

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Rheumatoid arthritis (RA) is a systemic inflammatory disease which is associated with osteoporosis. The incidence of osteoporosis is doubled in patients with RA compared to the general population, leading to an increased rheumatoid comorbidity (1). Several case-control studies have documented a high rate of vertebral and hip fractures in patients with RA (2,3,4). The reported fracture incidence varies widely, with some authors pointing to the doubled figures in RA.
The fractures lead to chronic pain, disability, and bed-ridden morbidity, a common cause of mortality (5, 6). Glucocorticoids, high disease activity, decreased joint function, and cytokine hyperproduction drive the bone resorption and enhance the risk of falls, which is a major cause of osteoporotic fractures in patients with RA (7, 8). To prevent such fractures, it is important to identify the high-risk patients with low bone mineral density (BMD) and other clinical risk factors and prescribe pharmacological interventions at early stages of osteoporosis.
Bone strength depends on its mass and quality, which are subjected to the structure and material composition (9). BMD is only partially represent the bone strength, and is not predictive of osteoporotic fractures if taken alone. Pharmacological interventions in osteoporosis due to RA are often based on the T-score values measured by dual-energy X-ray absorptiometry (DEXA), similar to the strategy applicable to the general population. However, T-score alone may not be sufficient for the risk stratification in RA. To overcome limitations of T-score, the fracture risk assessment tool (FRAX) was developed by the World Health Organization (WHO), based on a twelve powered prospective cohort studies. The FRAX tool assesses a 10-yr probability of hip and other major osteoporotic fractures (10). It takes into account ten clinical risk factors, and can be calculated with or without femoral neck BMD. In 2008, the National Osteoporosis Foundation (NOF) of the USA endorsed the FRAX tool and recommended relevant pharmacological interventions for patients, who fulfill a 10-yr probability of ≥ 20% for a major osteoporotic fracture or ≥ 3% for a hip fracture. In many countries, the FRAX tool has been proved useful over the last five years, with a few reports reflecting on the measurements in patients with RA (11,12,13). A study from Korea demonstrated the differences between the FRAX, the NOF guideline, and the Korean Health Insurance Review Agency (HIRA) regarding the candidates for pharmacological interventions (14). It appears that patients who meet the FRAX criteria are different from those who are diagnosed with osteoporosis based on BMD values (15).
The FRAX criteria of the NOF are not accepted by the HIRA for the reimbursement of pharmacological interventions. Therefore the FRAX is rarely used in Korea. Inappropriate approaches to clinical risk factors for fractures and an under-treatment of osteoporosis are not the only concerns in Korea (16).
The aim of this study was to investigate the frequency of osteoporosis in Korean patients with RA and to identify patients who meet the FRAX criteria for pharmacological interventions despite the absence of osteoporosis. We also aimed at evaluating the demographic characteristics and the incidence of fractures in the identified patient group.
MATERIALS AND METHODS
Patients
We performed a prospective cohort study with 545 RA patients who visited the Department of Rheumatology, Seoul Saint Mary's Hospital in Korea between October 2010 and December 2012. All patients fulfilled the 1987 American College of Rheumatology (ACR) revised criteria or the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria for RA. Subjects older than 40 yr were enrolled in the study, because the osteoporotic fracture risk cannot be calculated by the FRAX tool for younger subjects. We recorded age, sex, disease duration, menopausal status, hormone supplement therapy in postmenopausal women, fracture history, history of parental hip fracture, glucocorticoid use, alcohol intake per day, smoking status, presence of secondary osteoporosis, biologic disease-modifying anti-rheumatic drugs (DMARDs) therapy, pharmacological intervention for osteoporosis, and BMD by questionnaire and a medical chart review. These are viewed as clinical risk factors for the FRAX calculation. Patients with malignancy under treatment, parathyroid diseases, malabsorption, chronic kidney disease, chronic liver disease, and bed-ridden state were excluded from the study. Women with a postmenopausal hormone replacement therapy were excluded from pharmacological interventions for osteoporosis.
