

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) is a reliable and accurate tool for the diagnosis and treatment of biliary and pancreatic diseases. However, acute pancreatitis is the most common adverse event of ERCP, occurring overall in 5%–7% of patients (12). As post-ERCP pancreatitis (PEP) carries a potential risk of morbidity and occasionally of mortality, early PEP prediction would allow the safe discharge or prompt admission of patients who undergo outpatient ERCP procedures (345). For inpatients, it would help deal with PEP in a timely manner and prevent disease progression.
Four-hour post-ERCP amylase level is the most widely investigated potential predictor of PEP (5678) because it can be compared with 24-hour amylase level, which is the key determinant of PEP diagnosis and a practical parameter for early prediction and treatment of PEP. However, the data measured at 4 hours after ERCP carry a potential risk of PEP over-prediction because serum amylase levels can be asymptomatically increased between 90 minutes and 4 hours after ERCP, subsequently returning to normal values within 48 hours; however, they remain remarkably elevated when PEP occurs (910). Moreover, the ideal cut-off values for prediction of PEP differ among different studies. Therefore, the aim of this study was to verify the usefulness of 4-hour post-ERCP serum amylase and lipase levels for early PEP prediction and find predictive cut-off values of 4-hour post-ERCP serum amylase and lipase levels for PEP.
MATERIALS AND METHODS
Patients and procedures
Between January 2013 and August 2014, 516 consecutive patients with native papilla and without a history of pancreatitis or surgically altered enteric anatomy underwent ERCP. We retrospectively reviewed these cases from a prospectively collected ERCP database system. Both serum amylase and lipase were measured before and at 4 and 24 hours after ERCP. All ERCP procedures were performed using standard techniques and a side-viewing duodenoscope (JF-260V/TJF-260V; Olympus Corp., Tokyo, Japan) by 3 operators (JHK, BMY, JCH) with an experience of more than 300 ERCP procedures per year.
Outcome measurements
Patients' demographics, indications for ERCP, details of ERCP procedure, 4-hour post-ERCP amylase/lipase levels, and PEP occurrence on the next morning were analyzed. PEP was defined as abdominal pain persisting for at least 24 hours and associated with an amylase level of at least 3 times the upper limit of reference (ULR). Clinical severity of PEP was assessed according to the consensus criteria (11). The cut-off values of 4-hour post-ERCP amylase and lipase level with best sensitivity among the cut-off values with sensitivity higher than 90% were selected as the cut-off values for safe same day discharge to minimize the incidence of false negative results. The cut-off values with best specificity among cut-off values with specificity higher than 90% were selected as the cut-off values for preventive therapy of PEP to minimize the incidence of false positive results.
Statistical analysis
Statistical analyses were performed using SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA). Quantitative data were compared using the student's t-test or Mann-Whitney test, and the significance of difference for categorical data was determined using the χ2 test and Fisher's exact test. A receiver-operator characteristics curve was computed to test the strength of a given diagnostic test. Binary logistic regression analyses were applied to identify significant predictors of PEP.
RESULTS
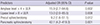
A total of 516 patients were enrolled in this study. Of them, 374 (72.5%) underwent therapeutic ERCP and 142 (27.5%) underwent diagnostic ERCP. The most common final diagnosis was bile duct stone (56.4%) (Table 1). PEP occurred in 16 (3.1%) patients and clinical severity was mild in 4 (25%) patients, moderate in 9 (56.3%) patients, and severe in 3 (18.8%) patients. All patients recovered completely with in-hospital supportive care, except for 1 patient with severe PEP who died of septic shock. A significant difference was found between patients with and without PEP with regard to the proportion of the nondilated extrahepatic bile duct (P = 0.007), precut sphincterotomy (P = 0.016), pancreatogram performance (P = 0.003), pancreatic sphincterotomy (P = 0.003), elevated 4-hour post-ERCP serum amylase (P = 0.001), and lipase levels (P = 0.003) in the univariate analyses (Table 2).
Table 1
Patient characteristics
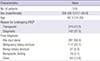
Table 2
Univariate comparison of patients with and without PEP
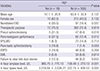
Values are presented as number (%). Continuous variables are expressed as the mean ± standard deviation.
