

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Depressive disorders have been of growing concern to mental health specialists globally (1, 2, 3). Among patients with diagnosed depression, alcohol use disorder (i.e., alcohol abuse or dependence) is a common psychiatric disease. In a cross-national comparative study conducted in 2001-2002 (4), the rate of alcohol dependence in Korea was higher (5.1%) than the US (4.4%). Conversely, the prevalence of alcohol abuse in Korea (2.0%) was compared with the US (5.3%). Moreover, major depression and dysthymia was suggested as the most significant comorbid psychiatric disorders in patients with alcohol abuse and dependence in two-stage cluster sampling in Korea in 1984 (5). In a nationwide epidemiological study conducted in the US, the rates of alcohol abuse and alcohol dependence in patients with major depression were 47.3% and 21.0%, respectively (6). The relationship between depression and alcohol disorders is generally viewed as reciprocally causal in nature rather than due to random overlap. However, other disease models have been proposed: some have suggested that the disorders co-exist independently in individuals; others have posited one-way causality in that depressive disorders are alcohol-induced; some have hypothesized that a third factor is the cause of the comorbidity such as a shared genetic and environmental factor(s) (7). Brière et al. (8) demonstrated that rates of comorbidity of major depression and alcohol use disorder are significantly higher in early adulthood (11.0%) than in either adolescence (2.0%) or adulthood (7.0%). Since concomitant alcohol abuse can exacerbate and prolong a depressive episode (9), patients with this comorbidity might benefit from additional clinical scrutiny.
The World Health Organization (WHO) defines hazardous drinking as a pattern of alcohol consumption that increases the risk of harmful consequences; it defines harmful levels of alcohol consumption as >40 g/day for men and >20 g/day for women (10). The National Institute of Alcohol Abuse and Alcoholism (NIAAA) defines hazardous drinking as >21 standard drinks/week or >7 standard drinks/day for men, and >14 standard drinks/week or >5 standard drinks/day for women (11). To date, clinical factors associated with hazardous drinking in depressive patients have not been thoroughly investigated in the medical literature. The Clinical Research Center for Depression (CRESCEND) study in Korea was the first large, prospective, observational study of a nationwide sample of patients with depression to provide extensive epidemiological data using psychometric scales (12). The aim of the present study was to investigate clinical factors associated with hazardous drinking in the CRESCEND study patients, using the Alcohol Use Disorder Identification Test (AUDIT) as a psychometric tool to identify hazardous drinking behaviors.
MATERIALS AND METHODS
Study overview
A more detailed description of the CRESCEND study and protocol can be found elsewhere (12). Patients with depression were recruited at 18 study centers nationwide, including 16 university-affiliated hospitals and 2 general hospitals in Korea from January 2006 to August 2008. Data collection was managed and monitored by the Department of Preventive Medicine of the Catholic University College of Medicine in Seoul. All demographic and clinical data were collected by trained and certified clinical research coordinators, who were supervised by clinical psychiatrists at the regional centers. All data were recorded using a standardized clinical report form and stored on the website of the CRESCEND study (www.smileagain.or.kr).
Subjects
The CRESCEND study adopted broad inclusion criteria and minimal exclusion criteria to reflect current psychiatric clinical practice in Korea: It recruited 1,183 depressed patients who were beginning psychopharmacological treatment for first-onset or recurrent depression, and who gave written informed consent prior to study participation. For the purpose of the present study, additional inclusion criteria were adopted: 1) age greater than 18 yr; 2) a diagnosis of non-psychotic major depression, dysthymic disorder, or other non-specific depressive disorder according to the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) (13), and confirmed by a Structured Clinical Interview for DSM-IV (SCID) (14); 3) the total score ≥8 on the Hamilton Depression Rating Scale (HAMD) (15) and 4) availability of a fully completed Alcohol Use Disorder Identification Test, Korean version (AUDIT-K) (16). The resulting cohort meeting these criteria consisted of 402 patients, 332 (82.6%) patients with non-psychotic depression, 15 (3.7%) patients with dysthymia, and 55 (13.7%) patients with other non-specific depressive disorder. Based on the recommendation in Zimmerman et al. (17), in terms of depressive symptom severity, patients with mild, moderate, and severe depression were 127 (31.6%), 174 (43.3%), and 101 (25.1%), respectively. History of previous depressive episodes was reported by about half of the subjects; the mean number was 1.9 (SD=2.0).
