

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
An outbreak of Middle East respiratory syndrome (MERS) occurred in May 2015 in Korea. MERS entered the country through a single infected traveler and was amplified by infections in hospitals and the movement of cases within and between hospitals (1). Ninety-seven percent (181/186) of all the cases were associated with healthcare facilities (2). Given that emergency departments (EDs) were suggested as the primary locations through which the virus was spread, changes in their utilization pattern (i.e., a decrease in ED visits) were observed.
As usual, natural disasters (e.g., hurricanes or earthquakes) or infectious disease outbreaks (e.g., the severe acute respiratory syndrome [SARS] outbreak) have the potential to cause ED volume changes (345). Several studies showed a surge in the volume during the spring 2009 H1N1 influenza pandemic (6789) or a decline in ED visits during the SARS outbreak in Asia (31011). However, there has been no study on ED utilization patterns when MERS was spreading through hospitals. The aim of this study was to analyze the changes in the visit patterns in adult and pediatric EDs in one tertiary referral hospital in Korea during a period of the spread of MERS.
MATERIALS AND METHODS
Study design and setting
In Korea, the MERS outbreak occurred from June 1 to July 31, 2015. We retrospectively analyzed the patterns of visits of adult and pediatric patients to the ED during this outbreak and compared the results to the same period in 2013 and 2014. We included all patients who visited the ED during this time period (Fig. 1). This study was conducted in one tertiary referral hospital where approximately 60,000 patients (40,000 adults and 20,000 children) visit the ED annually.

Selection of participants
A pediatric patient was defined as a patient who was younger than 18 years of age. We subdivided the pediatric patients into 3 groups: younger than 1 year of age (infants), 1 to 4 years of age (young children), and 5 to 17 years of age (school-aged children).
Measurements
The emergency severity index (ESI) was used as a triage tool in both the adult and the pediatric ED. The acuity level was classified as high (ESI level of 1, 2, or 3) or low (ESI level of 4 or 5) (12). The acuity level, cause of the visit (disease/trauma), ambulance use, admission rate, and length of stay at the ED (EDLOS) were compared between the study period and the other periods.
Data analysis
The data were analyzed using the SPSS 22.0 statistical package (SPSS Inc., Chicago, IL, USA). The values of continuous variables are expressed as the mean ± standard deviation (SD) or the median (and interquartile range), whereas the values of categorical variables are expressed as the frequency (and percentage). Fisher's exact test and the Pearson χ2 test were used for categorical variables. Student's t-test was used to compare the differences between two groups. If needed, the Mann-Whitney U-test was used. The significance of the differences in the repeated-measures data between groups such as the EDLOS was analyzed using a repeated-measures analysis of variance. A P value of < 0.05 was considered statistically significant.
RESULTS
The total number of patients who visited the ED during the MERS epidemic period (9,107 patients) decreased compared to the same period in 2013 (11,333 patients) and 2014 (11,652 patients). The number of adult patient visits decreased by 12.2% and 13.4% compared to the numbers from 2014 and 2013, respectively. The number of visits of pediatric patients decreased by 42.3% and 32.2% compared to of the numbers from 2013 and 2014, respectively (Supplementary Table 1).
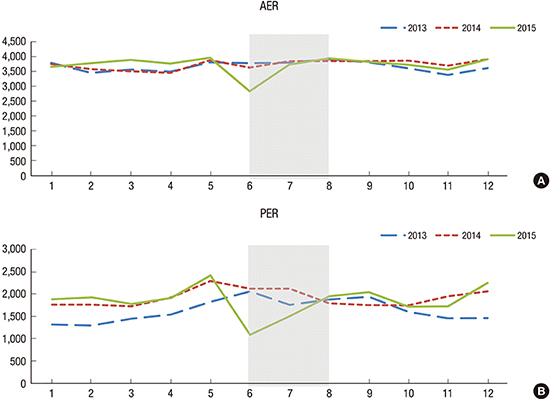
Fig. 2 shows a significant decrease in ED visits from June 1 to July 31, 2015 in comparison to the same period in 2013 and 2014. While the number of total pediatric patients in 2015 decreased, the proportions of infants (1.8%) and school-age children (4.8%) increased compared to those of the previous two years (Table 1).
Fig. 2
Number of patient visits per month to the Seoul National University Hospital ED from January 2013 to December 2015. (A) Total number of AER visits. (B) Total number of PER visits, total number of ED visits shows a sharp decrease of patients during MERS outbreak in 2015. The dark shading represents MERS period (June–July).
ED = emergency department, AER = adult emergency room, PER = pediatric emergency room, MERS = Middle East respiratory syndrome.
Table 1
ED pediatric patient volume by age group
| Age groups | PER | P | |
|---|---|---|---|
| 2013–2014 | 2015 | ||
| Infants (< 1 yr) | 542 (6.77) | 221 (8.59) | < 0.001 |
| Young children (1–4 yr) | 4,414 (55.15) | 1,248 (48.52) | - |
| School-aged children (5–17 yr) | 3,048 (38.08) | 1,103 (42.89) | - |
The most common symptom during the MERS period was fever (adult patients: 9.9%, pediatric patients: 31.5%). The most common diagnosis in adults was acute gastroenteritis (30.0%), followed by headache (7.5%) and dizziness (7.5%). The most common diagnosis in pediatric patients was acute gastroenteritis (19.0%), followed by acute pharyngitis (14.0%) and upper respiratory infection (6.0%). The most common symptom during the same period in 2013 was abdominal pain (8.7%) in the adult emergency room (AER) and fever (34.0%) in the pediatric emergency room (PER). For the same period in 2014, the most common symptom was also abdominal pain (9.7%) in the AER and fever (30.8%) in the PER. For 2013, the most common diagnosis in adults was acute gastroenteritis (22.4%) and for 2014 it was also acute gastroenteritis (15.3%). For 2014, the most common diagnosis for pediatric patients was acute pharyngitis (13.6%) and for 2014 it was upper respiratory infection (24.1%).