ERCP = endoscopic retrograde cholangiopancreatography, PEP = post-ERCP pancreatitis, EHD = extrahepatic bile duct, EP(L)BD = endoscopic papillary (large) balloon dilation, ERPD = endoscopic retrograde pancreatic drainage, EML = endoscopic mechanical lithotripsy.
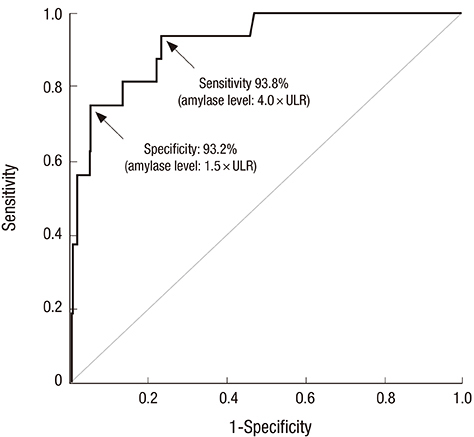
The receiver-operator characteristic curve for 4-hour post-ERCP serum amylase showed that the area under the curve was 0.919, demonstrating a good test performance as a predictor of PEP (P < 0.001) (Fig. 1). The cut-off levels of 1.5 times the ULR was found useful for exclusion of PEP with a sensitivity of 93.8%, and 4 times the ULR was found useful to guide preventive therapy of PEP with a best specificity of 93.2% (Table 3).
Fig. 1
Receiver-operator characteristics curve for 4-hour post-ERCP amylase levels as a predictor of PEP. Area under the curve = 0.919 (P < 0.001). The cut-off levels of 1.5 times the ULR is useful for exclusion of PEP with a sensitivity of 93.8%, and 4 times the ULR is useful to guide preventive therapy of PEP with a best specificity of 93.2%.
ERCP = endoscopic retrograde cholangiopancreatography, PEP = post-ERCP pancreatitis, ULR = upper limit of reference.
Table 3
Cut-off 4-hour post-ERCP amylase levels for predicting pancreatitis

The receiver-operator characteristic curve for 4-hour post-ERCP serum lipase level showed an area under the curve of 0.933, also demonstrating good test performance as a predictor of PEP (P < 0.001) (Fig. 2). The best sensitivity was noted for the lipase level of 2 times the ULR, and the best specificity was noted for 8 times the ULR (Table 4). After adjusting for potential confounders, logistic regression analysis showed that 4-hour post-ERCP amylase level above 4 times, 4-hour post-ERCP lipase above 8 times, precut sphincterotomy, and pancreatic sphincterotomy were significant predictors for PEP (Table 5).
Fig. 2
Receiver-operator characteristics curve for 4-hour post-ERCP lipase levels as a predictor of PEP. Area under the curve = 0.933 (P < 0.001). The cut-off levels of 2 times the ULR is useful for exclusion of PEP with a sensitivity of 93.8%, and 4 times the ULR is useful to guide preventive therapy of PEP with a best specificity of 91.4%.
ERCP = endoscopic retrograde cholangiopancreatography, PEP = post-ERCP pancreatitis, ULR = upper limit of reference.
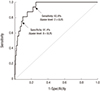
Table 4
Cut-off 4-hour post-ERCP lipase levels for predicting PEP

Table 5
Logistic regression analyses of significant predictors for PEP, adjusted for patient and procedure related factors
All factors were adjusted for patient age, sex, bile duct dilation, reason for undergoing ERCP, final diagnosis, extrahepatic bile duct dilation, precut sphincterotomy, pancreatogram performance, endoscopic papillary balloon dilation, pancreatic sphincterotomy, endoscopic retrograde pancreatic duct drainage, mechanical lithotripsy, failure to clear bile duct, the cut-off values of post-ERCP amylase and lipase with best specificity which guide the initiation of resuscitation.
ERCP = endoscopic retrograde cholangiopancreatography, PEP = post-ERCP pancreatitis, OR = odds ratio, CI = confidence interval, ULR = upper limit of reference.
