

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hypertension is among the most common diseases, with a prevalence of 33.7% in the Korean adult population (1). Uncontrolled hypertension is a major risk factor for cardiovascular disease, stroke, and other hypertension-associated morbidities (2).
Although many available antihypertensive agents substantially reduce the risk of hypertension-associated morbidities, blood pressure control in the general population remains suboptimal (2). Poor medication adherence and persistence were identified as a significant contributing factor to uncontrolled hypertension (3). Numerous studies investigated the rate of adherence to antihypertensive therapy and associated factors (4). However, persistence, another term for medication-taking behavior, is a relatively new descriptor that is different from adherence. Persistence is defined as the length of time during which physicians continue to prescribe therapy, while adherence represents the ratio of medication supply days over a given interval (5). Together, persistence and adherence and can provide a better understating of factors related to effective blood pressure control (6).
The discontinuation rate for antihypertensive drugs ranges from 50%-60% after 6 months (7), and many studies have investigated persistence with hypertensive therapy (689101112). Although information about persistence with antihypertensive therapy in patient populations from North America or Europe is plentiful, limited studies have addressed this in Asian populations. Previous studies conducted in Korea reported only cumulative medication adherence, as measured by the medication possession ratio (MPR) (1314). Persistence with antihypertensive therapy and related factors have not been investigated in this population. In addition, most previous studies included patients with both complicated and uncomplicated hypertension, so persistence data in patients who are free from hypertension-associated complications is limited (15).
We aimed to assess one-year persistence and adherence to antihypertensive therapy among newly treated uncomplicated hypertensive patients in Korea and to evaluate the influence of initially chosen therapeutic class on persistence and adherence.
MATERIALS AND METHODS
We conducted a retrospective cohort study using the National Health Insurance claims database provided from the Health Insurance Review Agency (HIRA), which contains medical service claims from 2011 to 2013. Information about prescription and medical service for almost all Koreans is included in the HIRA's claims database.
Study population
We included adult patients with uncomplicated hypertension who received their first antihypertensive agent as a monotherapy in 2012. Included patients had a diagnosis code of hypertension in the 2012 claims data and did not have diagnosis codes for hypertension (International Classification of Diseases, ICD-10, I10, I11, I12, I13 or I15) and related complications or any antihypertensive prescriptions during the 12 months before the first date of antihypertensive prescription in 2012 (index date). Hypertension-related complications were defined as cardiovascular disease (I20-I25, I30-I52), cerebrovascular disease (G45, I60-I63, I65-I69), peripheral vascular disease (I70-I79, Z95.8, Z99.2), renal disease (N03-N05, N18, N19, Z49, Z94.0, Z99.2), diabetes mellitus (E08-E11, E13) and pregnancy (O00-O9A).
In order to measure persistence and adherence, we excluded patients who had less than 7 days of total antihypertensive supply, more than 7 hospitalization days, or less than two antihypertensive prescriptions during one year following the index date. After building a final cohort, we randomly selected 20% of the patients in the cohort for analysis. We classified the cohort into six groups according to the therapeutic class of the initially prescribed medication: angiotensin receptor blockers (ARB), angiotensin converting enzyme inhibitors (ACEI), selective beta blockers (BB), dihydropyridine calcium channel blockers (CCB), thiazide diuretics (D), and others.
Study variables
The main dependent variables were medication persistence and adherence. Persistence was defined as continuation of therapy without a prescription gap of 60 days. In other words, having more than 60 days of prescription gap was considered as discontinuation of therapy. The duration of persistence was estimated with the number of days from the index date to either the first 60 day prescription gap or the cohort end date (one year after the index date). Treatment and class persistence were estimated based on any antihypertensive medications and medications belong to same antihypertensive class as the first prescription (index class), respectively. Treatment adherence was calculated using the medication possession ratio (MPR), which was obtained by dividing the number of days covered by antihypertensive prescription by the cohort period of 365 days. When calculating the number of days covered, we treated all antihypertensive medications as the same medication. If the last antihypertensive supply exceeded the cohort end date, it was truncated. MPRs ≥0.8 were regarded as being adherent.
Demographic characteristics such as age, sex, and insurance type were evaluated at baseline for each patient. In addition, the Charlson Comorbidity Index (CCI) score, a prognostic comorbidity assessment score calculated based on 19 disease conditions, was obtained to assess the disease burden of each patient for 1 yr before the index date using diagnosis codes (16). The presence of specific diseases such as dyslipidemia, dementia, and depression, which are known to affect medication taking behavior, was also identified.
