

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Adequate fluid management is one of the important therapeutic goals of dialysis because volume overload in patients on maintenance dialysis leads to increased cardiovascular morbidity and, consequently, to significantly increased mortality (1). For optimal body fluid control, inter-dialysis weight gain is assessed during each hemodialysis (HD) session and removed by ultrafiltration over the session to achieve adequate fluid removal. However, for children, weight gain does not always mean volume overload because children grow along with weight gain.
The dry weight of patients on dialysis is largely determined empirically by trial and error. Fluid status can be precisely measured by using the tracer dilution technique, but this gold standard is time consuming and expensive, and therefore not readily available for clinicians in routine clinical practice (2). Bioelectrical impedance methods, on the other hand, are easy to use, non-invasive, and rapid. These methods estimate body composition by measuring resistance and reactance of electrical current flow through the body (3). Owing to their convenience, repeated measurements are possible and excellent interobserver reproducibility has been reported (456). Therefore, bioelectrical impedance methods, bioimpedance analysis (BIA) or bioimpedance spectroscopy (BIS), are suited to routine use in the clinic or at the bedside, although they are less accurate in some pathologic conditions.
The literature on the application of bioelectrical impedance in dialysis patients indicates that this method can be useful for determining the accurate volume status (78910); however, only a few published studies are available in the pediatric population in this regard (111213). In the case of children, most published data using bioelectrical impedance methods are limited to evaluations of nutritional status rather than fluid status (1415). The present study thus aimed to determine whether bioelectrical impedance devices can correctly assess fluid status, and which device, BIA or BIS, is more valid for children receiving maintenance HD.
MATERIALS AND METHODS
Study subjects
From September 2014 to December 2015, children receiving maintenance HD at a single dialysis center in Korea were recruited, after obtaining written informed consent from their legal guardians. The participants were clinically stable and had been on maintenance HD for more than 1 month. The following patients were excluded from the study: 1) those aged ≤ 4 years and ≥ 20 years; 2) those with metallic implants; 3) those with severe cutaneous alterations such as wounds, eschars, or crusting skin; and 4) those with inability to maintain neutral position.
The patients were evaluated during a routine visit for HD and physically examined for signs indicating volume overload such as peripheral edema. Blood pressure was recorded before HD by using a single calibrated device. Height and weight (pre- and post-HD) were measured by using a single calibrated device. When the pre-HD body weight of the patient increased compare to the post-HD body weight of previous HD, the difference of body weight was regarded as fluid accumulation of the patient. The symptoms of volume overload (edema and hypertension) were assessed by a trained clinician. The number of antihypertensive medications prescribed at the time of the measurement was recorded for analysis.
Assessment of body composition and hydration state
Two commercially available bioelectrical impedance devices were used to estimate body fluid volume based on bioimpedance, namely Inbody S10 (BioSpace, Seoul, Korea) and Body Composition Monitor (BCM; Fresenius Medical Care, St. Wendel, Germany). InBody S10 is based on multi-frequency BIA (MF-BIA) that analyzes body composition in 5 segments of the body at 6 different frequencies (1, 5, 50, 250, 500, and 1,000 kHz) (16). The other device BCM is based on BIS and measures body composition in the entire body at 50 different frequencies ranging from 5 kHz to 1 MHz (9). As the reproducibility of the method is quite high (1617), measurement was not repeated.
After measuring pre-HD body weight, pre-HD body fluid status was measured in the supine position using the bioelectrical impedance devices following the instructions of the manufacturers of the devices, immediately before HD. For post-HD fluid status measurement, the measurement was repeated 30 minutes after completion of the session of HD, followed by post-HD body weight measurement. The patients were not allowed to drink or eat during or after dialysis before measurement; all measurements were performed by a single trained examiner.
