

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
WHO has reported ischemic heart disease and stroke as the first and second leading causes of death worldwide, accounting for 21.8% of all deaths (1). The mortality rate for these two causes has increased over the past decade (1). Hypertension is one of the main risk factors for cardiovascular disease and cerebrovascular disease (2). Obesity, diabetes, old age, low potassium intake, and high salt intake are the known risk factors for incident hypertension (3). High salt intake has been reported as a cause of hypertension in many studies, and also in animal and epidemiological studies (4, 5, 6). Therefore, reducing the salt intake is very important for human health as it decreases the prevalence of hypertension. To reduce the salt intake, we should know our salt intake. The salt intake can be checked by two methods: remembering the food items consumed over the previous 24 hr and then calculating the salt intake, and calculating the salt intake based on the sodium excreted in the urine, which is more accurate than the 24-hr recall method. Therefore, the 24-hr urine sodium level is the 'gold standard' method for estimating the salt intake. However, the 24-hr urine test is too cumbersome to administer. The urine collected can be easily lost from the bag, and it is also inconvenient to carry around a bag of urine all day. The result of urine collection can be different between weekdays and weekend. People may be considered to be sick when they collect urine in their office. Research has therefore been focused on estimating the salt intake using the spot urine test (7, 8). However, no study has reported the method for estimating the salt intake of Koreans using the spot urine test. Therefore, the present study aimed to estimate the 24-hr urine sodium excretion level by measuring the spot urine sodium and creatinine levels, and to validate the efficacy of the formula for determining the status of low salt intake<100 mEq Na/day in Koreans.
MATERIALS AND METHODS
Population
All data were collected retrospectively by accessing the electrical medical records of Seoul National University Hospital. Among 1,363 outpatients whose serum creatinine and 24-hr urinary sodium were measured when they visited the outpatient clinic, the 24-hr urine samples were collected from 400 outpatients based on the following inclusion criteria: we defined appropriate urine collection as the ratio of measured 24-hr urinary creatinine to estimated 24-hr urinary creatinine of 0.75-1.25, and patients with ratio in this range were included. Also, we excluded patients who had been prescribed diuretics or fluid therapy, which may influence the 24-hr urinary sodium excretion.
Analysis method
The 24-hr urine creatinine level was estimated based on the spot random urine creatinine. We estimated the 24-hr urine creatinine level by using the following three equations: the Tanaka equation (8), E24UCR_T: 24-hr urine creatinine level (mg)=-2.04×age (yr)+14.89×body weight (kg)+16.14×height (cm)-2244.45; the Cockcroft-Gault (CG) equation (11), E24UCR_CG: 24-hr urine creatinine level (mg)={8-[0.2×age (yr)]}×weight (kg), (if women,×0.85); and the Korean equation, (E24UCR_K) which we formulated based on the age, weight, and height by the linear regression model used by Tanaka (8).
These three equations were derived from the estimated 24-hr urine creatinine and the ratio of spot urine sodium and creatinine by the method reported by Tanaka (8).
Statistics
We calculated the correlation coefficients between the estimated and measured values for 24-hr urine creatinine and sodium and fitted the two variables by linear regression analysis. We used the Bland-Altman method to measure agreement between the measured and estimated values. To estimate the precision rate of estimated values, we calculated the interquartile range (IQR); and to estimate the accuracy, we calculated the proportion of estimates within 30% deviation of measured sodium (P30) and Root Mean Square Error (RMSE). We also calculated the sensitivity, specificity, and probability of area under curve (AUC) with a receiver operating characteristic (ROC) to predict 24-hr urine sodium>100 mEq/day by using the estimated values. Statistical analyses were performed with SPSS version 20.0 for Windows (SPSS Inc., Chicago, IL, USA). Two-sided P values were used for all statistical analyses. A P value<0.05 was considered statistically significant.
RESULTS
Study participants and their baseline characteristics
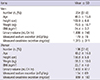
The study group comprised 204 men and 196 women (age 48.5±15.8 yr, 49.2±14.0 yr, respectively). The mean urine volume per day was 1,886±748 mL in men and 1,693±617 mL in women. The measured sodium excretion per day was 179±78 mEq in men and 154±69 mEq in women. The measured creatinine excretion per day was 1,315±311 mg in men and 889±183 in women (Table 1).
