

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The Korean Triage and Acuity Scale (KTAS) was developed in 2012 based on the Canadian Triage and Acuity Scale (CTAS), with modifications to adapt it to the Korean medical environment (12). After the completion of a pilot study, KTAS was introduced and mandated in all emergency departments (EDs) throughout the country on January 1, 2016. KTAS is divided into adult and pediatric KTAS (PedKTAS) at the age of 15 years (2).
Initial vital signs are recommended in assessing the level of PedKTAS (2); however, limitations have been noted when using the initial vital signs to determine the triage levels in children. Because children who are placed in unfamiliar environments become anxious and irritable, this effect may cause a shift of vital signs beyond the normal range (345). Therefore, although a child may have a non-emergent condition, the level of severity may seem to be higher when his or her initial vital signs are applied directly to determine the triage levels.
This incorrect ‘over-triage’ can lead to overcrowding of the pediatric ED with an increased length of stay, unnecessary utilization of medical resources, increased medical costs, and potential threats to patients' safety (467). Therefore, a nationwide controversy has emerged regarding whether the vital signs of children should be directly applied to PedKTAS or whether a modified interpretation of vital signs should be used. The pediatric CTAS guideline suggests that even if the patient's vital signs are measured to be abnormal, such as tachycardia in upset child, triaging lower than the measured abnormal vital signs can be done with careful clinical decision (5). Furthermore, a retrospective cohort study using the Japanese Triage and Acuity Scale based on CTAS also demonstrated that patients who were down-triaged (assignment of lower triage level) by clinical decision based on the patient's general condition had better predictability for the disposition from the pediatric ED (4).
The aim of this study was to determine the effectiveness of the triage method based on the clinical decision dependent on the patient's general condition. We hypothesize that clinical decision-based triage rather than the strict application of initial vital signs to the PedKTAS will exhibit a more accurate correlation with the disposition of the patient from the pediatric ED.
MATERIALS AND METHODS
Study setting and design
This was a retrospective cohort study of patients who visited the pediatric ED of a tertiary hospital with 315 beds. All patients under 15 years of age who were triaged using PedKTAS during the study period from January 1 to December 31, 2016, were included.
Upon arrival at the pediatric ED, patients' vital signs were measured (pulse rate was measured by pulse oximeter and respiratory rate was measured manually); and patients were triaged using PedKTAS by experienced triage providers. The triage team providers consisted of five nurses with at least two years of working experience in the pediatric ED. The triage was processed through a computer program that was networked with the hospital's medical record system. The patient's PedKTAS level, processing code, vital signs, gender, age, and disposition from the pediatric ED were transmitted to the National Emergency Department Information System. In this study, after the data were transmitted to the system, all information was collected and de-identified prior to analysis.
PedKTAS level simulation process
PedKTAS is a 5-level triage system (level 1, resuscitation; level 2, emergent; level 3, urgent; level 4, less urgent; and level 5, non-urgent) that classifies the patients into 17 categories based on their symptoms. Depending on the presence of modifiers (e.g., consciousness, vital signs, degree of respiratory difficulty, and bleeding disorders) that can be applied in the subcategories, the final PedKTAS level is determined (2). Therefore, patients within the same symptom category may be sorted into different PedKTAS levels, depending on the presence of modifiers, such as abnormal vital signs.
When using the PedKTAS, the patient's symptom categories and modifiers are recorded in the processing code. Even though the patient's vital signs measured at the pediatric ED (study site) were abnormal, if the patient's medical condition appeared to be mild and the measured abnormal vital signs were determined to have been measured in an upset child, the triage nurse down-triaged the patient based on previous studies suggesting evidence for a down-triage (59). In these cases, we re-calculated the patient's PedKTAS levels by direct applying their abnormal vital signs to the classification criteria of PedKTAS for the study. The final PedKTAS levels of those patients whose initial abnormal vital signs were reconsidered by the triage nurse were defined as the ‘real practice (RP)-PedKTAS levels,’ and the calculated PedKTAS levels of these patients were defined as the ‘simulation (S)-PedKTAS levels.’
Primary and secondary outcomes
The primary outcome of this study was to observe whether the hospitalization rate according to the PedKTAS level was consistent with the hospitalization rate suggested by pediatric CTAS (9). Hospitalization included admission to the general ward, intensive care unit (ICU), operation room, and transfer to another hospital. The secondary outcomes were whether the PedKTAS level-specific hospitalization rate and ICU admission rate correlated with the previously results of CTAS multicenter study (10).
Statistical analysis
The Kolmogorov-Smirnov normality test was used to assess for normality. Data with a normal distribution were described using mean ± standard deviation, and non-parametric data were described using median (interquartile range). Pearson correlation analysis was used to compare results according to the level of PedKTAS and pediatric CTAS. P values < 0.05 were considered statistically significant. All statistics were analyzed using R version 3.3.3 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Study population and triaged levels
During the study period, a total 24,670 patients visited the pediatric ED. Of these, 22,841 patients under 15 years of age were triaged using PedKTAS (Fig. 1). The median age of the patients was 3.15 years, and 12,840 (56.2%) were male (Table 1).
Fig. 1
A flow chart of the entire patient and subject distribution based on PedKTAS classification methods.
PedKTAS = Pediatric Korean Triage and Acuity Scale, RP = real practice, S = simulation.