The extracellular water (ECW), intracellular water, and total body water volume were assessed using each device, and overhydration (OH) was subsequently calculated by using equations in the devices (1718). To assess the accuracy of the devices measuring fluid status of the pediatric patients, the difference in total body water measured (measured fluid [MF]) by using each device before and after a HD session was compared to the clinically assessed body fluid status change, defined as the difference of body weight before and after the HD session. In order to evaluate the usefulness of each device to assess the fluid status of the pediatric patients, device-reported OH was compared to the clinically assessed fluid accumulation at the time of pre-HD measurement. Device-assessed fluid status of each patient was designated as adequate, fluid overload (FO), and severe FO as follows; The proportional OH relative to ECW (OH/ECW, %) was referred as the hydration status (ΔHS), and ΔHS greater than 7% was defined as FO according to previous publications, considering the 90th percentile of ΔHS in the normal reference population is 7% (119). As an ΔHS greater than 15% has been reported to be related to mortality (1), ΔHS greater than 15% was defined as severe FO. Designation of the device-assessed fluid status was compared to the clinical manifestations of the patients.
Statistical analysis
Descriptive statistics are shown as mean ± standard deviation. Pearson's correlation analysis was used to assess the relationships between weight change and volume status change before and after HD. Regression analysis was performed to demonstrate the correlation between weight and volume status changes with HD. The intercept (α), slope (β) coefficient, and correlation coefficient (r2) of regression were calculated. The Bland-Altman method based on between-method differences was used to determine the agreement between the values measured by different methods (20). All statistical significance was set at P < 0.05.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Seoul National University College of Medicine (IRB No. 1304-110-484) and conducted in accordance with the Declaration of Helsinki. Informed consent was submitted by all subjects when they were enrolled.
RESULTS
Participants' baseline characteristics
The characteristics of the patients included in the study are shown in Table 1. Twenty-three values were collected from 12 patients who were undergoing maintenance HD. The patients' mean age was 11.9 ± 5.0 years (range, 5–19 years). When a patient clinically seemed to have change in his/her body fluid status, the fluid status of the patient was measured again and analyzed as separate measurements. Their mean body weight was 32.9 ± 15.9 kg (range, 15–71 kg), and mean height was 132.4 ± 21.5 cm (range, 104–174 cm). The mean duration of HD was 12.5 months (range, 1–38 months). The underlying diseases included chronic glomerulonephritis (3 patients), renal hypoplasia (2 patients), renal tubular acidosis (1 patient), glycogen storage disease type I (1 patient), neurogenic bladder (1 patient), and unknown (4 patients). Volume overload symptoms of pitting edema and/or hypertension were observed in 12 measurements (52.2%).
Table 1
Clinical characteristics and laboratory variables of the patients (recordings = 23)
Validation of Inbody S10 and BCM
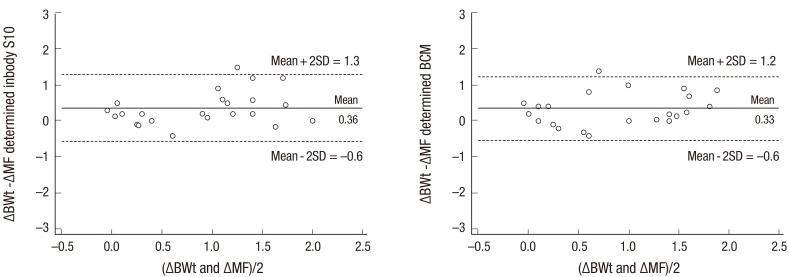
If the device measures the fluid status of a pediatric patient, the difference in MF state before and after HD (ΔMF) would be the same as the difference in clinically assessed body fluid status change, in other words the weight changes (Δbody weight, ΔBWt) over HD. Pearson's correlation analysis was performed to assess the correlation between the ΔBWt and ΔMF measured with each device, showing strong correlation with Pearson's coefficient (r) = 0.772 with Inbody S10 (P < 0.001) and 0.799 with BCM (P < 0.001; Fig. 1). Regression analysis revealed a correlation coefficient and r2 of 0.610 and 0.596 for Inbody S10 and 0.690 and 0.639 for BCM, respectively (Fig. 1). Bland-Altman analysis to assess the agreement between different methods showed, the mean difference between ΔBWt and ΔMF were 0.36 L (−0.6 to 1.3 L) in the Inbody S10 and 0.33 L (−0.6 to 1.2 L) in BCM, with wider limits of agreement by Inbody S10 (Fig. 2).
Fig. 1
Correlation between the differences in MF state before and after HD and weight changes over HD.