Screening hazardous drinking with the AUDIT-K
The Alcohol Use Disorder Identification Test (AUDIT) is a reliable and valid screening tool for hazardous drinking. The WHO developed the tool in 1989 to evaluate alcohol consumption, drinking frequency and the damage it causes, and to screen for hazardous drinking behavior (8). The AUDIT is a self-reported questionnaire consisting of 10 items with a minimum score of 0 and a maximum score of 40. In a large standardization study of its Korean version (AUDIT-K), scores of 10 for men and 6 for women were defined as cut-off scores for hazardous drinking. A higher score on the AUDIT-K indicates more severe (hazardous) drinking behavior (16).
Demographic and clinical characteristics
The study collected a wide range of demographic data on participants including age, sex, marital status, occupation, education, religion, and monthly income. The clinical data of interest included age at the onset of the first depressive episode, inpatient/outpatient status, history of depressive episodes, number of previous depressive episodes, history of suicidal attempts, family history of depression, concurrent physical diseases, and current smoking status. As recommendation of Zimmerman et al. (17), depressive symptom severity was classified by the following severity range for the HAMD: mild depression (8, 9, 10, 11, 12, 13, 14, 15, 16); moderate depression (17, 18, 19, 20, 21, 22, 23); and severe depression (≥24).
Assessment scales
Clinician-administered scales consisting of the HAMD, the Hamilton Anxiety Rating Scale (HAMA), the Brief Psychiatric Rating Scale (BPRS), the Clinical Global Impression of Severity scale (CGI-S), and the Social and Occupational Functioning Assessment Scale (SOFAS) were used to evaluate depressive symptoms, anxiety symptoms, psychotic and other symptoms, global severity, and levels of social and occupational functioning, respectively (16, 18, 19, 20, 21). In addition, we used a raft of self-reported questionnaires, including the Scale for Suicidal Ideation (SSI-Beck) and the WHO Quality of Life questionnaire-abbreviated version (WHOQOL-BREF), to evaluate the severity of current suicidal ideation and quality of life, respectively (22, 23). All survey instruments had been formally translated into Korean, and their validity and reliability had been confirmed in Korean populations (24, 25). Higher scores on the HAMD, HAMA, BPRS, CGI-S, and SSI-Beck scales correspond to more severe symptoms, while lower scores on the SOFAS and WHOQOL-BREF indicate poorer overall function. In addition, individual items on the HAMD were used to compare the diverse and complex dimensions of depressive disorder in patients with and without hazardous drinking habits. All data collectors received training twice a year, with a formal consensus meeting to agree on the application of the assessment instruments.
Statistical analysis
Demographic and clinical characteristics and the assessment scale scores were compared between patients categorized with and without hazardous drinking behaviors. The independent t-test was used to assess statistically significant differences for continuous variables, while the chi-square (χ2) test was used to assess statistically significant differences for discrete variables. A binary logistic regression model was also fitted to identify independent predictors of hazardous drinking behavior. In this model, the hazardous drinking group was defined as the dependent variable, and the non-hazardous drinking group was as the reference category. In addition, clinical variables shown to be significantly different between the two groups were tested as covariates. Goodness of fit was used to select and validate the final model. Statistical significance was set at P<0.05 (two-tailed) for all tests. All statistical analyses were performed using SPSS 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
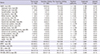
As shown in Table 1, the prevalence of hazardous drinking among 402 patients with depressive disorders was 51.0%. Depressed patients with hazardous drinking behavior were younger (40.2 yr, SD=14.6 vs. 45.1 yr, SD=14.5; t=-3.335, P=0.001) and a disproportionately higher proportion of male (n=88, 42.9% vs. n=63, 32.0%; χ2=5.133, P=0.023) than those without hazardous drinking behavior. Hence, using the analysis of covariance for continuous variables and binary logistic regression analyses for discrete variables, the two group differences with the adjusting for the effects of age and sex were analyzed. There were no significant differences between the hazardous and non-hazardous drinkers for diagnosis (χ2=0.180, P=0.914) and depressive symptom severity (χ2=0.110, P=0.574).