Table 1
Baseline characteristics of the patients

The triage results when using RP-PedKTAS showed that the KTAS level with the most patients was level 3 (11,789 [51.6%]), followed by level 4 (6,957 [30.5%]), level 5 (1,990 [8.7%]), level 2 (1,967 [8.6%]), and level 1 (138 [0.6%]). In contrast, the triage results when using S-PedKTAS showed that the highest number of patients was in level 2 (13,939 [61.0%]), followed by level 1 (4,532 [19.8%]), level 3 (2,510 [11.0%]), level 4 (1,333 [5.8%]), and level 5 (527 [2.3%]). Compared with triage using RP-PedKTAS, significantly more patients were triaged into levels 1 and 2 by S-PedKTAS, with a total of 18,229 cases, which was 79.8% of all patients observed during the study period (Table 2).
Table 2
Comparison of the hospitalization rates between RP-PedKTAS level and S-PedKTAS level

Primary outcome
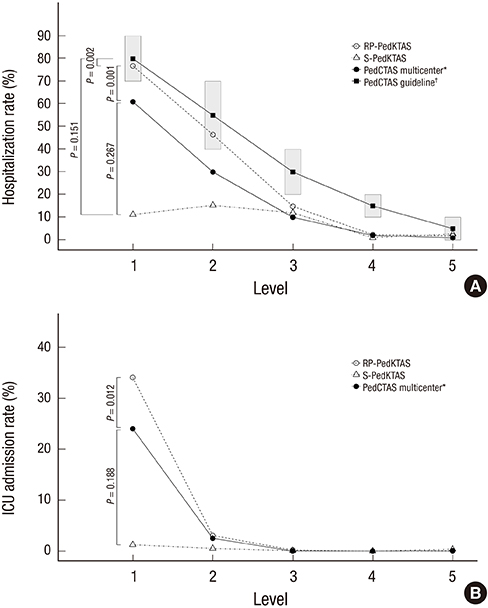
The hospitalization rates according to the PedKTAS levels in this study were compared with the expected hospitalization rates proposed by pediatric CTAS (level 1, 70%–90%; level 2, 40%–70%; level 3, 20%–40%; level 4, 10%–20%; and level 5, 0%–10%) (9). For the RP-PedKTAS levels, the hospitalization rates according to the level showed a significant correlation with the proposed rates (r = 0.987, P = 0.002), and the hospitalization rates at 1, 2, and 5 were within the suggested range. However, in the case of S-PedKTAS levels, there was no significant correlation (r = 0.742, P = 0.151), and only the hospitalization rate of level 5 was within the proposed range (Fig. 2A).
Fig. 2
Hospitalization rates and ICU admission rates according to triage levels. (A) Comparison of hospitalization rates according to triage levels. Gray boxes indicate the range of PedCTAS level-specific expected hospitalization rates, and black rectangles represent the median for each level. (B) ICU admission rate according to triage levels.
ICU = intensive care unit, PedCTAS = Pediatric Canadian Triage and Acuity Scale, PedKTAS = Pediatric Korean Triage and Acuity Scale, RP = real practice, S = simulation.