DISCUSSION
Nowadays, outpatient ERCP procedures are widely performed because they can reduce medical costs and conserve resources, while their safety is comparable with that of ERCP procedures performed on an inpatient basis (3). However, a reliable prediction model for PEP should be established before the widespread use of outpatient ERCP. Based on this model, patients who underwent outpatient ERCP procedures would be classified into 2 groups: the “discharge group” with asymptomatic patients or patients with mild, self-limiting symptoms, and the “admission group” with patients at potential risk for developing PEP that would need supportive therapy (34). In patients admitted after ERCP, early prediction of PEP would enable early aggressive fluid resuscitation and careful monitoring, which could limit the disease progression and contribute to a better prognosis.
Post-ERCP serum amylase level has been widely investigated as an early predictor for PEP in many studies (4567810121314). However, each study used different blood sampling times for measuring serum amylase levels and reported different predictive cut-off values for best PEP prediction.
Defining the optimal cut-off value of post-ERCP amylase level at a specific time that would allow a safe same-day discharge after ERCP is a complex task. The most important qualifying factor for setting a cut-off value is to exclude or nearly minimize the number of patients with false negative results, in whom PEP is finally diagnosed at 24 hours after ERCP, but early post-ERCP amylase level was below the cut-off value. In ERCP procedures performed on an outpatient basis, these patients with false negative results would have been discharged on the same day of ERCP based on the results of early post-ERCP amylase level. Therefore, a cut-off value minimizing false negative results can guarantee a safe same-day discharge after outpatient ERCP. Among the diagnostic discrimination values, both the sensitivity and the negative predictive value include cases with false negative results. However, the sensitivity is a more likely considerable factor of the 2 because a true negative value is disproportionately much higher in cases with false negative results at any cut-off values of post-ERCP amylase; therefore, a negative predictive value has little discriminating role at different cut-off levels.
To set an optimal cut-off value for deciding urgent admission in the outpatient setting is somewhat different from deciding a cut-off value for discharge. The crucial factor is to minimize the number of cases with false positive results, who would finally be proved to have no PEP, but post-ERCP amylase level had exceeded the cut-off value. If ERCP was performed on an outpatient basis, these patients would be unnecessarily hospitalized and additional cost would be incurred without clinical benefit. Although both specificity and positive predictive value reflect false positive cases, specificity is a more reliable discrimination value because positive predictive value is usually low at any cut-off level due to the imbalance between the true positive and false positive cases, as shown in many previous studies and in our study. As a result, good specificity is the key factor to determine the same-day admission and the initiation of preventive treatment following an ERCP performed on the outpatient basis.
However, if we choose the ideal cut-off values based only on the numerically high sensitivity and specificity, the gap between the cut-off value with high sensitivity and value with high specificity become large, because lower cut-off value provides higher sensitivity, while higher cut-off value provides higher specificity. Consequently, the number of patients in the middle zone with post-ERCP amylase levels between the two cut-off values will be increased, and preventive treatment initiation in those patients will be complicated and based on various procedure-related and patient-related risk factors, not on the post-ERCP amylase and lipase levels. Therefore, in order to keep the discriminating roles and reduce the size of the middle zone, we selected the highest cut-off value among the cut-off values with sensitivity higher than 90% as a criterion for safe discharge, and the lowest cut-off value among cut-off values with specificity higher than 90% as a criterion for initiation of prompt resuscitation.
Two factors should be considered in deciding when to obtain blood samples for testing serum amylase levels after ERCP. The first factor is the practical usefulness in the outpatient setting, and the second is a reliable correlation between the early post-ERCP amylase levels at a specific time and those measured at 24 hours after ERCP. Therefore, the amylase levels measured not only at 8 hours, but also at 24 hours have a time limitation with regard to obtaining results and making a decision of discharge on the same day of ERCP.
