically developed (1112). The results for injuries by playground equipment were also similar. Previous study, which did not consider injury mechanisms, reported that the relative incidence of TBI was higher by 1.4 times and 1.15 times on swings and monkey bars, respectively (7). This study considered the result that primary injury mechanism of TBI at playground is fall, and found that swings had a relatively high incidence followed by slides and climbing equipment compared to seesaws which is used on the ground level. We recommended installation of safety swings like dining table chairs for children and more effective shock absorbing ground materials around swings for minimizing the severity of TBI.
The analysis of factors influencing upper extremity fractures revealed a relatively high incidence of injuries for children over 3 years old and injuries due to falls (1319). Upper extremity fractures are presumed to be more common when shock is absorbed by the upper extremity since falls occurred on equipment above a certain height such as climbing equipment, other equipment, and slides. Falls accounted for 57.6% of injuries on swings, but the OR was the lowest. This is because the upper extremity remains in a fixed posture when riding swings, thus lowering the possibility of fractures to the upper extremity, even if falls occur.
The analysis of factors influencing lower extremity fractures revealed a relatively high incidence of injuries for overuse of the body, as well as on other equipment such as horizontal bars, parallel bars, and trampolines. Previous studies have associated more severe injuries with falls from playground gyms, monkey bars, and trampolines (20). The overuse of the body is presumed to be the primary injury mechanism rather than falls, considering that other equipment such as horizontal bars, parallel bars, and trampolines involved jumping or landing on the ground.
The limitations of this study are as follows. First, it focused on patients who visited emergency rooms after sustaining injuries, and excluded cases with unclear injury mechanisms, body parts, and primary injuries. The selected subjects do not represent all cases of injuries associated with playground equipment as some victims may have visited smaller medical institutes or received non-emergency treatment. Second, the EDIIS does not take into account factors such as presence of caregivers, height of falls, and floor materials. These are known to be important environmental factors of injuries occurring on playgrounds (8212223). One study found that the relative incidence of injury for falls from a height greater than 2.0 m was 2.56 times that of falls from a height below 1.5 m, and a relative incidence also increased by 2.26 times when hard floor materials were involved (23). Third, this study only considered injuries associated with playground equipment, and excluded cases of collisions between children on playground equipment. Further research is required on this aspect as safety standards have been developed for space within equipment and space between equipment.
This study analyzed the characteristics of injuries associated with playground equipment, factors influencing TBI, upper extremity fractures, and lower extremity fractures in preschool-aged children under the age of 7. Many of the injuries associated with playground equipment involved falls and occurred on slides. TBI was most prevalent among children 0–2 years old, usually involved falls, and occurred on swings. Upper extremity fractures were prevalent among children in 3–7 years old, usually involved falls, and occurred on climbing equipment. Lower extremity fractures were caused by overuse of the body, and occurred on other types of equipment such as horizontal bars, parallel bars, and trampolines.
 XML Download
XML Download