

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Spirometry is required to make diagnosis of chronic obstructive pulmonary disease (COPD). The Global Initiative for Chronic Obstructive Lung Disease (GOLD) report had recommended staging system based on airflow limitation as measured by spirometry. However, the impact of COPD on an individual patient does not depend on the degree of airflow limitation only. Airflow limitation is weakly correlated with symptoms and impairment of patient's health related quality of life (1). Airflow limitation alone is not predictive of dyspnea, quality of life and exacerbation frequency (2).
As the goals of assessment for a chronic disease are to determine the severity of disease, its impact on the patient's health status and the risk of future event in order to guide therapy, the GOLD consensus report proposed a new classification for COPD in 2011 to more comprehensively assess disease severity. This new classification system combined the symptoms in addition to COPD exacerbation history and airflow limitation measured by FEV1. The modified Medical Research Council (mMRC) questionnaire or COPD Assessment Test (CAT) is recommended for assessing symptoms (3). The GOLD 2011 classification stratifies first on the basis of symptoms with either dyspnea (mMRC 0-1 or≥2) or health status (CAT<10 or ≥10) score resulting in two low-symptom categories (A and C) and two high symptom categories (B and D). Further, exacerbation risk is assessed with either airflow limitation measured by FEV1% predicted (<50% or ≥50%), or COPD exacerbation history (0-1 or ≥2) in the previous year to stratify patients into low-risk categories (A and B) versus high-risk (C and D) categories (Fig. 1). There were several studies evaluating this new GOLD assessment system (4, 5, 6, 7). The new GOLD assessment system showed uneven distribution of COPD patients and limited data on the clinical outcomes.
In Korea, a revised COPD guideline was released in 2012 by the Korean Academy of Tuberculosis and Respiratory diseases (8). The new Korean COPD guideline also emphasized the combined assessment for COPD patients. However, there were some differences present between the Korean guideline and GOLD consensus report. The Korean guideline classified the COPD patients into 3 groups. The Korean guideline combined GOLD C, D group into one group and used different the spirometry cut-off value for the high risk of exacerbation from that of GOLD report. The Korean COPD guideline stratified first on the basis of risk of exacerbation with either FEV1 (<60% or ≥60%) or exacerbation history (0-1 vs. ≥2) in the previous year resulting in low risk or high risk group (group 'da'). The low risk group then stratified with mMRC or CAT like in GOLD report resulting in low symptom (group 'ga') or high symptom (group 'na') group (Fig. 1).
The purpose of this study was to compare the Korean COPD guideline to GOLD report in terms of acute exacerbation.
MATERIALS AND METHODS
Study design and patients
The patients included in the present study were from the Korean COPD Subtype Study (KOCOSS) cohort. The patients were recruited from 28 referral hospitals in Korea. Patients were eligible if they were age ≥40 yr, postbronchodilator FEV1/FVC <0.7 and presence of respiratory symptoms such as cough, sputum, or dyspnea. Patients with any respiratory diseases mimicking COPD such as bronchiectasis, asthma, and the tuberculosis-destroyed lung were excluded. Patients included in this analysis were part of the patient dataset obtained on May 10, 2013.
Procedures
All patients underwent clinical examination and spirometry. We used self-administered questionnaires to record demographic and medical history data. Symptoms were asked with mMRC questionnaire, CAT and the St George's Respiratory Questionnaire for COPD (SGRQ-C). Data about exacerbation history in the previous year were gathered at baseline. Prospective exacerbation data were gathered through a longitudinal follow-up protocol done every 6 months. Prospective exacerbation data were analyzed for all patients with COPD where longitudinal follow-up datawere available. The definition of exacerbation used in this study was that worsening of one of the respiratory symptoms, such as increase in sputum volume, increase in sputum purulence or increase in dyspnea which required treatment with systemic corticosteroids or antibiotics, or both. As the length of follow-up varied on the basis of time of enrollment, May 10, 2013 was used as the cut-offdate for available longitudinal data.We determined the distribution of COPD patients by the GOLD consensus report or Korean COPD guideline.We also compared the experience of exacerbation during follow-up according to the two classification systems.
