

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Various managements for restoring volume to the body or rejuvenation of facial wrinkles with injectable materials have been described over the last 100 yr. Autogenous fat graft was firstly performed for the correction of facial soft tissue defect at 1893 (1). In the beginning of 20th century, liquid paraffin was injected for the facial contouring in Vienna (1). In spite of substantial complications and public backlash, alternative injectable substances were explored.
Liquid silicone was used to improve body contouring in Switzerland and Japan during the 1940s and facial injections of liquid silicone was generalized and common procedure for rejuvenation in the 1960s, particularly with the microdroplet injection technique (2).
There was a great development of injectable fillers in 1981 with initial U.S. Food and Drug Administration (FDA)'s approval of bovine collagen fillers (Zyderm, Zyplast; Inamed Aesthetics, Santa Barbara, California) for cosmetic use (1). After that, bovine collagen became the standard for injectable materials. The new era of injection with synthetic selective bioactive fillers began in 2003, when a Restylane (Medicis, Scottsdale, Arizona) became FDA approved product. Since then, the FDA has approved a variety of fillers for cosmetic use, mostly in the European market. This has led to a boom in the use of injectable fillers (1). Many filler types have been developed, resulting in expectations for reduced complications. However, variable complications have been reported.
IDEAL MATERIAL
Ideal injectable fillers should possess the following characteristics. We evaluated the safety and efficacy to decide whether a material is ideal or not. The injectable filler materials should be safe, biocompatible, resistant to infection, and fixed to the surrounding tissue as well as should maintain its volume for wrinkles and body contouring. It would be better induce a minimal foreign body reaction, including granuloma formation. And ideal materials for injection should not be teratogenic, carcinogenic and allergenic; not require pretesting; be painless, and inexpensive; and stable when stored at room temperature. And easy removal of filler is also necessary in case of complications (3, 4). Although the ideal filler has not yet been developed, researchers are still searching for fillers that meet these demanding criteria (4).
CATEGORIES OF FILLER
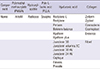
There are several methods for categorizing dermal fillers; we focus on the following three types in this article: natural, synthetic, mixed. Natural materials may be extract preparations of human or animal tissues. Natural material consists of autologous fat and collagen, and the collagen is subdivided into porcine collagen, bovine collagen and human collagen, which are xenogeneic and allogeneic collagens, respectively. Autologous fat is usually extracted from the abdomen or thigh. Autogenous dermofat graft has been used successfully for several decades, while the use of fat injection for body contouring began popular than 30 yr ago. Bioynthetic materials are chemical materials or biologic organic products, such as hyaluronic acid, silicone, calcium hydroxylapatite, polylactic acid, and polyacrylamide gel (4). One of the most commonly used fillers is hyaluronic acid, which consists of linear polymeric dimers of N-acetyl glucosamine and glucuronic acid (5). If the hyaluronic acid fillers are over injected or misinjected, they can be corrected or removed by hyaluronidase immediately (1, 6). Some products, such as Artecoll (Artes Medical, San Diego, California), exhibit special characteristics because of an inner methylmethacrylate covered with a collagen barrier (4). The FDA has approved 22 fillers (Table 1).
INDICATIONS & CONTRAINDICATIONS
Currently, fillers are used in a variety of situations. Their main indications are for the filling of superficial or deep wrinkles as well as correction of congenital or acquired soft tissue depression. Increasingly, fillers are used for volume replacement and enhancement procedures (7), including facial contouring, lower eyelid wrinkle correction, and hand rejuvenation as well as the correction of facial asymmetry and congenital bony and soft-tissue defects (5, 8). Fillers are also used in patients suffering from scleroderma, Romberg's disease, or facial lipodystrophy secondary to immunodeficiency syndrome treatment (9). Another indications are lip augmentation and soft palate augmentation in secondary cleft lip and palate deformity, unilateral paralysis of the vocal cords, correction of anophthalmic orbit syndrome and enophthalmos (8, 10, 11, 12).
By contrast, contraindications to the use of dermal fillers include hypersensitivity to product components, bleeding disorders and a history of severe allergies and anaphylactic shock. Polymethylmethacrylate injection is contraindicated into the mucosa of the lip. Polymethylmethacrylate and poly-L-lactic acid should not be used in patients who are suffered from keloid or hypertrophic scar (13).
