

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anti-tumor necrosis factor alpha (TNFα) is often used in patients with rheumatic disease who do not respond to conventional treatments, such as non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroid, or disease modifying anti-rheumatic drugs (DMARDs) (1, 2). Dramatic improvements have been shown in clinical symptoms and signs in patients with ankylosing spondylitis (AS) receiving anti-TNFα. However, anti-TNFα has a number of rare but serious adverse effects, including infection, tuberculosis (TB), increased risk of certain malignancies, congestive heart failure and drug-induced lupus (3, 4). Among these, latent tuberculosis infection (LTBI) or new TB are of the most particular concern in Korea. The degree of concern for LTBI differs by country and its frequency of TB. Hence, the standard for TB surveillance may be different before and after treatment. Physicians should be aware of TB, especially in patients receiving anti-TNFα or other biologic agents because the incidence rate of TB in Korea is considerably high (5). In addition, AS patients have higher risk of TB than the general population (6).
In the 2012 update of the American College of Rheumatology (ACR) recommendation, annual LTBI testing is suggested in rheumatoid arthritis (RA) patients taking anti-TNFα who live in situations where TB exposure is likely (1). Therefore, follow-up LTBI testing also seems to be important in AS patients receiving anti-TNFα. Because of the increasing use of anti-TNFα in AS patients, a well-established guideline concerning follow-up LTBI testing needs to be generated. Park et al. (7) reported that the tuberculin skin test (TST) conversion rate is significantly higher in the AS than in the RA patients. However, the TST may not be the appropriate value of measurement to employ because prior Bacillus Calmette-Guerin (BCG) vaccination can produce false-positive results. Recently, Kim et al. (8) showed that AS patients have an independent association with discordant IGRA-negative/TST-positive results. In contrast to the TST, because IGRA is unaffected by BCG vaccination status. In addition, TST testing has a boosting effect, which could lead to conversion in repeated testing, whereas IGRA does not exhibit such testing error. Hence, IGRA may serve as an appropriate guideline measurement (9, 10). However, follow-up IGRA testing in AS patients receiving anti-TNFα has rarely been studied. Moreover, there are no country-specific guidelines for IGRA testing.
In the present study, we assessed the pattern of serial IGRA results in AS patients receiving anti-TNFα in Korea with intermediate TB burden, and analyzed the characteristics of AS and RA patients.
MATERIALS AND METHODS
Study population
The study participants were enrolled from September 2008 to August 2012, among AS patients who were registered with the outpatient clinic of Hanyang University Hospital for Rheumatic Diseases in Seoul. A total of 127 patients with AS started to receive anti-TNFα (etanercept, adalimumab, and infliximab) during this period, and had negative initial IGRA result and follow-up testing. These patients were evaluated by follow-up IGRAs until November 2013. The patients were of Korean nationality, and met the 1984 New York criteria for AS (11). We reviewed data from the subjects according to age, gender, TB prophylaxis, concomitant treatment (methotrexate, steroid), IGRA conversion and anti-TNFα, including type, and treatment duration. No patient had a prior history of active TB.
To compare the characteristics of AS and RA patients, we also reviewed 26 RA patients in the same study design. All the RA patients met the American College of Rheumatology 1987 classification criteria for RA (12).
The interferon-gamma release assay
From September 2008, the QuantiFERON-TB Gold In-Tube test (QFT-GIT) as IGRA had applied to the LTBI screening. Therefore the QFT-GIT was performed in all patients before initiating anti-TNFα and for follow-up testing, according to the manufacturer's instructions (Cellistics Limited, Carnegie, Victoria, Australia). Interferon-gamma concentration≥0.35 IU/mL, and ≥25% of the negative control were interpreted as positive. Conversion of QFT-GIT was defined as negative QFT-GIT at baseline and positive QFT-GIT at follow-up. We excluded the indeterminate QFT-GIT results from our study.
Statistical analysis
We analyzed patient characteristics and IGRA conversion rates using multivariable logistic regression analysis adjusted for age, sex, LTBI prophylaxis, concomitant use of methotrexate and steroid, and treatment duration of anti-TNFα. We compared the characteristics of AS and RA patients using the Wilcoxon rank sum test for quantitative variables and the chi-square test for qualitative variables. Results are presented as means±SDs unless specified otherwise. When P values were less than 0.05, results were considered statistically significant. All statistical analyses were performed using SPSS (version 18.0, Inc., Chicago, IL, USA).
RESULTS
Patient characteristics and IGRA conversion result
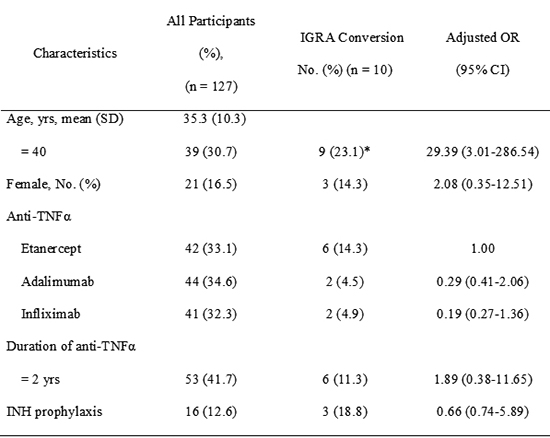
The 127 AS patients were enrolled in the study. The mean age was 35.3±10.3 yr. There were 106 (83.5%) male and 21 (16.5%) female patients. The median duration of anti-TNFα was 22.6±11.4 months. Forty two patients received etanercept, 44 received adalimumab, and 41 received infliximab (Table 1).