Candidates for pharmacological intervention for osteoporosis
Based on the filled questionnaires and medical chart reviews, the 10-yr probability of major osteoporotic fracture and hip fracture was calculated by the FRAX tool. The FRAX calculation was done including femur neck BMD (g/cm2) and using the model for Korea (http://www.shef.ac.uk/FRAX/tool.aspx?country=25). BMD of the lumbar vertebrae (L1-L4) and both hips were measured by DEXA (GE Lunar, Madison, WI, USA). One DEXA machine was used to measure the BMD of all patients. Since no well-developed national BMD data were available for Korea, T- and Z-scores were calculated with the referent BMD of 8 tertiary medical centers, which used the same DEXA machine. BMD scores were classified based on T-score (SD for a reference population) by the following criteria: normal if ≥-1, osteopenia if -2.5<T<-1, and osteoporosis if T≤-2.5 for postmenopausal women or men ≥50 yr-olds. Z-scores≤-2.0 for premenopausal women or men <50 yr-olds were regarded as "low BMD for chronological age" and, thus considered as indicative of osteoporosis. This classification system was in accordance with the BMD criteria of the WHO and the International Society of Clinical Densitometry (ISCD). However, there is no consensus on the definition of osteopenia for premenopausal women or men <50 yr-olds. Therefore, these patients were divided into two categories: those with normal and low BMD for their chronological age (the same to osteoporosis). The candidates for pharmacological interventions against osteoporosis were defined by the BMD criteria of the WHO or the FRAX criteria of the NOF, which is 10-yr probability of ≥20% for major osteoporotic fracture or ≥3% for hip fracture.
Group classification and definition of fractures
The study population was divided into a group without a need for pharmacological intervention and those who met BMD or the FRAX criteria for pharmacological intervention. From the start of the study until October 2013, the new onset fractures were investigated by medical chart reviews and taken radiographs. Fractures were judged according to the plain X-ray films and official descriptions by musculoskeletal radiology specialists. In a patient who underwent a fracture operation in another hospital, the fracture was acknowledged if the patient's history corresponded to prosthesis on a plain X-ray film. The median follow up was 30 (10-30) months. The incidence of previous fractures and new onset fractures were evaluated between patients who met only the FRAX criteria of the NOF and patients with osteoporosis by BMD criteria of the WHO.
Statistical analysis
Normality of parameters was performed by Shapiro-Wilk test. Patient characteristics were expressed as median (interquartile range [IQR]) and percentages. To compare the incidence of fractures between patients satisfying only the FRAX criteria and patients with osteoporosis by BMD, incidence rate was investigated. Significance threshold was set at P<0.05. Software used for statistical analysis was SAS version 9 (Cary, NC, USA)
RESULTS
Patients and baseline characteristics
The characteristics of the 545 patients with RA are presented in Table 1. The study population included 29 men (5.4%) and 516 women (94.6%). There were 107 (20.7%) premenopausal and 409 (79.3%) postmenopausal women. The median (IQR) age was 57(50-64) yr and median (IQR) disease duration was 135 (62-210) months. There were 322 (59.1%) patients with osteoporosis by the BMD criteria of the WHO. Of them, 228 (41.8%) patients were on pharmacological therapy. 206 of the 228 patients were treated with bisphosphonates while the remaining 22 patients were treated with selective estrogen receptor modulators. The remaining 93 patients received no pharmacological intervention. With the HIRA, the patients were selected for the treatment using a simplified method based on a minimum T-score -3.0 of a BMD examination or radiologic evidence of osteoporotic fractures until October 2011. Pharmacological intervention did not include hormone replacement therapy in postmenopausal women.
Comparison of candidates for pharmacological intervention by both BMD criteria of the WHO and the FRAX criteria of the NOF guideline
To identify the discordance between the WHO BMD criteria and the FRAX criteria of the NOF guideline, the candidates were investigated for pharmacological intervention according to both criteria. The FRAX score was calculated including femur neck BMD (g/cm2). Table 2 shows the number and percentage of candidates for pharmacological intervention in the categorized groups. Eleven of 29 (37.9%) men were candidates for pharmacological intervention based on BMD values. This was similar to the candidate frequency in premenopausal women. Three hundred eleven of 516 (60.2%) women were candidates for pharmacological intervention based on BMD values, which is similar to the overall frequency of the candidates. The percentage of the candidates among premenopausal women and postmenopausal women was 39.2% and 66%, respectively. Postmenopausal women showed a 2-fold higher candidate frequency than premenopausal women.