A comparison of the demographic and clinical characteristics of depressive patients with and without hazardous drinking behaviors
As shown in Table 1, depressive patients with hazardous drinking behavior were more likely than non-hazardous drinkers to be current smokers (adjusted odds ratio [aOR], 3.043; P<0.001) and have a history of suicidal attempts than non-hazardous drinkers (aOR, 1.968; P=0.005).
There were no significant differences between the hazardous and non-hazardous drinkers for the following variables: marriage status (aOR, 0.409; P=1.370), employment status (aOR, 1.152; P=0.561), educational attainment (F=0.420, P=0.517), religious affiliation (aOR, 0.952; P=0.813), monthly income (aOR, 1.157; P=0.483), age at onset (F=0.289, P=0.591), enrollment as outpatients (aOR, 0.357; P=0.778), history of depressive episodes (aOR, 0.914; P=0.662), number of previous depressive episodes (F=0.001, P=0.977), family history of depression (aOR, 1.238; P=0.474), or comorbid physical diseases (aOR, 0.801; P=0.371).
A comparison of assessment scale scores between depressive patients with and without hazardous drinking behaviors
As shown in Table 2, the hazardous drinking group had statistically significantly higher scores on several HAMD items, including suicidal ideation (F=7.648, P=0.006), psychomotor retardation (F=5.238, P=0.023) and weight loss (F=4.526, P=0.034), and lower scores for hypochondriasis (F=6.805, P=0.009) than the non-hazardous drinking group. In addition, the hazardous drinking group had a higher total score on the SSI-Beck (F=14.165, P<0.001).
However, there were no statistically significant differences between the two groups in terms of their total scores on the HAMD (F=1.414, P=0.235), HAMA (F=0.007, P=0.936), and BPRS (F=0.798, P=0.372), nor for the scores on the CGI-S (F=0.221, P=0.639), SOFAS (F=1.061, P=0.304). There was also no statistically significant differences on important HAMD items, including depressed mood (F=2.449, P=0.118), feelings of guilt (F=1.809, P=0.179), early insomnia (F=1.192, P=0.276), middle insomnia (F=0.079, P=0.778), late insomnia (F=0.079, P=0.778), work and activities (F=0.009, P=0.926), psychomotor agitation (F=0.935, P=0.334), psychological anxiety (F=0.825, P=0.364), somatic anxiety (F=0.032, P=0.858), gastrointestinal somatic symptoms (F=1.431, P=0.232), general somatic symptoms (F=0.797, P=0.373), genital symptoms (F=1.007, P=0.316), and insight (F=0.348, P=0.556).
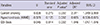
A binary logistic model for predicting hazardous drinking in depressive patients
The Hosmer-Lemeshow goodness-of-fit test validated the logistic model (χ2=9.145, df=8, P=0.330). After the effects of age and sex of the study participants were adjusted, the initial covariates in the binary logistic model were history of attempted suicide, current smoking, scores on several HAMD items including psychomotor retardation, hypochondriasis and weight loss, and total score on the SSI-Beck. Forward selection of the model was performed to avoid issues related with multicollinearity. As shown in Table 3, the final model explained 16.2% (Nagelkerke R2) of the variability in hazardous drinking, and showed that a higher score on the SSI-Beck (P=0.002, aOR, 1.046; 95% confidence interval [CI], 1.017-1.076), current smoking (P=0.002, aOR, 2.311; 95% CI, 1.349-3.960), and a lower hypochondriasis score (P=0.002, aOR, 0.685; 95% CI, 0.536-0.875) were independently associated with an increased likelihood of hazardous drinking in depressed patients.