Among the 127 AS patients, IGRA conversion was found in 10 patients (7.9%). There was no significant variation between IGRA conversion rate and any risk factors except for age. Type of anti-TNFα was not associated with IGRA conversion rate. The IGRA conversion rate was higher in older patients (≥40 yr) (9/39, 23.1%) than in younger patients (<40 yr) (1/88, 1.1%) (P<0.05). Table 2 shows the characteristics of AS patients with IGRA conversion. In spite of isoniazid (INH) prophylaxis, three patients among 16 AS patients with INH prophylaxis had positive IGRA conversion result. However, no patient among the 127 AS patients has developed TB.
Comparison results of IGRA between AS and RA
As shown in Table 3, the mean age of RA patients was 54.3±16.4 yr. RA patients were older than AS patients. While 83.5% of AS patients were male, only 7.7% of RA patients were male. The median duration of anti-TNFα showed no difference between AS and RA. Type of anti-TNFα was not different between RA and AS. RA patients used methotrexate and steroids more often than AS patients. Among the 26 RA patients, positive conversion was found in 5 patients (19.2%). The IGRA conversion rate was not significantly different between AS and RA patients (P=0.12).
DISCUSSION
AS patients undergoing anti-TNFα in Korea have an ongoing risk of TB because they have a higher risk of reactivation of LTBI or contracting new TB than patients in low TB-burden areas do. This is because Korea is an intermediate TB burden area, posing a greater risk for TB exposure (6), which in turn leads to an increased risk of new TB infection. As a result, the number of infected patients who cannot be diagnosed through IGRA may become higher than that of developed countries. Chen et al. (13) reported that development of active tuberculosis presented persistently high interferon gamma level or IGRA conversion in RA patients receiving anti-TNFα. Therefore, interferon gamma (IFNγ) level and serial IGRA testing may be useful for the control of TB in patients receiving anti-TNFα (1). We assessed the utility of a follow-up IGRA in AS patients who were receiving anti-TNFα. Age was the only risk factor that seemed to influence the IGRA conversion rate. Therefore, a follow-up IGRA test may be more useful for elderly AS patients receiving anti-TNFα.
There is no gold standard for the diagnosis of LTBI. A TST, QFT-GIT, or T-SPOT TB (Oxford Immunotec, Abingdon, UK) are frequently used for LTBI screening (14, 15). The TST represents delayed type hypersensitivity reaction in the skin to intradermal injection of PPD. QFT-GIT detects secretory INFγ in response to TB-specific antigens (EAST-6, CFP-10, and TB7.7). T-SPOT TB uses ESAT-6 and CFP-10 as TB-specific antigens. Previous study showed the TST conversion rate was significantly higher in the AS (50%) than in the RA (17.5%) patients (7). Kim et al. (16) reported that eight patients among 26 AS patients treated with immunosuppressive agents or anti-TNFα had positive IGRA conversion (8/26, 30.8%). However, in our study, IGRA conversion rate in AS patients undergoing anti-TNFα were 7.9%, and IGRA conversion rate had no statistical difference between AS and RA.
In Korea, the BCG vaccination is given at birth. Until 1996, Korean children underwent a second TST at the age of 12 or 13 yr. Any child who had negative TST results received a second BCG vaccination. AS patients are relatively younger than those with other rheumatic diseases. Thus, relatively young AS patients might be more affected than RA patients by previous BCG vaccination. Recently, Kim et al. (8) showed that AS patients had association of discordant QFT-GIT-negative/TST-positive. With respect to AS, IGRA has several advantages for monitoring of LTBI. IGRA is not affected by BCG (9, 10). Second, patients do not need to visit the clinic once more. AS patients find it difficult to make a return visit for TST interpretation 72 hr later. There is also subjective variability in the interpretation of TST results (17).
Our study has some limitations. We usually start LTBI treatment before anti-TNFα following a positive LTBI screening result (1, 18). However, there is no strong evidence showing that LTBI treatment is needed in AS patients receiving anti-TNFα if they have an IGRA conversion result. We retrospectively analyzed the IGRA conversion rate. The duration of follow-up testing was quite long (22.6±11.4 months), therefore we do not know exactly when IGRA conversion occurred. Although the duration of anti-TNFα was not associated with IGRA conversion rates in our study, in a recent article, LTBI reactivation probably occurred during the first 6 months after starting anti-TNFα (13). However, in this study 9 of 10 patients with IGRA conversion had follow-up testing after 1 yr. If newly activated TB was detected in a follow-up IGRA, it would be necessary to prescribe the anti-TB medication (quadruple therapy) instead of INH prophylaxis. On the other hand, if the IGRA conversion presented a false-positive result, then INH prophylaxis would be socioeconomically impractical and medically unethical, and could lead to the risk of INH resistance. IGRA also exhibits variability of test results. Therefore, it is not guaranteed that a patient will continue to have positive results once a positive diagnosis is made, and not all of the patients with positive results will be diagnosed with TB. In countries with low rates of TB incidence, PPD conversion sometimes occurs, whereas IGRA conversion rarely does (19). In Korea, since the IGRA conversion rate is high, we should implement differentiated treatment method rather than following the examples of developed countries.
In conclusion, IGRA conversion was observed in AS patients receiving anti-TNFα in Korea. A follow-up IGRA test could be helpful in identifying LTBI or new TB in AS patients receiving anti-TNFα. The interpretation of IGRA conversion and how best to proceed in such cases require further clarification.
 XML Download
XML Download