Statistical analysis
Descriptive statistics such as mean, standard deviation, and percentage were calculated for demographic data and study variables. Each cohort was compared with the ARB cohort, which was used as the standard of comparison. To compare continuous variables and categorical variables between two groups, we performed the Student's t-test and chi square test, respectively. Kaplan Meier method and log-rank test were used to compare treatment persistence rate. Adjusted hazard ratio (aHR) and corresponding 95% confidence interval (CI) for the risk of treatment and class non-persistence were assessed with a multivariate Cox-proportional hazard model. The adjusted odds ratio (aOR) and corresponding 95% CI for adherence were estimated using multiple logistic regressions. Adjustments were made for age, gender, CCI score, insurance type, and baseline disease including depression, dementia and dyslipidemia. For all tests, a P value less than 0.05 was considered statistically significant. Statistical analyses were performed with SAS 9.3 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
Patient selection and demographic data
We identified 471,845 uncomplicated hypertensive patients who started antihypertensive agents in 2012. After excluding patients with more than 7 days of hospitalization (n=7,447) and those with only one antihypertensive prescription (n=66,972), 397,426 patients were left. Among these, 57.60% (228,925 patients) were prescribed monotherapy as an initial therapy, and we randomly selected 20% of this cohort (45,787 patients) for the final analysis. The final group was classified into six cohorts based on the initially prescribed drug class: CCB cohort (43.71%), ARB cohort(40.33%), BB cohort (10.02%), D cohort (3.62%), ACEI (1.21%), and other (1.11%).
The mean age of the cohort was 55.08 yr. On average, patients belonging to the CCB, D and other cohorts were older than those in the ARB cohort. Patients in the BB cohort were younger than those in the ARB cohort. The proportion of very elderly patients (more than 80 yr) was highest in the D cohort. The total cohort was predominantly male (52.08%), but ACEI, BB, and D were more frequently prescribed to females. The proportion of patients who received medical aid was highest in the D cohort (8.56%) and lowest in the ARB cohort (3.44%). The Charlson comorbidity score at baseline was very low (0.31±0.76), though the BB, D and others cohort was greater than average (Table 1).
Persistence and adherence
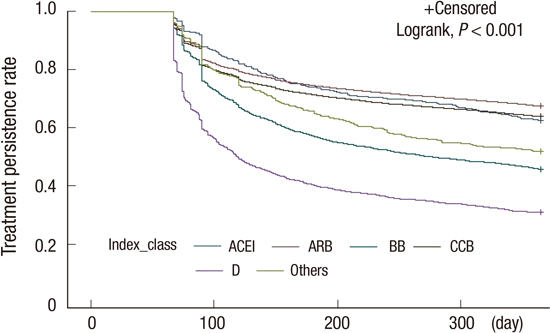
In total, 62.07% of patients were persistent with antihypertensive treatment after 1 yr of treatment, with a mean duration of 276.5±123.1 days. The proportion of patients persistent with any antihypertensive therapy was highest in the ARB cohort (67.39%), followed by the CCB (63.78%), ACEI (62.41%), BB (45.62%), and D (30.76%) cohorts.
The initial class was continued in 42.00% of overall patients at the end of one year. The proportion of patients remaining on the initial class at one year was greatest in the CCB cohort (44.42%) and the ARB cohort (43.55%), followed by the ACEI (35.25%), BB (34.95%), and D (15.50%) cohorts. When considering all patients, 64.24% were adherent to antihypertensive treatment. The MPR was highest in the ARB cohort (0.79± 0.28) and lowest in the D cohort (0.55±0.37).
Predictors of persistence and adherence
After adjusting for age, gender, co-morbid disease, and insurance type, initial use of D (aHR, 3.16; 95% CI, 2.96-3.74) and BB (aHR, 1.86; 95% CI, 1.77-1.95) significantly increased the risk of discontinuing any antihypertensive treatment compared with ARB. We observed a small increase with CCB (aHR, 1.12; 95% CI, 1.08-1.15), while no change with ACEI (aHR 1.12; 95% CI 0.98-1.29) was observed (Table 2).
