

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Influenza is responsible for substantial global morbidity and mortality every year. Worldwide, annual epidemics are estimated to result in about 3 to 5 million cases of severe illness and approximately 250,000 to 500,000 deaths (1). Studies conducted in the Western Pacific and South East Asian regions indicate that the burden of influenza-related hospitalization and death is substantial, and comparable to the United States and Europe (23456789). In the Republic of Korea (ROK), annual data from the Korea Centers for Disease Control and Prevention in patients of all ages indicate that 10%–12% of influenza-like illness (ILI) cases are positive for influenza (101112). Despite the availability of these data and the wide recognition of influenza as public health threat, estimation of its true burden and its complications, particularly social and quality of life, is still limited in Asia.
Recognition of differences in severity, outcomes and social and medical burden between people with laboratory-confirmed influenza (LCI) illness and non-influenza acute respiratory illness (ARI) is necessary to assess the true disease burden and the benefit of an influenza vaccination program. Here we present the results of 2 studies covering the 2007–2008 and 2008–2009 influenza seasons aiming to determine the frequency of LCI in older adults with an ARI in the ROK and to assess differences in medical and social outcomes among ARI patients with and without LCI.
MATERIALS AND METHODS
Study design and participants
These prospective, observational cohort multicentre studies (GlaxoSmithKline [GSK] identifier No. 110938 and 112519) were performed during 2 consecutive influenza seasons at 5 local clinics and 2 university hospital outpatient clinics in the ROK: Inha University Hospital and Hallym Medical Center in Incheon, Korea University Guro Hospital and Uni Medical Clinic in Seoul, Howon Silver Hospital and Onnuri Hospital in Ansan, and Hur's Hospital in Gwangmyeong. Most patients (approximately 96%) were enrolled from the local clinics. The university hospitals enrolled patients who visited the ambulatory outpatient clinic; they did not enrol patients who visited the emergency room or were admitted to hospital. All sites involved were located in Seoul metropolitan area covering 48%–50% of the ROK population. The influenza season was defined as the period beginning on the Monday of the week when the first influenza case was identified among study participants until the moment when no influenza cases could be identified for 2 consecutive weeks. Based on this definition, the studies were conducted between 19 November 2007 and 19 May 2008 (the first study) and between 4 December 2008 and 18 June 2009 (the second study). All adults ≥ 50 years of age consulting a physician for ARI at the selected centres were invited to participate. Patients were enrolled starting from the week when the first case of influenza was identified. ARI was defined as an illness consisting of fever defined as axillary temperature ≥ 37.5°C, and/or feverishness (subjective feeling of fever and/or chills as reported by the patient), and at least one other of the following: coryza and/or nasal congestion, sore throat and cough (131415). There was no exclusion criterion for enrollment; however, patients recruited before the start or after the end of the influenza season were excluded from the analysis.
During the enrollment visit, the following data were recorded for each study participant: demographic information (date of birth, gender), influenza vaccination status (history of influenza vaccination for the present season and during the previous three years), and presence of any chronic disease, the type and posology of any medications used for the ARI. Additionally, a physical examination was performed and 2 clinical samples (nasal swabs or washes, or throat swabs) were collected for each patient for laboratory confirmation of the influenza cases.
The follow-up contact was performed by phone or face-to-face meeting 12–21 days later to record the number of ARI-related medical visits over the interval since enrollment, use of prescribed or non-prescribed medication, occurrence of complications; number of days of reduced activity; number of days missed from work; hospitalization for ARI-related reasons over the interval since the enrollment visit; ARI episode outcomes. The follow-up was performed using questionnaires and all variables recorded were self-reported by patients. Medications were reported by class (e.g. antiviral, antibiotic, antipyretic) and were not otherwise specified.
Laboratory assays
The laboratory confirmation of influenza cases was performed twice. First, 1 of the 2 samples collected for each patient was tested in the investigator's office for the presence of influenza virus using a commercially available rapid diagnostic kit able to distinguish influenza A and B (161718). The SAS FluAlert (SA Scientific, San Antonio, TX, USA) (16) was used for the 2007–2008 season and the BinaxNOW Influenza A & B Test (Inverness Medical Innovations, Inc., Livermore, CA, USA) (17) or Directigen EZ Flu A + B (Becton, Dickinson and Company, Franklin Lakes, NJ, USA) (18) were used for the 2008–2009 season. The second sample was sent to the Korea University Guro Hospital for identification and typing by culture (for both seasons) and reverse transcriptase polymerase chain reaction (RT-PCR; capillary electrophoresis-based multiplex RT-PCR assay using the Seeplex Respiratory Pathogen 18-plex Test [Seegene, Seoul, Korea]) (19); only during the second season according to local standard operating procedures.