FILLER COMPLICATIONS: TREATMENT ALGORITHM
As the number of filler injections increase, the cases of complications also increase. After filler injection, risk of both short-duration and long-duration complications is always existence. While most complications are mild and transient, more severe complications can occur, leaving patients with long lasting, functional and aesthetic problems. Some adverse events occur immediately after filler injection, while others don't. The types of complications according to time of onset are illustrated in Table 2 (5).
Early complications
Swelling, ecchymosis and erythema
Swelling and ecchymosis may develop at the time of injection and they usually resolve spontaneously (14, 15, 16). Cold compression and applying pressure helps to treat the symptoms. Immediately after injection, skin erythema is also transient and normal. If erythema lasts for more than several days, it is likely to be a hypersensitivity reaction. However, it should be differentiated from infection after checking for accompanying fever. Management for erythema with steroids can be useful. Vitamin K cream is also effective in the resolution of reddish swelling (5, 17). Patients with rosacea have a higher risk of developing erythema after injection and should be warned of this fact prior to injecting (5).
Lumps, nodules
Lumps or nodules usually appear to the cystic, edematous or sclerosing types shortly after treatment in the form of well-confined palpable lesions, which can result from injection in areas of thin soft-tissue coverage (e.g. eyelids, nasojugal region, and lip), injection of too much material, clumping of the filler, or dislocation by movement of the muscles (18, 19, 20). The lips are an area of high mobility with thin mucosa. Measures to avoid visibility of the implanted material include firm massage and meticulous placement of filler in the deep supraperiosteal plane (21, 22). Relatively short-term fillers such as hyaluronic acid products are preferable for these high-risk regions. An additional benefit of using hyaluronic acid in these areas is that irregularities can be reversed with hyaluronidase. Semi-permanent fillers, such as poly-L-lactic acid, are longer lasting than hyaluronic acid. However, in cases of overcorrection, irregularity and nodule formations are more persistent and difficult to treat. The management of resulting nodule as the cystic type is a simple puncture (incision and drainage) with a blade or sharp needle. If it is impossible to puncture the lump in the edematous or sclerosing types, a more invasive procedure, such as direct excision will be required or observation may be necessary until the product is absorbed (23, 24, 25, 26). Lumps caused by poly-L-lactic acid or polymethylmethacrylate respond well to intralesional steroid injections, but steroids are less effective for calcium hydroxylapatite (18).
Infection, erythematous nodule
As with any procedure that penetrates the skin, soft-tissue filler injections are also always associated with infection (5). Because chronic inflammation or infection leading to the formation of a granuloma can interfere with the wound healing process, infection control is a significant process (27). Moreover, wound infections are often associated with aesthetically and functionally unfavorable scarring (28). Erythematous nodules, multiple red and tender lumps that persist beyond the first few days of treatment, may be signs of inflammation (14, 19, 21). Additionally, there is a risk for infection with swelling following filler injection. If a single abscess is formed, contamination through the skin likely occurred during injection (29). But, if a patient has multiple abscesses, contamination likely occurred in the syringe before injection. Once a fluctuant abscess is suspected, abscess culture and antibiotics are necessary. However, abscesses should not be treated with antibiotics alone; they should be treated with incision and drainage (I & D) in the absence of cellulitis surrounding tissues. If the abscess is non-fluctuant, we can use antibiotics and steroids as the first line treatment (Fig. 1). In the early stage of treatment, hyaluronidase should not be used because of the risk of spreading the infected material diffusely into the surrounding tissues in the case of active cellulitis (29). If these treatments fail, one should suspect biofilm, methicillin resistant staphylococcus aureus (MRSA) or non-typical tuberculosis (TB) and culture the infected material. In such a case, the patient should be given a TB test and treatments such as with quinolone and a third-generation macrolide, hyaluronidase, 5-fluorouracil (FU) or excision. The infection should be controlled with I & D at first, followed by hyaluronidase if necessary (29). We will discuss the biofilm theory later in this article.