Contrary to similar rate of persistence with overall antihypertensive treatment observed in ARB and ACEI cohort, the likelihood of non-persistence with the initial drug class was greater in patients who started ACEIs rather than ARBs (aHR, 1.15; 95% CI, 1.03-1.28). Adjusted Kaplan Meier curve of treatment persistence rate over the first year compared among initial therapeutic classes are shown in Fig. 1.
The initial choice of medications other than ARB decreased the likelihood of adherence to overall antihypertensive treatment, particularly for the D (aOR, 0.28; 95% CI, 0.25-0.31) and BB cohorts (aOR, 0.43; 95% CI, 0.41-0.46) compared with the ARB cohort. No difference between the CCB and ARB cohorts was observed.
Regardless of initial therapeutic class, very elderly patients aged ≥80 yr were at high risk of antihypertensive treatment discontinuation and non-adherence. However, female patients, patients aged 65-79 yr, and patients with dementia or dyslipidemia were more likely to persist and adhere to the treatment. Multivariate analysis of factors affecting class non-persistence showed similar trends with treatment non-persistence, with the exception that class non-persistence did not differ between very elderly patients and adults aged <65 yr (Table 3).
DISCUSSION
A nationwide cohort study using claims data in Korea confirmed that the initial choice of antihypertensive agent could affect persistence with antihypertensive treatment in uncomplicated hypertensive patients. Specifically, treatment persistence over the first year was best in patients with initial ARB therapy, with similar results in those treated with ACEI and CCB. Patients with BB use had medium treatment persistence, while persistence was worse in patients with initial D use. These results were in line with previous studies conducted in Western countries (8910). Recently, Mancia et al. (9) reported that the risk of discontinuation of antihypertensive therapy was minimal in ARB (HR, 0.3; CI, 0.29-0.30), followed by ACEI (HR, 0.35; CI, 0.35-0.36), calcium channel blockers (HR, 0.52; CI, 0.51-0.53), and beta-blockers (HR, 0.5; CI, 0.53-0.55) in comparison with diuretics. Hasford et al. (6) reported that the rate of treatment persistence was higher in patients with ACEI (32.5%) and ARB (32.2%) as the initial drug class, followed by calcium channel blockers (30.4%), beta-blockers (27.7%), and diuretics (24.9%). In another report, the difference in odds of treatment persistence compared with thiazide or thiazide like diuretics was largest in ACEI (aOR, 1.75; CI, 1.72-1.78) and ARB (aOR, 1.57; CI, 1.51-1.63), medium in calcium channel blockers (aOR, 1.36; CI, 1.33-1.40) and minimal in beta-blockers (aOR, 1.02; CI, 1.00-1.04) (8). On the contrary, Trimarco et al. (11) reported no differences in treatment persistence between thiazide diuretics and other classes of antihypertensive monotherapy as the starting drug in an open label randomized study.
The observed low adherence and persistence with overall treatment in thiazide initiators could be associated with tolerance to medications. Previous reports demonstrated the results that proportion of patients experiencing adverse symptoms were highest with thiazides (9.9%) and lowest with ARB (0.0%) when administered standard doses (17). Based on these published results, we inferred that patients who experience adverse symptoms with use of blood pressure lowering agents at the time of hypertensive treatment initiation tend to avoid use of any other agents.
The effects of initial antihypertensive choice on the continuation of the initial class were consistent with previous studies investigating persistence related to initial drug choice (1218). Class persistence with the ACEI was lower than ARB, which is in agreement with previous reports (81218). Although no difference was observed in overall treatment persistence, patients initiated antihypertensive drug treatment with ACEI tend to switch more frequently than ARB. Medication tolerability is a potential challenge to persistence, and the lower incidence of dry cough in ARBs compared with ACEI is associated with better persistence (19). Most previous reports showed lower class persistence with calcium channel blockers compared to ARBs (820). However, we observed similar class persistence in CCB and ARB cohorts, as previously reported (21). Analysis including only dihydropyridine calcium channel blockers can partly explain the better persistence observed when compared to previous reports. We did not include non-dihydropyridine calcium channel blockers because these are not primarily prescribed for uncomplicated hypertension; rather, they are used for other indications, such as angina pectoris or cardiac arrhythmias.
Persistence to therapy can differ from country to country; these measurements are important because they can be affected by health system and socioeconomic status, and they improve over time. In this study, 62.1% of patients were persistent with antihypertensive treatment during the first year, which is lower than rates in the elderly population from the US, the Netherlands, and Canada (75%) (22), similar to a recent report from Canada (64.6%) (8) and higher than rates in Germany (24.9%-32.5% among monotherapy initiators) (6).