As shown in Table 2, if the FRAX criteria of the NOF applied, 19 of 29 men (65.5%) were candidates for pharmacological intervention. With the FRAX criteria of the NOF, 303 of 516 women (58.7%) required the pharmacological intervention. The candidates for pharmacological intervention in pre- and postmenopausal women were 35 of 107 (32.7%) and 268 of 409 (65.5%), respectively. In men, candidates for pharmacological intervention by the FRAX criteria of the NOF were significantly more than those by BMD criteria of the WHO; 11 of 29 (37.9%) vs. 19 of 29 (65.5%). This difference was statistically significant (odds ratio, 3.1, P=0.036). However, women, whether premenopausal or not, showed a similar candidate frequency for pharmacological intervention, based on both criteria.
Distribution of candidates for pharmacological intervention by the FRAX criteria of the NOF Guideline in the BMD classified group
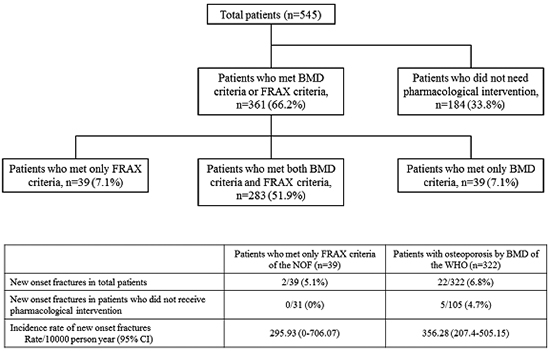
To further investigate the discordance of the two criteria for pharmacological intervention, all participants were divided into three groups, based on the BMD criteria of the WHO: normal, osteopenia, and osteoporosis. Premenopausal women or men <50 yr were divided into two categories: normal and osteoporosis. Then, candidates for pharmacological intervention by the FRAX criteria of the NOF were evaluated in the classified groups. Table 3 relates to the candidates for pharmacological intervention by the FRAX criteria of the NOF in each group. For 8 of 87 (9.2%) patients, 2 men and 6 premenopausal women, with normal BMD a pharmacological intervention for osteoporosis was required according to the FRAX criteria of the NOF. In osteopenia group, there were 31 of 136 (22.8%) subjects, candidates for pharmacological intervention according to the FRAX criteria of the NOF. For pharmacological intervention, there were 25 of 127 women (19.6%) with osteopenia. More than half of men with osteopenia (66.6%) fulfilled the FRAX criteria of the NOF. Expectedly, most participants with osteoporosis satisfied both criteria for pharmacological intervention. Based on Tables 2 and 3, the discordance of the candidates for pharmacological intervention was identified between BMD criteria of the WHO and the FRAX criteria of the NOF, which is remarkable in men and in osteopenia group. Fig. 1 displays the distribution of all patients requiring pharmacological intervention in the algorithm form. When BMD and the FRAX criteria applied, 184 patients with RA were not candidates for pharmacological intervention. Of the remaining 361 subjects, 283 fulfilled both criteria, but 39 patients satisfied the WHO BMD criteria only, and 39 patients satisfied the FRAX criteria of the NOF only.
Incidence of fractures in patients who met only the FRAX criteria of the NOF and in patients with osteoporosis
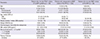
Patients eligible for pharmacological intervention were divided into 3 groups for the investigation of demographic characteristics: 39 patients who met only the FRAX criteria of the NOF, 322 patients with osteoporosis according to BMD criteria of the WHO, and 39 patients who met only BMD criteria of the WHO. The characteristics are presented in Table 4. The group satisfying the FRAX criteria of the NOF only presented with higher percentage of men (8 of 39 patients [20.5%]). The median (IQR) age was 61 (54-65) yr and the median (IQR) disease duration was 124 (52-178) months in patients who met only the FRAX criteria of the NOF. The percentage of subjects receiving biologic DMARDs was 12.8% in the same group. All 39 patients who met only the FRAX criteria of the NOF received glucocorticoid treatment. Eight of total 39 patients received a pharmacologic intervention for osteoporosis because of previous history of osteoporotic fracture. In the 322 patients with osteoporosis by BMD criteria of the WHO, there were 39 patients who met only BMD criteria of the WHO. Unlike 39 patients who met only the FRAX criteria of the NOF, there were no men and lower events of previous fractures in these 39 patients who met only BMD criteria of the WHO. The frequency of previous fractures was 25.6% in those who met only the FRAX criteria and 23.2% with osteoporosis by the BMD criteria of the WHO. This difference was not statistically significant (P=0.744). In both groups, the vertebra was the most common site of previous fractures.