The E24UCR_K equation for estimating the 24-hr urine creatinine level
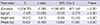
Using a linear regression model for age, weight, and height, we derived an equation to estimate the 24-hr urine creatinine, E24UCR_K=-7.428×age (yr)+10.372×weight (kg)+15.631×height (cm)-1,234.785 (P<0.001) (Table 2).
The correlation between the measured and estimated 24-hr urine creatinine levels
There was an association between the measured and estimated 24-hr urine creatinine levels using all three equations. The correlation coefficient was 0.846 by E24UCR_T, 0.896 by E24UCR_CG, and 0.863 by E24UCR_K (P<0.001) (Fig. 1).
The correlation between the measured and estimated 24-hr urine sodium levels
The three derived formulas to estimate 24-hr urine sodium level were as follows: E24UNA_T=21.98×XNA0.392, E24UNA_CG=33.409×XNA0.347, and E24UNA_K=28.985×XNA0.346. XNA was calculated as follows: XNA={spot urine sodium (mEq/L)/[10×spot urine creatinine (mg/dL)]} x estimated 24-hr urine creatinine level by each equation. There was an association between the measured and estimated 24-hr urine sodium levels using the three equations The correlation coefficient was 0.490 by E24UCR_T, 0.516 by E24UCR_CG, and 0.466 by E24UCR_K (P<0.001) (Fig. 2).
Validation of the adequacy of the estimated 24-hr urine sodium compared with the measured 24-hr urine sodium level
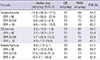
The median value for the difference between the measured and estimated 24-hr urine sodium levels was -12.4 mEq/day by E24UCR_T, 3.3 mEq/day by E24UCR_CG, and 9.8 mEq/day by E24UCR_K. The preciseness expressed as IQR, RMSE, and P30 was similar among the three equations (Table 3). In the Bland-Altman plot, the probability that the difference between the measured and estimated values existed within -1.96 SD and+1.96 SD of the mean value was 95.0% (380/400) in E24UCR_T, 95.5% (382/400) in E24UCR_CG, and 94.5% (378/400) in E24UCR_K (Fig. 3).
The prediction of measured 24-hr urine sodium level, >100 mEq/day, with the estimated 24-hr urine sodium level, >100 mEq/day
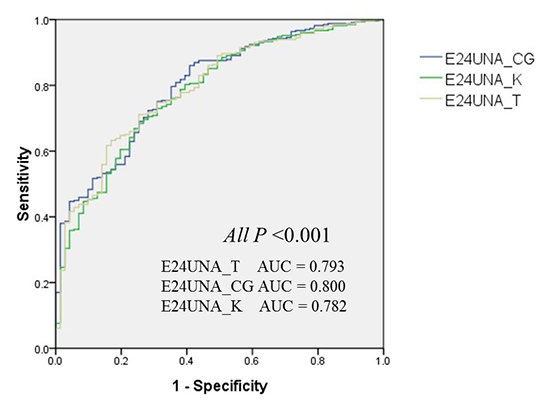
The sensitivity of formulas to estimate the measured 24-hr urine sodium≥100 mEq/day with the estimated amount≥100 mEq/day was 87.6% for E24UNA_T, 84.8% for E24UNA_CG, and 84.3% for E24UNA_K. However, the specificity was the highest for E24UNA_CG (Table 4). The AUC calculated by using the ROC curve was 0.793 in E24UNA_T, 0.800 in E24UNA_CG, and 0.782 in E24UNA_K (All P<0.001) (Fig. 4).
DISCUSSION
In order to estimate the amount of 24-hr urine sodium using the spot urine test, some assumptions are necessary. First, 24-hr urine specimen was collected without omission and the factors that may affect sodium excretion were excluded. Second, the actual amount of creatinine in the urine collected for 24 hr was equal to the estimated creatinine excretion from age and body weight. Third, the 24-hr urinary sodium to 24-hr creatinine ratio and the spot urine sodium to spot urine creatinine ratio are constant. Each assumption has to be considered.