Objectives
The primary objective in both studies was to determine the presence of LCI in patients presenting with ARI. The secondary objectives were to determine: number of days of illness, number of days of reduced activity (i.e. the patient considered that he or she was unable to do usual activities such as self-care, work or recreation), number of days of absenteeism, number of medical visits related to ARI, use of medication (prescribed or non-prescribed drugs), and the occurrence of complications (pneumonia, exacerbation of chronic lung disease, and exacerbation of congestive heart failure) and hospitalization during the follow-up period.
Statistical analysis
Based on the assumption of 20% of ARI cases being positive for influenza, a target sample size of 500 patients with ARI in each of the 2 influenza seasons was calculated with a 95% confidence interval (CI) of 16.6%–23.8%. Recruitment was estimated to end when either the target sample size had been enrolled or the influenza season had ended. Therefore, the number of enrolled patients could be less than 500 for each study. The total cohorts included all patients enrolled in the studies.
Data analysis was based on the According-to-protocol (ATP) cohorts which included all evaluable patients (i.e. those meeting all inclusion criteria and complying with the procedures defined in the protocol). Only the first ARI episode per patient was evaluated. An ARI case was defined as influenza if it was confirmed by any laboratory test (rapid test, culture or RT-PCR) from at least 1 clinical sample. Categorical variables were summarized with frequency tables. Descriptive statistics (mean, standard deviation [SD], median, interquartile range, minimum, and maximum) were computed for continuous variables. The variables were compared between LCI and non-influenza ARI patients using Fisher exact test and Mann-Whitney Wilcoxon test. These exploratory comparisons were planned for the 2008–2009 season and post-hoc for the 2007–2008 season. The exact 95% CI for a proportion within a group was calculated from Proc StatXact (Cytel, Cambridge, MA, USA). All statistical analyses were performed using SAS version 9.1 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
The studies were conducted in accordance with the Good Clinical Practice Guidelines and the Declaration of Helsinki. The study was approved by the Korea University Guro Hospital Institutional Review Board (KUGH0760). All participants signed an informed consent form that conformed to the recommendations of the IRB.
RESULTS
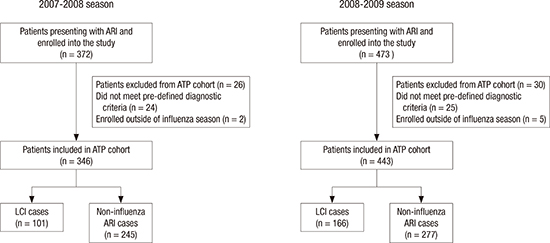
A total of 346 patients in the 2007–2008 season and 443 patients in the 2008–2009 season were included in the ATP cohorts (Fig. 1). The median participant age was 58 years in the 2007–2008 season and 60 years in the 2008–2009 season (Table 1). Of these patients, 101 tested positive for influenza (29.2%; 95% CI, 24.5–34.3) in 2007–2008 and 166 (37.5%; 95% CI, 32.9–42.2) in 2008–2009. Forty-four point three percent of the patients during the 2007–2008 season (38.1% of those with LCI and 46.7% of those with non-influenza ARI) and 46.5% of the patients during the 2008–2009 season (40.4% of those with LCI and 50.2% of those with non-influenza ARI) had been vaccinated against influenza for the seasons under the study. At least 1 influenza vaccination within the previous 3 years was reported by 54.3% of the patients during the 2007–2008 season (53.5% of those with LCI and 54.7% of those with non-influenza ARI) and 58.0% of the patients during the 2008–2009 season (52.4% of those with LCI and 61.4% of those with non-influenza ARI).
Fig. 1
Participants flow diagram.
Protocol violations: did not meet the pre-defined diagnostic criteria; Other: patients enrolled outside the influenza season.
ARI = acute respiratory illness, ATP = according to protocol, LCI = laboratory-confirmed influenza.

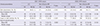
Table 1
Patient characteristics according to LCI status and season (ATP cohort)
LCI = laboratory-confirmed influenza, ATP = according-to-protocol, ARI = acute respiratory illness, SD = standard deviation, n = number of patients within a given category.
*Included emphysema/chronic obstructive pulmonary disease, previous pneumonia, asthma, immunosuppressive therapy (steroids, chemotherapy, and radiotherapy), diabetes mellitus, renal failure/dialysis, atherosclerotic cardiovascular disease/coronary artery disease, heart failure/chronic heart failure, cerebral vascular accident/stroke, human immunodeficiency virus infection, acquired immunodeficiency syndrome or CD4 count < 200, current smoker.