For this reason, many studies were performed to investigate the usefulness of 4-hour post-ERCP amylase levels than amylase levels measured at other times for early prediction of PEP. A prospective outcome study performed by Thomas and Sengupta (7) on 263 consecutive patients suggested a practical algorithm based on the 4-hour post-ERCP amylase levels and suggested that 1.5 times the ULR is useful for exclusion of PEP with a best sensitivity of 100% and 3 times the ULR is useful to guide preventive therapy with a best specificity of 95.3%. A larger-scaled retrospective study on 886 ERCP procedures by Sutton et al. (8) also reported the usefulness of the 4-hour post-ERCP amylase level as an early predictor for PEP. They recommended that patients who had not undergone a pancreatogram should be admitted if the 4-hour post-ERCP amylase level is greater than 5 times the ULR, the sensitivity and specificity of which were 100.0% and 96.3%, respectively, for predicting moderate to severe PEP. In patients who had not undergone a pancreatogram, 2.5 times the ULR was the best cut-off value for predicting a moderate to severe PEP with a sensitivity of 80.0% and a specificity of 80.4%.
In our study, the cut-off level 1.5 times the ULR had the great sensitivity of 93.8% and 2.5 times the ULR has great specificity of 93.2% in the amylase level analysis. Therefore, judging from our results, patients with 4-hour post-ERCP amylase levels less than 1.5 times the ULR could be discharged on the same day, while patients with 4-hour post-ERCP amylase levels above 4 times might be considered for urgent admission for supportive therapy. In patients who have equivocal amylase levels between 1.5 and 4 times ULR, the next clinical strategy should be decided based on the factors known to be definite or potential risk factors of PEP. Among these patients, patients with 4-hour post-ERCP lipase level above 8 times the ULR or those who received precut sphincterotomy or pancreatic sphincterotomy may be considered for admission for supportive treatment based on our results of multivariate analyses.
However, the amylase level is known to increase up to 4 hours after ERCP even in the absence of PEP (910); therefore, 4-hour post-ERCP amylase level may not correctly reflect the 24-hour level. In the large scaled prospective study, Testoni et al. (6) compared the 2-, 4-, and 8-hour post-ERCP amylase levels with those at 24-hour to identify the ideal timing for blood sampling after ERCP. They showed a significantly higher sensitivity of 100% at 8-hour measurement than at others, but recommended the 4-hour assessment from a practical point of view for outpatients. The largest retrospective study performed by Ito et al. (10) concerning the relationship between 3-, 6-, and 24-hour serum amylase levels after ERCP reported a meaningful outcome that a decrease in amylase levels at 6 hours after ERCP suggests a low probability for PEP, even though hyperamylasemia was noted at 3-hour measurement. Therefore, a future large scaled prospective study comparing 4-hour and 6-hour post-ERCP amylase levels as early predictors for PEP is needed, because 6-hour measurement may be the Maginot Line of time in outpatient settings.
Many studies have demonstrated that serum lipase level is the most accurate diagnostic marker for acute pancreatitis (1516), and serum lipase level increased faster than the levels of other measured enzymes and that the average peak in lipase level was the highest in PEP (17). However, the usefulness of post-ERCP lipase level as an early predictor for PEP has not been as widely studied as amylase level because it is not included in the diagnostic criteria of PEP. Our data showed that 4-hour post-ERCP serum lipase level is also a reliable predictor of the risk of PEP based on the area under the receiver-operator characteristic curve. However, in our study, the clinical utility of lipase levels for the prediction of PEP was lower than that of amylase levels because the gap between the cut-off values of best sensitivity (2 times) and specificity (8 times) was very large. Therefore, serum lipase level can be used as an adjuvant factor in patients with an equivocal range of amylase level. An additional study is needed to clarify the usefulness of the 4-hour post-ERCP hyperlipasemia as a predictor for PEP.
There are some limitations of this study. ERCP-related detailed confounders associated with PEP, such as cannulation time, the number of papillary contacts of cannulas, or the number of inadvertent pancreatic cannulations were not systematically analyzed owing to the study's retrospective nature. Therefore, it is difficult to set a well-designed practical prediction model for PEP in patients with equivocal range of serum amylase level between the cut-offs of best sensitivity and specificity.
In conclusion, the 4-hour post-ERCP amylase and lipase levels are useful early predictors for PEP and would ensure safe discharge on the same day of ERCP or prompt fluid resuscitation and close monitoring after ERCP.
 XML Download
XML Download