DISCUSSION
The prevalence of hazardous drinking behavior among depressive patients in this study was 51.0%, which is comparable to or marginally higher than the frequencies reported elsewhere. In a nationwide observational study of patients with major depression in the US, the prevalence of hazardous drinking was 47.3% (6). In the sequenced treatment alternatives to relieve depression (STAR*D) trial, 11.0% of 1,376 depressed outpatients were diagnosed with alcohol abuse or dependence (26). In the Netherlands study of depression in older persons (NESDO), at-risk drinkers (AUDIT≥5) comprised 19.0% of 373 patients (27). Similarly, in the Netherlands study of depression and anxiety (NESDA), the rates of remitted and current hazardous drinking among 1,369 patients with depression and/or anxiety were, 22.4% and 9.3%, respectively (28). In Korea, the age-adjusted prevalence of hazardous drinking was 38.8% among 6,276 adult participants in the 2009 Korean Health and Nutrition Examination Survey (KNHANES) (29). There is no simple explanation for these differences in prevalence among similar and dissonant populations; however, unlike in the US and other countries, the higher prevalence of hazardous drinking in Korea has been demonstrated in two nationwide epidemiological studies (30, 31). Other explanations for the divergence have focused on potential cultural differences: a more permissive attitude towards harmful levels of drinking is more common in Korean culture than in others (32). The difference also may be a function of different diagnostic tools: in depressed patients, the AUDIT scale is known to detect alcohol dependence rather than mere alcohol abuse among depressives (28). This may be caused by the high proportion of female and outpatient subjects included in this study, and higher AUDIT cutoff scores than those employed by Dybeck et al. (33), Gual et al. (34), and Gache et al. (35) (5, 7, and 6, respectively), our study observed a higher prevalence of hazardous drinking among depressives.
The literature consistently has identified younger individuals and males as two factors predicting hazardous drinking; this was also the case in our study. A 12-month study of alcohol abuse and dependence in the US demonstrated that younger patients who were male had a more common history of alcohol abuse/dependence among subjects with major depressive disorders. Indeed, hazardous drinking behavior appears to be one of several distinctive clinical features that point to a greater burden of disease in patients with early-onset depressive disorders. In terms of history of depressive episodes, we observed no difference between the hazardous and non-hazardous drinkers. However, Sher et al. (36) found that depressed patients with concomitant alcohol abuse had experienced greater previous depressive episodes than their counterparts. Different inclusion criteria may be a partial explanation for this discrepancy with our findings: in contrast to the inclusion criteria of Sher et al. (36), we only recruited patients who began the psychiatric treatment for first-onset or recurrent depression.
Another of this study's major findings is also found in the literature: a greater severity of current suicidal ideation and more previous suicide attempts are more common in patients with hazardous drinking habits. A previous epidemiological study suggested that, in patients with concurrent depressive and alcohol use disorders, depression exerted a stronger effect on suicide-related cognition and behaviors (37). A study of a community-based sample in Korea observed a significant association among unplanned suicidal attempt(s), alcohol use disorder, and major depressive disorder (38). In addition, East-Asians who have major depressive disorder, regardless of depressive symptom severity, have a suicidal risk that is significantly associated with melancholic features and hostility (39). Moreover, atypical features of a major depressive episode including hypersomnia and hyperphagia were associated with both alcohol abuse and suicide attempts (40). Therefore, impulsivity, hostility and reversed vegetative symptoms of depression may be among the factors that contribute to the development and escalation of suicidal ideation in depressive patients who are hazardous drinkers.