New onset fractures were further evaluated during the follow-up period to ascertain whether pharmacological intervention is necessary for patients with RA who met the FRAX criteria of the NOF only. The comparison targets were patients with osteoporosis by BMD of the WHO. The median follow-up was 30 months. Other fracture sites incorporated were including tibia, fibula and rib, as well as common sites of osteoporotic fractures. As shown in Table 5, the frequency of new onset fractures in both groups was 5.1% among those who met the FRAX criteria of the NOF only and 6.8% among those with osteoporosis by the BMD criteria of the WHO. There were no statistically significant differences between two groups during the follow-up (P=0.687). There were no patients who developed new onset fractures in the 39 patients who met only BMD criteria of the WHO. The vertebra was the most common fracture site. New onset fractures were further investigated in patients who did not receive pharmacological intervention. However, there were no new onset fractures in patients who met only the FRAX criteria of the NOF. The incidence rate of new onset fractures in both groups was 295.93 cases per 10,000 person-years (95% confidence interval [CI], 0-706.07) and 356.28 cases per 10,000 person-years (95% CI, 207.4-505.15), respectively. The incidence rate had low statistical power because the number of new onset fractures was too small in patients who met only groups was overlapped. One of the four femur fractures was an atypical subtrochanteric fracture withouthe FRAX criteria of the NOF. However, there were no statistical differences because the width of CI in both groups was overlapped. One of the four femur fractures was an atypical subtrochanteric fracture without trauma. The atypical fracture is depicted in Fig. 2. The presented 66-yr-old woman had an 8-yr history of risedronate therapy.
DISCUSSION
This prospective cohort study demonstrated a higher frequency of osteoporosis and 10-yr fracture probability in men with RA than in premenopausal women. Several patients with a T-score >-2.5 were classified eligible for the pharmacological intervention according to the FRAX criteria of the NOF. Of these patients, 21% were men with RA. The present study proved that the incidence of fractures in these patients was higher when compared to the general population and not inferior in comparison to patients with osteoporosis. In fact, the incidence rate of fractures was higher than those of incidence rate 114.99 cases per 10,000 person-years reported by the HIRA in 2008.
Several previous studies reported the FRAX as useful for the risk assessment and for the identification of high risk patients requiring pharmacological intervention worldwide (10,11,12,13). Also, several reports verified the use of the FRAX tool for patients with inflammatory arthritis (15, 17). This is the first study using the Korean FRAX model to evaluate the fracture risk in patients with RA. The Korean FRAX model was not validated yet. The use of the Korean FRAX model may not be an issue, because it was developed based on a large epidemiologic study from Korea. A recent Korean study demonstrated the discrepancy between the standards of HIRA and FRAX (based on the Japanese FRAX model) (14). In that study, 13.4% of patients met the FRAX criteria without osteoporosis. However, in the present study 16.9% of patients met the same criteria. Moreover, the median values of the FRAX score are higher in the Korean model: 10-yr probability of major osteoporotic fracture -7.9% vs. 12% and 10-yr probability of hip fracture -1% vs. 3.8%. Although participants were different in both studies, more patients in the Korean FRAX model required pharmacological intervention.
The FRAX model was originally proposed for postmenopausal women and men older than 50 yr. The model is now applicable for 40-90 age groups. This is why we collected data for RA patients aged ≥40 yr. Although the ISCD or NOF recommend BMD evaluation in postmenopausal women and men ≥50 yr (18), the authors measured BMD regularly, from the time of diagnosing RA which is a critical risk factor for a fracture. Because of this regular procedure, a single center can collect a large number of FRAX data, including femur neck BMD.
In general, BMD of men is higher than that of women in same age groups (19). The reasons are higher peak bone mass in men (20), heavier weight than women (21), a rapid bone resorption regarding the sex hormone withdrawal in women (22). As presented in this study, men with RA showed a significant difference of candidates for pharmacological intervention based on BMD and the FRAX criteria, and this difference was more expressed in men compared to women. The FRAX model calculates a lower risk score for men than for women, with an assumption that all other variables are similar. To explain this unexpected result, the characteristics of the FRAX variables in men were investigated further. The mean±SD of BMI was 22.9±2.5 kg/m2 in men and 22.5±3.2 kg/m2 in women (P=0.434). Age was also not different between both groups (P=0.845). Other than age, sex and BMI, men had a mean score 2.6 for the clinical risk factors which is higher than the mean clinical risk factor score 2 for women (P=0.003). Men were more exposed to alcohol and smoking than women, which may explain higher FRAX score in men with RA.