Statistical analyses
All data were presented as mean (±SD) where appropriate. Analyses were done with SPSS (version 16.0) for Windows. We performed descriptive analyses to assess differences in baseline characteristics. We used chi-square test and Fisher's exact test for categorical variables and Kruskal-Wallis test for continuous variables. All P values were two-sided, and values<0.05 were considered statistically significant.
RESULTS
Baseline characteristics
A total 361 patients were enrolled in this study. Male comprised of 89.8% of the cohort. Mean age of the patients was 68.5 yr and mean follow-up duration was 22.8 months. The mean FEV1 were 1.43 L and 52.7% of the predicted value. The distribution of the spirometry classification was as followed; 7.2% in GOLD1, 47.9% in GOLD2, 35.5% in GOLD3 and 9.4% in GOLD4, respectively. The mean total CAT score was 15.9. A total 43.2% of the patients responded their mMRC ≥2 (Table 1).
Distribution of patients according to each classification system
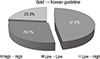
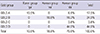
After applying Korean COPD guideline, 70.9% of the patients were re-classified into Korean group 'da'. A total 10.5% and 18.6% of the patients were in Korean group 'ga' and 'na', respectively. The distribution of 2011 GOLD classification system was followed; 17.5% in GOLD A, 34.9% in GOLD B, 3.6% in GOLD C and 44.0% in GOLD D. The Korean COPD guideline used different FEV1 cut-off values for high risk of exacerbation from that of GOLD report. We also evaluated the reassignment of the two COPD classification systems. Among the patients in GOLD A and B, 39.7% and 46.8% of the patients were reassigned into group 'da' of Korean COPD classification (Table 2). Therefore, 23.3% of all patients have been changed their risk group from low risk group to high risk group after applying Korean system (Fig. 2).
Experience of acute exacerbation
A total 16.9% of the patients experienced acute exacerbation during the follow-up. The proportion of patients who experienced exacerbation at 6 and 12 months of follow-up were 9.7% and 12.2%, respectively, which meant 72.1% of exacerbated patients had experienced their exacerbation during the first year of follow-up. The mean number of acute exacerbation of the patients who experienced exacerbation was 2.75 (range 1-11).
A total 16% of Korean group 'da' patients experienced exacerbation during the first year of follow-up. However, none of Korean group 'ga' patients experienced had exacerbation and 4.5% of Koran group 'na' patients experienced exacerbation during the same period. The first year exacerbation rate was 6.3% for GOLD A, 9.5% for GOLD B, 7.7% for GOLD C and 17% for GOLD D, respectively (P=0.09) (Fig. 3). During the follow-up period, 14.3% of patients reassigned into GOLD A experienced exacerbation. A total 13.5% of patients with GOLD B, 23.1% of GOLD C and 20.1% of GOLD D experienced exacerbation. This figure was not statistically significant. The proportions of the patients who experienced exacerbation during the same period according to the Korean COPD classification were 7.9% in Korean group 'ga', 6.0% in Korean group 'na', and 21.1% in Korean group 'da', respectively (P=0.004).
Comparison of acute exacerbation between the two classification systems
As mentioned above, 23.3% of the patients were changed in their risk groups. We explored the experience of exacerbation in patients with change of their risk group after applying Korean COPD guideline. During the first year of follow-up, 16.0% of the patient who were reclassified from GOLD A to Korean group 'da' experienced acute exacerbation. And 15.3% of patients from GOLD B to Korean group 'da' experienced acute exacerbation. A total 7.7% of patients from GOLD C to Korean group 'da' and 17.0% of patient from GOLD D to Korean group 'da' had exacerbation during follow-up period, respectively (Fig. 4).