During both seasons, LCI and non-influenza ARI patients were similar in terms of gender, age, and proportion of patients reporting at least 1 chronic disease or pre-existing conditions (Table 1). A lower proportion of patients with LCI had received current season influenza vaccination compared with patients with non-influenza ARI (Table 1). More samples tested positive for influenza by culture than rapid test (Table 2). The analysis by influenza type showed for all age groups that influenza B accounted for the majority of influenza-related illness in the 2007–2008 season (84/101 [83.2%] of the LCI cases) while almost all influenza-related illness cases in the second season were caused by type A (164/166 [98.8%] of the LCI cases) (Table 2, Fig. 2).
Table 2
Detection of influenza by testing method
Values are presented as number (%).
n = number of patients within a given category, ARI = acute respiratory illness, LCI = laboratory-confirmed influenza, NA = not applicable (RT-PCR was not performed during the 2007–2008 season), RT-PCR = reverse transcriptase polymerase chain reaction.
*One indeterminate, 2 not tested; †One not reported; ‡Culture not done for 1 patient.

The most common presenting ARI symptom in both LCI and non-influenza ARI patients was fever/feverishness during both seasons (96.0% overall in the 2007–2008 season and 100.0% overall in the 2008–2009 season). The incidence of the most frequently reported combination of symptoms during both seasons was generally higher in LCI than in non-influenza ARI patients (Supplementary Table 1).
At the time of the enrollment during both seasons, at least 28.1% of patients reported having taken medication for ARI-related symptoms prior to enrollment and at least 96.4% of the patients in each season were prescribed at least 1 ARI-related medication at enrolment (Table 3).
Table 3
ARI-related medication taken prior to enrollment and prescribed at enrollment visit (ATP cohort)

The mean illness duration was significantly longer in LCI patients (9.7 days in 2007–2008 and 9.1 days in 2008–2009) than in non-influenza ARI ones (8.0 days in 2007–2008 and 8.1 days in 2008–2009) (Table 4). The proportion of patients who had ARI-related medical visits, were hospitalized, or reported complications due to ARI was low for both LCI and non-influenza ARI patients (Table 4). In the 2007–2008 season, none of the patients experienced exacerbation of chronic obstructive pulmonary disease (COPD) or congestive heart failure and only 3 had pneumonia, all in the non-influenza ARI group. During the 2008–2009 season, 4 non-influenza ARI patients developed pneumonia, and 1 LCI patient and 1 non-influenza ARI patient presented with an exacerbation of COPD (1 patient experienced both pneumonia and exacerbation of COPD). Similar outcomes were reported in LCI and non-influenza ARI patients during both seasons, and most of the cases were resolved at the end of the follow-up (67.6% in 2007–2008 and 76.6% in 2008–2009). No deaths were reported for either season (Table 4).
Table 4
Patient outcome at the end of the follow-up period (ATP cohort)
Complications: pneumonia, exacerbation of chronic lung disease, exacerbation of congestive heart failure.
ATP = according-to-protocol, LCI = laboratory-confirmed influenza, ARI = acute respiratory illness, N1 = number of patients with available results in a specified season, N2 (%) = number (percentage) of patients within a given category, SD = standard deviation.
*One patient experienced 2 complications.
Of the patients enrolled during the 2007–2008 and 2008–2009 seasons, 98.4% and 46.1% respectively were professionally active. In the 2007–2008 season, a significantly higher proportion of patients with LCI reported work absenteeism (51.1%) compared with patients with non-influenza ARI (25.6%) (P < 0.001; Table 5). No significant difference was observed during 2008–2009 (Table 5).
Table 5
Impact of influenza on work attendance and on the quality of life (ATP cohort)
The percentages, means (SD) and medians (range) were calculated based on the N value shown to the left (number of patients with available results).
ATP = According-To-Protocol, LCI = laboratory-confirmed influenza, ARI = acute respiratory illness, N1 = number of patients with available results in a given season, N2 (%) = number (percentage) of patients within a given category, SD = standard deviation.
In terms of quality of life, a higher proportion of LCI patients than non-influenza ARI patients reported an impact of the ARI episode on the performance of normal daily tasks but the mean number of days with reduced activity were similar (Table 5).