Persistence to antihypertensive therapy has not been investigated previously in a Korean population. However, treatment adherence, which is intrinsically linked with persistence (23), has been studied. The proportion of adherent patients (MPR ≥ 0.8) in this study (64.2%) was much higher than previous reports from a similar Korean population who started antihypertensive therapy in 2005 (39.2%) and 2009 (59.4%) (1314). This phenomenon may have resulted from various interventions to improve adherence and persistence.
Other factors shown to affect persistence and adherence were age, gender, and underlying disease such as dementia and dyslipidemia. Older patients aged 65-79 yr were more likely to be persistent or adhere to treatment, while very elderly patients aged 80 yr and above were less likely to persist or adhere compared with adults ≤65 yr. The reported effect of age on adherence or persistence is uncertain, but in general older patients were more persistent than younger patients (2425). Poor persistence in very elderly patients (≥75 yr) has been reported (822). In line with previous reports (222526), women were more likely to be persistent and adherent to treatment. Dyslipidemia is associated with higher adherence in newly diagnosed hypertensive patients, which was consistent with our findings (26). Unlike previous reports (927), we also found that patients with dementia were more likely to be persistent and adherent to therapy. This discrepancy is not explained by our findings.
This study demonstrates different prescription pattern of first line antihypertensive agent in treatment of uncomplicated hypertensive patients, when compared to other countries. The CCB and ARB were prescribed most frequently whereas the use of D and ACEI as initial monotherapy was minimal in uncomplicated hypertensive patients. The prevalent use of CCB in uncomplicated hypertensive patients was similar to usage in Taiwan (28). The minimal use of ACEI as initial monotherapy was remarkably different from other countries, where ACEI are one of the most frequently prescribed classes (8). This can be explained by the high prevalence of ACE inhibitor-induced dry cough (29) and by comparable drug prices of ARB with ACEI in Korea. This is not true for other countries, where significant cost savings by the restriction of access to ARB has been reported (30). We also observed a significantly low utilization rate of thiazide diuretics, the least expensive hypertensive agents, as monotherapy, which is also significantly different from observations of other countries (31). The observed low prescription rate of BB indicated negative findings regarding clinical outcomes in hypertensive patients without compelling indications for these drugs (32).
This study shows the real-world prescription and adherence pattern of antihypertensive drug in uncomplicated treatment naïve patients, using national claim data in Korea. Although head to head comparison may not be appropriate due to different health insurance system and degree of financial burden imposed for medication and medical services between countries, the effect of initially chosen antihypertensive class on treatment adherence and persistence were similar to previous reports. Given ever increasing socioeconomic burden of hypertensive complications partially caused by treatment non-persistence, the result of this study could be helpful information for the clinicians and policy-makers in deciding initial hypertensive treatment agent.
Although the large scale data source is strength of our study, some limitations should be considered. First, we could not adjust baseline characteristics when we compared outcome data among 6 cohorts. For example, average age in the CCB and D cohorts was much higher than in other cohorts. However, the observed differences in the risk of non-persistence among initially prescribed class were adjusted by age, gender, and concomitant disease through multivariate analysis. Second, we did not consider other confounding factors such as socioeconomic status, which affect treatment persistence. Third, we could not assess disease severity due to the lack of blood pressure data. However, to minimize this confounding effect, our study was limited to patients who started with monotherapy. Therefore, the treatment persistence of patients who started combination therapy could not be evaluated. Previous studies reported that starting with combination therapy favors persistence, mainly due to the severity of hypertension at diagnosis that informs patients about the importance of pharmacotherapy. Further work is warranted to investigate persistence among combination initiators in this population.
In conclusion, this study provides new and updated information about treatment persistence and adherence in uncomplicated hypertensive patients using national insurance claims in Korea. More than 60% of patients maintained antihypertensive therapy at least one year after treatment initiation. The results support previous findings that initially prescribed antihypertensive drug class influences the treatment persistence and adherence with minimal differences among ARB, ACEI, and CCB. Relatively low persistence was observed with BBs and was lowest in diuretics as initial drug. The prescription prevalence of BB, ACEIs, and diuretics as initial monotherapy was significantly low in patients without compelling indications.

 XML Download
XML Download