Discoloration, blanching, and necrosis
Vascular-related events are the major, immediate complications that are most likely to result in permanent sequelae. They can occur from intravascular embolism of the injected material, direct needle injury to the vessels, or external compression of the adjacent vasculature secondary to the hydrophilic properties of the product (5). Inadvertent injections of the angular, dorsal nasal or supratrochlear artery are likely to lead to ischemic responses that result in necrosis (15, 22, 30). Localized color changes in the affected areas should increase the index of suspicion about vascular compromise. The pathophysiology of vascular occlusion begins with immediate changes that are visible in the vascular system, including initial blanching, which is followed by mottled discoloration called livedo reticularis. This is accompanied by pain unless there is a nerve block or local anesthetic blocking the pain pathways. The resulting ischemia produces a dusky discoloration that is associated with sluggish or absent capillary refill after digital compression as well as possible loss of function. The final stage of vascular compromise is skin necrosis.
Appropriate treatment should be initiated immediately upon suspicion of vascular compromise. Injection should be stopped, and the area of injection should be massaged immediately as well as warm compresses applied to increase vasodilatation (5, 14, 21). Utilization of nitroglycerine paste and hyaluronidase is also advocated for cases that present early. Other treatments include systemic or topical steroids to reduce the associated inflammation, mitigating the degree of injury. Although aspirin and intravenous (IV) prostaglandins have been suggested, their efficacy has not been proven (31). Other options with unproven efficacy are filler removal via puncture and low-molecular-weight heparin. The aim for treatment is dissolving the product, facilitating blood flow, and promoting vasodilation. Dayan et al. (32) have suggested the use of hyaluronidase in all cases of vascular compromise, independent of the filler type, because of its edema-reducing benefits and theoretical advantage in reducing the occluding vessel pressure. Because of vascular compromise and the resultant necrosis, debridement and wound care are required to minimize scarring. The treatment options are antibiotics and I&D as well as topical wound care, and adipose-derived stem cell injection to boost the healing process and tissue regeneration, which usually takes several weeks for granulation and reepithelialization once an eschar develops. Stem cells are a unique population of undifferentiated biological cells (33). They promote angiogenic processes by secreting angiogenic factors. They also can stimulate cells that helpful in wound healing and differentiate cells that contribute to neovascular formation. However, exact mechanisms are not yet come out into the open (Fig. 2) (34). Many articles on human trials of adipose-derived stem cells are phase I safety trials and case reports (35).
Late complications
Adverse events from fillers can be sorted according to the timing of symptom onset. Fourteen days after the procedure, late complications may occur.
Telangiectasia
Erythema and, occasionally, permanent telangiectasia may occur at the injection site. In cases with erythema, prolonged intralesional or topical steroid therapy should be avoided because they can induce telangiectasia (5). And, in patients with telangiectasia, injection of the filler could worsen their appearance and size. Treatment with intense pulsed light therapy or pulsed dye laser can be helpful (18, 19).
Migration
Migration is thought to result from muscle- or gravity-induced displacement of the filler material (18). When the filler is located too superficially or in mobile anatomic areas, such as lips or lid area, sometimes migration can occur. This complication is strongly associated with injection of calcium hydroxylapatite into the lip. While speaking or eating and so on, the superficial and deep portion of the orbicularis oris muscle acts as a pump, which makes the material coalesce and results in nodule formation (26). To mechanically break up the product, intralesional steroid injections with massage should be performed. Alternatively, the nodular formation site can be opened with a needle for removal of the product. As an optional treatment, surgical removal is also considered (36).
Hypertrophic scar
Superficial placement of fillers may be associated with hypertrophic scarring. Superficial placement of fillers rarely resolves with permanent scar, consisting mainly of extracellular matrix components such as collagen, fibroblasts, and small vessels (37). For softening the hypertrophic scar, a pulsed dye laser or intralesional steroids are helpful. After this treatment, if there is no improvement, scar revision can be considered.
Granuloma and biofilm
The enveloped filler material may resist degradation and remain sequestered in the macrophages. These macrophages secrete various cytokines and other inflammatory materials that attract other macrophages and blood monocytes. Each macrophage may increase in size (epithelioid histiocytes) or fuse to form multinucleated foreign body giant cells. During this process, granuloma is formed (5). The reported rate of granuloma formation is 0.01% to 1% (18, 38). Granulomas can occur with all soft-tissue fillers, regardless of type, and usually appear after a latent period, which can be several months to years after filler injection (5). Nodule and granuloma are different in terms. Pathological diagnosis is not available, we can use nodule as a descriptive term. However, the latter term should only be used when the required pathological criteria for granulomas have been satisfied (29).