DISCUSSION
Prevention of acute exacerbation is one of the COPD treatment goals (3). The 2011 updated GOLD report applied the symptoms and exacerbation history in addition to spirometry classification for better assessment and individualized treatment for COPD patients. GOLD report used the 50% of FEV1 of predicted value to differentiate the high and low risk for exacerbation in terms of spirometry. GOLD report recommends the pharmacological treatment according to the combined assessment system (GOLD A-D). Unfortunately, the recommended treatment for GOLD C and D (high risk patients) is almost same for each group. And the proportion of GOLD C group was very small in the previous reports (9). Regular treatment with inhaled corticosteroids (ICS) in addition to bronchodilators is effective in COPD patients with an FEV1<60% predicted (10, 11, 12). However, the GOLD report recommended ICS combined with long acting beta2-agonist for the patients group C and D, which means for the patents with FEV1<50% predicted. The Korean Academy of Tuberculosis and Respiratory Disease (KATRD) revised COPD treatment guideline in 2012. Korean guideline simplified the COPD grading system. Korean guideline used 3 grading system and an FEV1 of 60% to differentiate high and low risk of exacerbation. Korean COPD guideline also recommends the pharmacologic treatment according to the assessment systems. Korean guideline is simple to apply to real world practice than GOLD report. However, there was no study to evaluate the usefulness of Korean COPD guideline, which simplified the assessment system compared to GOLD report.
In this study, a total 16.9% of the patients experienced the acute exacerbation rate of the during the mean 22.4 months follow-up duration. And the proportion of patients who experienced exacerbation at 12 months of follow-up was 12.2%. The proportions of the patients who experienced exacerbation during the first year of follow-up in each Korean classification system were 0% in Korean group 'ga', 4.5% in group 'na', and 16.0% in group 'da', respectively (P=0.002). On the other hand, 6.3% of patients in GOLD A, 9.5% in GOLD B, 7.7% in GOLD C and 17.0% of GOLD D experienced exacerbation during the first year of follow-up (P=0.09). As only 3.6% of the patients were reassigned in GOLD C, we compared the exacerbation between the GOLD C&D as a whole and Korean group 'ga'. A total 16.3% of patients in GOLD C&D and 16.0% of patients in Korean group 'da' experienced the exacerbation during the first year of follow-up, respectively. As the spirometry cut-point for was different between the two COPD classification system, 39.7% of GOLD A and 46.8% of GOLD B patients were reassigned into Korean Group 'da'. The proportions of the patients who experienced exacerbation during the first year of follow-up in these two subgroups were 16.0% and 15.3%, respectively. This suggested that there are many patients who experienced exacerbation with FEV1 between 50% and 60% predicted. The value of an FEV1 60% predicted is more useful to differentiate the exacerbation in terms of spirometry.
The 2011 GOLD report divided COPD patients into 4 groups and recommended inhaled corticosteroid for GOLD C and D patients. However, only small proportion of the patients were reassigned into GOLD C (4, 5, 6, 7), encompassing a rare mixture of patients with severe airflow limitation but no or little symptoms. Regular treatment with ICS is known to improve symptoms, lung function and quality of life and reduce the frequency of exacerbation in patients with an FEV1<60% predicted (10, 11, 12). So, there has been a discrepancy between the guideline and real world practice. As the spirometry classification of COPD in the initial GOLD report was for the educational reasons the cut-points was not validated (1). The revised Korean COPD guideline was developed to overcome these problems in GOLD report. This study demonstrated the usefulness of 60% of FEV1 predicted as a cut-point for differentiation of high and low risk of exacerbation. We think that this study can give rationale for the early treatment with ICS to prevent exacerbation to patient with moderate airflow limitation. As COPD patients susceptible to exacerbation were stable over 3-yr period (2) and the exacerbation is the most important determinant of frequent exacerbation, early treatment with such as ICS is important for COPD patients.
This study had some limitations. It is not population-based study and cannot represent the COPD severity in the general population (13). However, this study could give the real world information about currently treated COPD patients, because participating institutes of this study could cover almost Korea. As the different use of cut-off point in Korea COPD guideline was to differentiate the risk of exacerbation, we did not evaluate other important parameters, such as quality of life, improvement pulmonary function, etc. These parameters will be explored in near the future as the KOCOSS is currently ongoing study.
In summary, we showed that 60% of FEV1 predicted was useful to differentiate between the high risk and low risk for exacerbation in terms of spirometry. This indicates that Korean COPD guideline is more appropriate to apply to Korean COPD patients. Physicians make continuous efforts to update the Korean guideline to improve treatment of COPD.




 XML Download
XML Download