According to the first assumption, the 24-hr urine collection method is useful to determine the precise sodium intake, but it is difficult to collect urine without any loss of urine (12). To date, most of the studies of sodium intake in Korea have used the 24-hr recall method for measuring the sodium intake. Only a few studies have used the 24-hr urine collection method, in which there was no mention about the accuracy of urine collection (13). In our study, we excluded the patients who had been prescribed diuretics and fluid therapy, which could have an effect on sodium excretion. Also, we compared the 24-hr urine creatinine estimated by the Cockcroft-Gault equation with the actual 24-hr urine creatinine level. In order to increase the accuracy, we selected the value of 24-hr urine collection, in which the ratio of measured value to estimated value was within 0.75-1.25. But, there are some issues in our study. The study subjects were patients who visited the tertiary hospital, and we did not check the amount of sodium in their diet, exercise, and urine collection time, which could have an effect on sodium excretion. To generalize the equation, along with addressing these issues, there must be an effort to collect urine completely by using the method of para-amino benzoic acid recovery as in the other survey (14).
Second, the actual 24-hr urine creatinine in the urine collected was equal to the 24-hr urine creatinine estimated. Creatinine is the end product of creatine metabolism in the muscle and is excreted through the kidneys. The urine creatinine excretion is proportional to the muscle mass of the subject and is almost unaffected by the diet. Therefore, the amount of urine creatinine was used for precise judgment of urine collection (15). But, the difference between the estimated value provided by the Cockcroft-Gault equation and the actual value in the urine collected was already known. This difference originated from the difference in the physique of species and/or urine creatinine excretion per kg. To date, the Cockcroft-Gault equation is widely used after the correction, but there seem to be some problems in applying it to the general Korean population (16). In our study, we used two formulas for estimating creatinine excretion along with the Cockcroft-Gault equation. There was no difference in the accuracy of the three equations. The production of creatinine in the body is influenced by the muscle mass and dietary habits. When there is a decrease in the muscle mass and/or an increase in the age, there is a decrease in the production of creatinine. When people have a high protein diet, the production of creatinine is increased. Also, drugs such as trimethoprim, cimetidine can block proximal tubular creatinine excretion. Antibiotics can have an effect on the microflora in the colon in which the excretion of creatinine is affected, and then the creatinine level is increased (17). In our study, we excluded the factors that can have effect on sodium excretion, but we could not control the factors that can have an effect on creatinine excretion.
Third, the 24-hr urinary sodium to 24-hr creatinine ratio and the spot urine sodium to spot urine creatinine ratio are constant. Usually, urine creatinine excretion is proportional to the muscle mass of the subject and is almost unaffected by the diet; therefore, the characteristics of creatinine support this assumption. But, this may not be true for sodium. The velocity of excretion of sodium per day is not constant, and it can change according to the position, exercise, diet, and hemodynamic factors (18). Also, it is impossible to measure the amount of extrarenal excretion such as that in stools and sweat, and therefore, we could not derive the formula without this assumption. Also, the amount excretion of sodium can be different according to the glomerular filtration rate. Therefore, we could increase the accuracy by stratifying according to the glomerular filtration rate when comparing the estimated value and the actual value.
WHO recommends a daily salt intake of less than 5 grams (sodium 2,000 mg). But no study has examined the usefulness of the formula for estimating the sodium level proposed in this guideline. In this study, we compared the estimated and measured sodium intake based on 100 mEq/L of sodium (2,300 mg) and assessed the equations using the AUC values. According to the results, E24UNA_CG showed the highest accuracy, and both E24UNA_T and E24UNA_K also showed significant accuracy. Thus, all of the three formulas can be used in accordance with the standard recommended guideline and also as an indicator of the current salt intake for determining the appropriate low salt diet.
There may be some limitations to this study because of lack of strict control of factors that have an effect on sodium excretion and the retrospective study design. In the future, a prospective study is needed to prove the usefulness of these derived equations.
In conclusion, E24UNA_K, E24UNA_CG, and E24UNA_T formulas, which were derived from sodium concentrations in spot urine, are useful for predicting 24-hr sodium intake and there is no difference among the formulas for predicting sodium over intake.




 XML Download
XML Download