MF = measured fluid, HD = hemodialysis, ΔBWt = body-weight changes, ΔMF = difference in measured fluid state before and after HD.
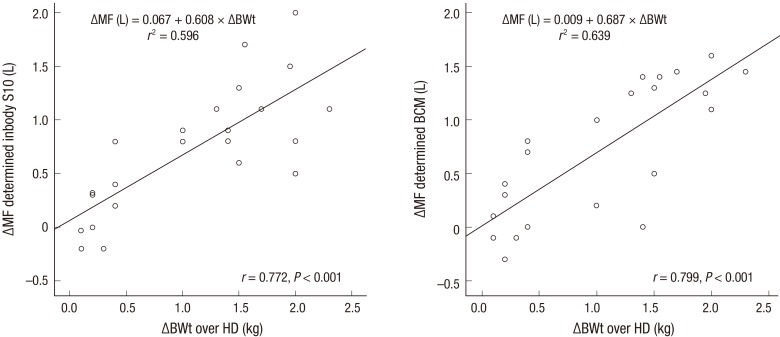
Fig. 2
Agreement between the differences in MF state before and after HD and weight changes over HD. The solid line is the mean differences, and the dashed horizontal lines represent the two standard deviations of the differences.
MF = measured fluid, HD = hemodialysis, ΔBWt = body-weight changes, ΔMF = difference in measured fluid state before and after HD, TBW = total body water, SD = standard deviation.
In clinical setting, a device to measure body fluid status is used to estimate OH before a session of HD, therefore clinicians use the value to decide how much fluid to remove from the patient. If dry weight of a patient is known, the accuracy of the device can be easily evaluated; however, the tracer dilution technique measuring the fluid status precisely is not available. Therefore, we made an assumption that post-HD body weights of a patient were his/her dry weight, and gain of weight after previous HD was regarded fluid accumulation. Ideally, device-reported OH would be the same as clinically assessed fluid accumulation; therefore, OH reported by each device was compared to clinically-assessed fluid accumulation. As seen in Fig. 3, clinically-assessed fluid accumulation was not correlated with OH assessed by either device (r = 0.368; P = 0.084 with Inbody S10 vs. r = 0.218; P = 0.317 with BCM). However, while BCM assessed OH up to 4.8 L, which was often observed in our subjects, OH assessed by Inbody S10 was less than 1.5 L (Table 2, Fig. 3).
Fig. 3
Comparison of difference between clinically calculated OH and bioimpedance measured OH.
OH = overhydration.
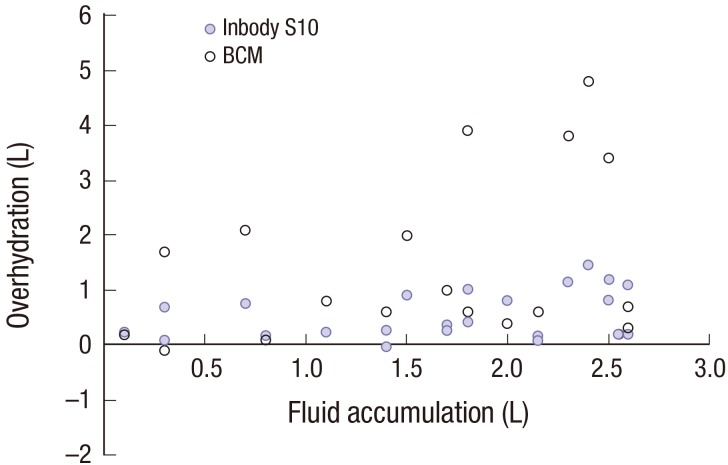
Table 2
Comparison of results for BIA before and after HD (recordings = 23)
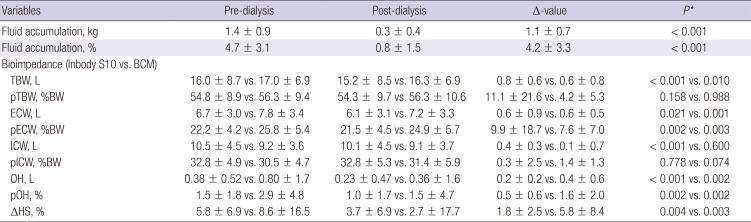
Reference range of the TBW, ECW, and ICW is 60%, 20%, and 40%.