DISCUSSION
Our studies showed that in adults aged 50 years and older, about one third of all medically-attended ARIs included in analysis were due to influenza (29.2% in the 2007–2008 season and 37.5% in the 2008–2009 season) indicating a significant burden of disease in the elderly in ROK. Although we enrolled patients from community primary care centres and thus theoretically assessing less severe cases, our results are in the range reported for the 2011–2012 season in ROK by 2 studies enrolling patients in emergency departments (2021). These studies present data from the Hospital-based Influenza Morbidity & Mortality (HIMM) surveillance system which collects clinical data from influenza patients presenting to tertiary hospitals in ROK, and which has been recently launched (2021). Using a similar methodology (combined ILI and laboratory-based surveillance) the authors of the two studies determined a rate of 14% of LCI cases among the total number of ILI cases of all ages and 45.7% in patients ≥ 18 years of age (2021). The methodology of our study and the HIMM studies are similar regarding ILI definitions and laboratory methods, but the study sites and age range of the patients are different because we recruited patients 50 years and older from primary care, whilst HIMM recruited patients of all ages from tertiary hospitals.
Influenza A and B are major causes of respiratory illness in all age groups. More than 80% of all influenza cases were due to influenza B during the 2007–2008 season and 99% of influenza cases were due to influenza A during the 2008–2009 season. This shows that influenza B could account for a substantial proportion of the overall influenza burden in ROK and that the level of influenza B burden can be unpredictable. A high incidence of influenza B cases was also reported in the 2011–2012 season when this strain was the predominant one in ROK during the second peak period of influenza activity in this season (20). Two studies performed in tertiary hospitals in ROK during the 2011–2012 season and aiming to compare the clinical manifestations of influenza A and B reported no differences in regards to symptoms and complications in adult patients (2324). This information is particularly important because influenza trivalent vaccine contains only one influenza B lineage, and it has been shown that mismatches occur often (25). For example, in ROK during the 2011–2012 season influenza B/Victoria lineage was included in the selected vaccine but over 30% of the influenza B samples were influenza B/Yamagata lineage (26).
In our study, the majority of the patients (68.8%) were aged 50–64. This younger age distribution probably accounts for the few complications of the illness seen, even though 30% of the patients presented with at least 1 chronic medical condition at study start and we would have expected a higher number of complications in these patients. Similar to previous observations (202127), our data show vaccination rates against influenza below 50% during the seasons under study. The higher vaccination coverage in our study compared to the vaccination coverage in the ROK general population, 34.3%–35.8% before 2008 (2728), reflects the fact that free influenza vaccination is offered in ROK to people older than 65 years of age, and thus, the elderly population has greater accessibility to influenza vaccination than the younger population.
The impact of influenza on daily performance and work absenteeism was also studied. Certainly, in this study, patients with influenza reported a higher impact on daily performance and higher rates of lost work in professionally active patients aged 50 to 64 years and longer illness overall, suggesting that influenza caused more severe illness than non-influenza ARI. During both seasons, the majority of patients were prescribed ARI-related medication at enrollment. Loss of income due to work absenteeism in professionally active patients combined with the medical costs calls attention to the socio-economic impact of influenza in this population. It should be noted that work absenteeism among patients with influenza was substantially higher in the 2007–2008 season (51%) than in the 2008–2009 season (14%); the same trend was observed in patients with non-influenza ARI. We have no obvious explanation for this finding. The main difference between the 2 influenza seasons was the predominant influenza subtype: type B in the 2007–2008 season and type A in the 2008–2009 season. It is possible that this may have influenced work absenteeism.
The results of our study should be interpreted in the light of some limitations. One is the possible outcome misclassification; the definition of LCI lacked specificity by defining a case by any positive result, with some false positives thus expected. Also there was some potential of misclassification between the 2 seasons given the difference between the diagnostic methods used: PCR and culture in the 2008–2009 season which has been shown to be more sensitive than the viral culture used in the 2007–2008 season. In addition, because we recruited patients from primary care, patients who presented with respiratory complications or were directly referred to hospital were not included in our studies. Thus our data may not generalizable to influenza across the spectrum of severity.
Our results showed that influenza is an important cause of ARI in adults aged 50 and older in ROK causing more severe illness than non-influenza related ARI. Both A and B types of influenza can cause the majority of ARI and are equally important vaccine formulations as preventive measures. Higher work absenteeism and healthcare utilization were noted in persons with influenza. Therefore, there is a need for more effective strategies, such as a higher uptake of the vaccination, for the control of ARI in older adults in ROK. Influenza vaccination may decrease the burden of severe ARI in individuals above 50 years of age in the ROK.
 XML Download
XML Download