Though RA is a strong risk factor for osteoporosis, the prevalence of osteoporosis due to RA varies widely all over the world (15%-35%) (1, 23). According to the Korean nationwide survey in 2009, the prevalence of osteoporosis was 32.6% in postmenopausal women of the general population (24). However, the prevalence of osteoporosis in the present study is 66%, nearly twice that reported in the Korean nationwide survey. This is higher than 51% in the previous report, where the Japanese FRAX model was used for Korean patients with RA (14). Considering the results of all previous Korean studies, including the current one with its limitation as a single-center study, a nationwide and RA-oriented epidemiologic survey is warranted to accurately identify the prevalence of osteoporosis in Korea.
There are still debates whether the femur neck BMD values should be included in the FRAX score calculations for a more accurate fracture risk prediction. In the present study, the femur neck BMD value (g/cm2) was included in the FRAX calculation since all patients presented with the BMD data. In some cases, the FRAX score substantially differed, depending on the inclusion of femur neck BMD values in the calculation (mostly remarkable elevation of the FRAX score with femur neck BMD). This is one of the several limitations of the FRAX model. Although individual differences such as peak bone mass, rate of bone resorption, and life environment have to be considered to assess the fracture risk, the FRAX cannot reflect individual's bone status. It is thus advisable to take into account femur neck, and even other sites'-BMD values for an individual's the FRAX calculation. The femur neck BMD in the FRAX model is an acceptable inclusion since it was shown to predict major osteoporotic fractures, except femur neck fractures (12). We are looking forward to suggesting a new FRAX model, which will include vertebral BMD for more accurate fracture risk assessment.
The effect of glucocorticoids on osteoporotic fractures in patients with RA is not fully explored. Systemic glucocorticoids enhance the risk of fracture disregarding the dose. This is why the FRAX model takes into account whether or not a patient has been exposed to oral glucocorticoids at daily doses equivalent to 5 mg prednisolone or more during a period of more than 3 months. In the current study, 432 patients were on glucocorticoid therapy and 378 patients were taking ≤5 mg prednisolone daily (or an equivalent dose of other glucocorticoids). Fifty-four patients were exposed to doses ≥7.5 mg/day. Giving the same weighted value for patients who took different dose of glucocorticoid it was inappropriate for the assessment of osteoporotic fracture risk. A recent study suggested the guideline for the adjustment of the FRAX model to the dose of glucocorticoids (25, 26). According to that study, the probability of major fractures decreased by about 20%, depending on age in cases of low dose exposure (<2.5 mg prednisolone daily or equivalent). The unadjusted FRAX value could only be used in patients exposed to 2.5-7.5 mg daily. The probabilities could be upward revised by about 15% for high doses (>7.5 mg daily). Another point of consideration may be an exposed duration as well as the dose of prednisolone. A population-based cohort study demonstrated that patients exposed to glucocorticoids at least 90 days within 12 months presented with a lower femur neck T-score, compared to those who never received glucocorticoids (27). To sum up, the FRAX tool may accurately predict the risk of fractures if dose and duration of glucocorticoid therapy are taken into account.
Our study has some limitations. First, the Korean FRAX model is not validated yet. The Korea National Health and Nutritional Examination Surveys are still in progress. When the survey finish, the Korean FRAX model can be validated based on the results of the survey. Second, the number of patients was relatively small, and the current study was a single-center study. In particular, the number of men was much smaller than that of women. Nevertheless, RA is more common in females than in males, at a 2:1 to 3:1 ratio (28). Third, to evaluate the incidence of fractures the duration of follow-up duration was not long. A larger number of patients, more events of fractures, and longer duration of follow-up are required for future evaluations. Fourth, the 10-yr probability of fractures for RA patients was evaluated on the number of pharmacological interventions for osteoporosis assessed by the FRAX. The effect of bisphosphonates and selective estrogen receptor modulators on reducing osteoporotic fractures are well documented in previous studies (29,30,31). Therefore, the fracture risk of patients undergoing pharmacological intervention may be different from that of patients without such interventions.
In conclusion, we demonstrated the discordance in candidates for pharmacological intervention between BMD and the FRAX criteria. Remarkably, men with RA showed a high prevalence of osteoporosis. There were more candidates for pharmacological interventions in men after the application of the FRAX criteria. The incidence rate of fractures in RA patients who met the FRAX criteria only without osteoporosis was higher than that in the general population. Therefore, clinicians should more actively implement the FRAX tool and treat RA patients who meet the FRAX criteria.



 XML Download
XML Download