BIA = bioimpedance analysis, HD = hemodialysis, TBW = total body water, pTBW = percent TBW (TBW/BW × 100), ECW = extracellular water, pECW = percent ECW (ECW/BW × 100), ICW = intracellular water, pICW = percent ICW, OH = overhydration, pOH = percent OH, ΔHS = proportional OH relative to ECW (OH/ECW).
*Paired t-test of the mean difference of pre- and post-dialysis bioimpedance data.
Clinical correlation
Some of the subjects showed clinical symptoms of OH; pitting edema and hypertension were identified on 5 (22%) and 11 (48%) occasions among a total of 23 recordings, respectively (Table 3); ΔHS was not significantly higher in the patients with edema (mean 8.1% by Inbody S10 and 13.5% by BCM) than in those without edema (mean 4.5% by Inbody S10 and 7.4% by BCM; P = 0.294 for Inbody S10 and 0.317 for BCM). Hypertension as indicator of clinical OH was less straightforward because some normotensive patients were taking antihypertensive medications, therefore in fact their blood pressure would be higher than normal if they were not taking the medication, and some of them might have clinical OH. However, no significant difference in the numbers of antihypertensive agents was found between patients with and without hypertension. ΔHS was not significantly different between the patients with and those without hypertension (Inbody S10: 5.2% vs. 5.4%, P = 0.939; BCM: 9.7% vs. 7.8%, P = 0.796) (Fig. 4).
Table 3
Relationship between volume overload and clinical parameters

| Clinical symptoms | BCM | Inbody S10 | ||||
|---|---|---|---|---|---|---|
| severe FO (−)(n = 15) | severe FO (+)(n = 8) | P* | severe FO (−) (n = 21) | severe FO (+) (n = 2) | P* | |
| Pitting edema | 4 | 1 | 0.621 | 3 | 2 | 0.036 |
| Hypertension | 8 | 3 | 0.667 | 10 | 1 | 0.949 |
Fig. 4
Hydration status according to symptoms. Scatter graph shows the degree of ΔHS according to clinical symptoms in enrolled patients. FO (ΔHS greater than 7%) denoted by the yellow color box and severe FO (ΔHS greater than 15%) denoted by green box.
FO = fluid overload, ΔHS = hydration status, HT = hypertension, E = edema.
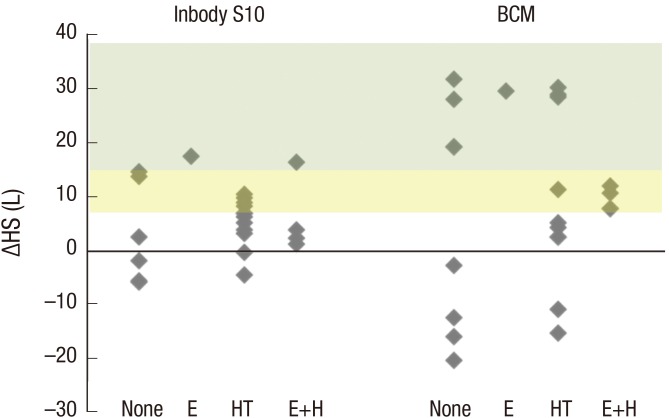
On the other hand, the mean ΔHS was 5.3% with Inbody S10 and 8.7% with BCM; FO was found in 34.8% by Inbody S10 and 56.5% by BCM and severe FO was found in 8.7% by Inbody S10 and 34.8% by BCM, before HD. Two patients (40%) and one patient (20%) with edema (n = 5) were identified as having severe FO as determined by using Inbody S10 and BCM, respectively. One patient (9%) and three patients (27%) with hypertension (n = 11) had severe FO as determined by using Inbody S10 and BCM, respectively (Fig. 4).