Secondary outcomes
The PedKTAS level-specific hospitalization rate and ICU admission rate of this study were compared with the results of previous study using pediatric CTAS (10). The hospitalization rates and the ICU admission rates according to RP-PedKTAS levels were both highly associated with the results of the multicenter study using pediatric CTAS (r = 0.994, P = 0.001 and r = 0.999, P = 0.012; respectively). In contrary, the S-PedKTAS levels did not show a significant correlation with both the hospitalization rates and the ICU admission rates (r = 0.618, P = 0.267 and r = 0.957, P = 0.188; respectively) (Fig. 2B).
DISCUSSION
The higher predictability of a triage tool for determining a patient's status is essential for the efficient distribution of medical resources and quality improvement (6711). This study is the first validation study on the predictability of the PedKTAS, and the results of this study can be helpful for revising the PedKTAS.
Compared with RP-PedKTAS, S-PedKTAS had an inferior predictability for ED outcomes, such as hospitalization rate and ICU admission rate. Therefore, for children visiting the ED, the strict application of their vital signs to the triage tool without any modifications would lead to an excessive utilization of resources and an inefficient distribution of medical resources. Moreover, when comparing the hospitalization rates with the expected hospitalization rates proposed by pediatric CTAS, RP-PedKTAS showed more compatible ranges with the proposed scheme than did S-PedKTAS.
Although the RP-PedKTAS level based on clinical decision better predicted the hospitalization rate, this practice should be considered a ‘bypass’ to improve the triage system rather than the ultimate solution. Because the excessive dependence on subjective decision may cause additional bias in triage, the CTAS system also recommends being careful when applying clinical judgment (58). To complement this limitation, repeated education for triage nurses should be provided, and methods for setting objective criteria for down-triage should be developed (4). As an option for other solutions, an ED version of ‘reference’ vital signs range can be developed and utilized rather than vital signs standards from healthy populations (31213).
The problem of the direct application of abnormal vital signs in children is not only a problem of KTAS but is also a common problem of CTAS-based triage systems. Therefore, several studies have been conducted to overcome this limitation, and these studies showed similar results as our study (49). However, Gravel et al.'s study (9) was restricted to patients with fever (3–36 months), whereas the present study was not limited to fever and showed an analysis according to all ages using PedKTAS.
This study has some limitations. First, the data of this study are derived from a single center. Considering that patient severity and facility characteristics, including the numbers of the beds available for hospitalization varies between hospitals, applying the conclusions obtained from the results of this single center study to other hospital is not warranted. Nevertheless, this study brings awareness to the pitfalls of the PedKTAS and can serve as baseline data for further multicenter or even nationwide studies. Second, although the triage was done by multiple triage nurses, interpersonal reliability has not been verified. However, the fact that all triage nurses have more than 2 years of working experience at the pediatric ED and that the volume of patients was substantial (more than 22,000 patients during the study period) can reduce the bias in relation to triage nurses. Finally, this study did not perform an in-depth analysis of the patients' underlying disease and/or general medical condition. Rather than analyzing the underlying disease of the patients, this study focused primarily on the issue arising from directly applying abnormal vital signs without any modifications. Thus, further comprehensive studies are needed to investigate the characteristics of the study subjects.
In conclusion, even if the patient has abnormal vital signs measured in an upset state, if the patient's medical condition is mild instead of directly applying their abnormal vital signs to the PedKTAS, relying on the clinical decision of an experienced triage provider to determine the severity level has higher predictability for disposition from the pediatric ED. However, there are issues concerning the subjective clinical parameters that are used to modify an objective severity classification system. Therefore, to overcome these shortcomings, multicenter and national studies are needed to obtain objective and unbiased data.
 XML Download
XML Download