More patients were admitted to the ED by ambulance in 2015 compared to the 2013–2014 period in both the adult and the pediatric groups. The proportion of ESI level 1–3 increased in both adults (0.5%) and children (6.0%) and this change was statistically significant only in pediatric patients (P < 0.001). The number of adult patients who visited the ED due to illness increased, whereas the number who visited due to trauma decreased (1.4%). In children, these changes were diametrically opposite; proportion of visit due to trauma increased by 4.1% (P < 0.001). More adult (1.3%) and pediatric (7.2%) patients were admitted compared to the 2013–2014 periods. The EDLOS of hospitalized patients was significantly reduced in both adult (2.7 hours) and pediatric (1.8 hours) patients (Table 2).
Table 2
ED patients in 2013–2014 compared to 2015
DISCUSSION
This is the first study to analyze the utilization patterns of an ED during the MERS outbreak in Korea. During this period, the number of ED visits declined overall, with a predominance of low-acuity visits. These changes were more pronounced in the pediatric ED. In children, the number of visits of injured patients was greater than that of medically ill patients. On the other hand, in adults, the number of medically ill patients was greater than that of injured patients.
As in the US and Europe, PER utilization rates continue to increase in Korea (13141516). Especially in pediatric patients, the proportion of non-emergency patients with mild symptoms is relatively greater than that of adults who visit the ED (171819). Despite an increase in the number of primary care pediatric clinics since the 2000s in Korea, it was confirmed that the ratio of non-emergency patient visits to tertiary hospital EDs was still too high (15). Our results showed a decline in the number of non-emergency visits to the ED after the MERS outbreak. This means that there have been a relatively high number of cases of non-emergency ED visits and that another system other than the ED (i.e., after-hours clinics) could handle these needs.
Previous study showed an increase in the number of ED visits during an epidemic of a respiratory infection similar to MERS (i.e., H1N1 outbreak) (9202122). In that study, the number of pediatric ED patients suddenly increased by 19.7% during the H1N1 outbreak in comparison to an increase of 1% in adult patients (9). This sudden increase in the use of EDs was caused by a fear of the flu in which the media played a major role. Rubinson et al. (21) also showed that there was a 31% increase in the number of ED patients during the H1N1 epidemic. In 1987, during a forest fire disaster in California, the number of ED visits due to asthma and respiratory infections increased 1.4 times (23). In Korea, two studies analyzed the clinical and epidemiological characteristics of the H1N1 pandemic (2425). Nam et al. (25) compared the H1N1 pandemic period from October 2009 to March 2010 to the same months during the first three years. The number of patients who were admitted to the ED with symptoms of an upper respiratory tract infection was 15,217 during the pandemic period, although only 1,304 patients visited the ED one year later, showing that the utilization of EDs increased dramatically during the pandemic period. In contrast, our study showed that both the proportion of patients with mild symptoms and the number of ED visit decreased at the time of the MERS outbreak, which was a respiratory infection that was similar to H1N1. Unlike H1N1, the MERS infection in Korea was characterized by its spreading through hospital facilities. In particular, the ED was considered as a high-risk place of exposure, suggesting that the number of ED visits might have decreased at the time of the MERS outbreak.
Approximately 25%–30% of the patients who visit the ED are trauma patients, and the severity of trauma patients requiring hospitalization is greater in adults than in children (18). During the MERS outbreak period, the proportion of non-trauma patients who visited the adult ED increased by 1.4%, whereas the percentage of trauma patients increased by 4.1% in the pediatric ED. This is thought that pediatric or adolescent trauma patients could not be easily treated in primary medical institutions in Korea.
After the MERS period, ED volumes recovered very quickly. However, compared to the H1N1 outbreak, there was a difference. One study showed that during the H1N1 outbreak, ED visits for influenza-like illness peaked quickly in the first week of the outbreak and remained high for approximately 6 weeks (6). The reason why ED visits recovered so quickly was that the Korean government declared that the MERS outbreak had ended on July 28th and the World Health Organization (WHO) reported that MERS was no longer likely to spread in Korea (2627). When there were no newly reported infected patients, the anxiety about the MERS infection significantly decreased and patients visited the ED regularly as before. Also, our hospital had no infected MERS patients, so when the end of MERS was declared, ED visits resumed normal. It is possible that other EDs may not recovered as quickly. The results are limited to the interpretation as a result of a single hospital study. Therefore, it is necessary to study the number of patient visits to the ED after MERS in various local hospitals.
This study has some limitations. First, the retrospective, single-institution nature of this study is its main limitation. Because the patients in our study were enrolled at only one tertiary hospital, the results cannot reflect the characteristics of all ED patients in Korea. Future research is suggested, and a re-evaluation of all the data from emergency rooms at tertiary educational institutions in Korea during the same period is necessary. The analysis of data from the National Emergency Department Information System (NEDIS) is needed. Second, there might be unmeasured confounding factors that could have affected the outcomes such as an underlying disease. Third, the ESI level that we used might not completely reflect the true disease severity, as it is sorted based on the initial assessment of the acuity level, followed by the expected resource needs.
During the MERS outbreak period, the number of ED patients with a non-emergency situation decreased significantly. The decrease in pediatric patients was greater than that in adult patients. The sharp decline in ED use seems to be due to the increased public awareness of the ED as a hotbed of infection. This study shows changes in the use pattern of ED during the MERS epidemic in Korea.
 XML Download
XML Download