First treatment of choice for this complication is massage and intralesional corticosteroids. Granulomatous reactions after hyaluronic acid injection can be cured with hyaluronidase (39). Patients who are not responsive to steroid alone can respond to the combination treatment of 5-FU and corticosteroids, discouraging additional fibroblast activity and fibrosis. In the event of repeated failure of aforementioned therapies, surgical removal should be considered (5, 40). If these treatments fail, a biofilm is likely, consisting of MRSA or non-typical TB and culture of the infected material, TB test and treatments such as 2-drug with a quinolone and third-generation macrolide, hyaluronidase, 5-FU or excision should be performed.
Recently, there has been discussion on the role of biofilms in causing delayed nodule formation, and it has not been precisely proven that biofilms are involved in granuloma formation. However, many articles present arguments in favor of this hypothesis (16, 29, 41). Biofilms are accumulations of microorganisms within a self-developed matrix; they are irreversibly adherent to one another and to a variety of surfaces (42). In the biofilm, bacteria can safely avoid from immune defenses, so antibiotics have no effect. (29) Hyaluronidase helps break down the matrix, decreasing the biofilm mass (43). Other treatment options for biofilms are the prolonged use of antibiotics, administration of intralesional 5-FU and intralesional laser therapy with a 532-nm or 808-nm laser (44). With respect to antimicrobials, 2-drug therapy with a quinolone and a third-generation macrolide is recommended (16, 44).
Skin defects
There might be skin loss, scarring, and asymmetry, resulting in skin defects in spite of active treatment after skin necrosis. In cases with skin defects, various reconstruction treatment options can be used for the aesthetically and externally competent results. The primary usable methods of reconstruction are a full thickness skin graft (FTSG), local flap, composite graft and cartilage graft. A FTSG usually involves performing a skin graft using donor tissue from behind the ear, and composite and cartilage grafts are also applied by the conchal cartilage of the ear, which is harvested according to the size of the defect. It is advantageous that the scar from the donor site is invisible because it is usually harvested from ear, and the recipient site can achieve symmetry by supplying the site of skin loss defect (Fig. 3). And, in the case of a small defect, primary closure or local flaps are the best treatment of choice because they can offer similar skin color and texture like surrounding tissue (45).
From these results, we constructed a treatment algorithm that incorporates our case and related articles (Fig. 4).
PREVENTIVE METHOD FOR FILLER INJECTION
Although proper treatment for complications is important, the prevention of the complications is crucial. The selection of appropriate injection techniques is important because it can help successful outcomes and reduce the risk of complications (36). First, strategy for reducing the risk of infection is thorough cleansing of the injection site. We should not inject the hydrophilic permanent filler materials through oral or nasal mucosa and not inject into the previous filler site or traumatized tissue (5).
There are several injection techniques that are associated with an increased risk of adverse events. Increasing the dissection of the subepidermal plane (i.e., a fan-like injection pattern), rapid injection, rapid flow rates, and higher volumes are included. (36). Specially, if a large volume bolus injection was administered, blood circulation defects could occur, which require attention. Large volume injections should only be performed when administered above the bone or into the dermis (5). Other precautions include aspiration before injection and delivery of material at different points (21, 23). Some have advocated the use of small-caliber needles because they slow the speed of injection. The use of blunt needles is another method of reducing complications. After filler injection, exposure to high and low temperatures should be avoided. For one day, filler recipients should avoid touching or pressing on the site of the surgical procedure and avoid contacting water to prevent inflammation. For almost 1 week, drinking alcohol and smoking should be avoided.
CONCLUSION
Filler injection for soft tissue augmentation is a satisfactory procedure with very modest results in spite of high expectations. However, as the number of indications and performance increases, the number of complications also increases. It is important for the physicians to know facial anatomy and high-risk regions. The experts of filler injection must be familiar with each filler material, the injection techniques, and the potential complications. If a complication does occur, the treatment algorithms of this article will be helpful for facilitating minimization of long-term sequelae. We summarized the key information about fillers and their complications, which can help clinicians, allowing them to successfully avoid and efficiently treat potential adverse events.



 XML Download
XML Download