DISCUSSION
Fluid status is a critical issue to consider in patients receiving dialysis, but reliable end points for euvolemia are difficult to establish in routine clinical practice. Hypervolemia state is considered as the most important predisposing factor of hypertension and long-term complications in patients receiving dialysis (121). Traditionally, the volume status in dialysis patients is determined via clinical assessments such as inter-dialytic weight gain, presence of hypotension or hypertension, and edema. However, interpretation of clinical indicators is subjective and these indicators lack precision, while the degree of OH needs to be measured precisely to manage the dialysis patients adequately. In this regard, bioimpedance has found widespread application in dialysis patients since it was first applied in 1963 (37891122). Two methods of bioimpedance, namely BIA (Inbody S10) and BIS (BCM), quantify the passive electrical properties of a biological tissue, which resists or impedes an applied electrical current (323). Inbody S10 and BCM differ in how they measure bioimpedance. Inbody S10 uses empirical linear regression models but includes impedances at multiple frequencies. In contrast to Inbody S10, BCM uses mathematical modeling and mixture equations, and then develop empirically derived prediction equations rather than go to mixture modeling (23). Both Inbody S10 and BCM are considered useful to predict body composition, and they reflect both nutrition and hydration (141524), although their findings are not valid under certain pathological conditions (25). In patients receiving dialysis, several studies have analyzed the use of bioimpedance methods (78919). Davies and Davenport (8) reported a role of bioimpedance in aiding clinical decision-making of volume assessments in dialysis patients. Kim et al. (7) reported that RFO measured with bioimpedance in HD was related to the overall survival. However, limited data are available for children (111213), and the results from research in adults may not be extrapolated to children. Nonetheless, Zaloszyc et al. (13) asserted that dialysis children should benefit from the measurement of hydration status by bioimpedance, supporting the clinical assessment of OH.
For children, assessment of volume status is more complex because their body composition and body size are expected to change considerably along their growth. To assess the clinical validity of bioimpedance measurement devices, we used body weight change during HD. In patients without urine output, accumulation of body fluid after ingestion results in direct increase in body weight. During ultrafiltration, for every liter of water removed, the weight of a patient decreases by 1 kg. Thus, changes in body weight and total body water volume with HD are compared to evaluate the accuracy of bioimpedance methods. In our study, ΔMF measured with each device showed a significant correlation with ΔBWt. This result suggests that both Inbody S10 and BCM might be valid to determine the fluid status in pediatric patients receiving HD.
Regarding assessment of the fluid status of the patients, FO assessed by each device was compared with clinically recognized OH. In the children with symptoms of hypertension or edema, FO was indicated in 42% by Inbody S10 and 67% by BCM method, implying that clinically recognized volume overload was not always recognized as OH by these bioimpedence methods. On the other hand, only about 60% of children with FO by bioimpedance methods showed hypertension and/or edema, indicating poor correlation between clinically recognized volume overload and device-recognized FO. Since some patients remain asymptomatic despite having volume overload (26) and volume overload is difficult to recognize by clinical assessments, even in the hands of experienced physicians (27), practical tools to objectively assess volume overload in children receiving dialysis are needed, where a bioimpedance device can be a good choice as shown in recent several studies (781928). Then, which device is more relevant in children? In our study, FO was more frequently detected by BCM (56.5%) than Inbody S10 (34.8%), while it was expected that the proportion of FO be higher with Inbody since BIS method (of Inbody) was reported to overestimate TBW in adults (29). Since true fluid status of our subjects was not known and the number of subjects were too small, we are not able to compare the usefulness of these two devices; however, in some patients with larger weight gain Inbody S10-assessed OH was much smaller than BCM-assessed OH, suggesting that Inbody S10 was less reliable than BCM in estimating fluid accumulation amount.
Our study has some limitations. First, given the small sample size, our results should be interpreted with caution. Second, device validity was not confirmed by using the tracer dilution technique. However, HD is an excellent model of fluid removal, and comparison of body weight and total body water changes with HD seems a relatively accurate method for estimating device accuracy. To increase the accuracy of impedance methods, further studies are needed based on a tracer dilution technique.
In conclusion, bioimpedance is suitable for determining volume status in pediatric patients receiving HD. BCM showed better accuracy and agreement with fluid status than Inbody S10 in children receiving HD. To our knowledge, this is the first report on the application of bioimpedance in children receiving dialysis in Korea.
 XML Download
XML Download