Interestingly, a participant's total score on the HAMD was not significantly different between the hazardous and non-hazardous groups in our study. This finding is partly consistent with Rodgers et al. (41), who first showed that the relationship between the severity of depression and alcohol use was U-shaped rather than linear in relationship. This was later explained by psychosocial factors in early adulthood. In particular, distress tolerance has been suggested as a significant moderator of the relationship between depressive symptoms and problematic alcohol use (42). This relationship also appears to be moderated by gender (43). In our study, the specific manifestations of depression linked to hazardous drinking included higher levels of psychomotor retardation and weight loss, as well as lower levels of hypochondriasis. Hypochondriasis is typically defined as the unfounded fear of having a disease (44). Previous research has shown that hypochondriacal worry is a common manifestation in depression (45). Hence, one could propose that the low levels of hypochondriasis in hazardous drinkers represent their own denial of physical problems or diseases. Hence, depressed patients with hazardous drinking behavior may continue alcohol consumption. An item response analysis of the DSM-IV criteria for MDD showed that psychomotor retardation was a solid predictor of the severity of depression (46). It could be hypothesized that severity of depression contributes indirectly to the development of alcohol use disorders in depressed patients. Indeed, because early-onset depressive mood may be a factor that facilitates the initiation of alcohol consumption, the relationship between depressive mood and concomitant hazardous drinking in depressed patients also warrants robust discussion from the perspective of developmental psychiatry.
Our finding that depressed patients with hazardous drinking habits had higher rates of current smoking is consistent with the report by Holma et al. (47) that smoking has a strong relationship with alcohol use disorders and personality disorders in adults with major depression. Moreover, the relationship between smoking and depression was found to be independent of the patterns of alcohol consumption, being stronger for women than men, but it could be mediated by several intervening factors (48). In a 13-yr population-based longitudinal study, smoking was independently associated with depression, anxiety, and parasuicide among young adults. The same study found that hazardous drinking was associated with a lower quality of life (49), which cannot be simply explained in terms of depressive symptoms alone or hazardous drinking. It is probable that alcohol abuse contributes to an unfavorable course of depression associated with an increased burden of disease, which also reduces the overall quality of life.
Finally, our binary logistic regression model showed that higher levels of current suicidal ideation, greater frequency of current smoking, and lower hypochondriasis were associated with an increased likelihood of hazardous drinking behavior. In other words, it suggests that there is a close yet independent link between current smoking status, hypochondriasis, suicidal ideation, and hazardous drinking behavior in depressed patients. This finding is not only consistent with theoretical conclusions of previous studies, but also provides evidence of common neural substrates. Interestingly, the finding that hypochondriasis was an inverse predictor of hazardous drinking in our study is controversial. It is possible that hypochondriasis is an unconventional manifestation of hazardous drinking in depressed patients, although this would fail to negate the finding that these patients experience more severe symptoms and a greater burden of illness than non-hazardous drinkers.
This study has several limitations. First, comorbidities, including personality disorders, were not taken into consideration. As a result, our discussion of any intervening factors between hazardous drinking and depression has a limited scope to other populations. Second, the clinical significance of our findings may be relatively small. It cannot be ruled out that the study's large sample size or the broad inclusion criteria influenced our findings. Third, Bonferroni correction to reduce familywise error due to multiple comparisons was not performed during data analysis. Thus, the clinical relevance of our findings should be interpreted with caution, particularly regarding the level of significance used to classify findings as 'significant.' Fourth, age at onset of alcohol consumption, history of black out(s), and other substance-related clinical data were not considered in our study. Fifth, comorbid conditions for personality disorders were also not evaluated; as a result, the potential influence of comorbid personality disorders on the status of hazardous drinking was not analyzed. Sixth, consistent with documentations of Jeon et al. (50), specific depressive symptoms are expressed differently cross-culturally. In particular, Korean patients have experienced less frequent depressed moods and more frequent suicidal ideation than Americans. Hence, these cross-cultural differences can contribute to the under-diagnosis of depressive disorder and close relationship between hazardous drinking and suicidal ideation in Korea. Lastly, there was no formal inter-rater reliability study to assess the reliability of the psychometric methods.
Despite these limitations, the study provides a comprehensive comparison of diverse clinical characteristics of patients with and without hazardous drinking behavior. We also show that current smoking status, suicidal ideation, and hypochondriasis are independent predictors of hazardous drinking in depressed patients. In this context, screening depressed patients for alcohol abuse may help to identify those who could benefit from more comprehensive therapeutic approaches.

 XML Download
XML Download