

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Microalbuminuria is a well-known risk factor or predictor for cardiovascular morbidity and mortality in individuals with hypertension or diabetes mellitus (3, 4) and even in the general population (1, 2) as well. The mechanism of occurrence of microalbuminuria is unclear although it is known to be a marker of generalized endothelial dysfunction triggered by metabolic processes, and insulin resistance (5, 6, 7). In addition, insulin resistance is a risk factor of microalbuminuria, especially in patients with diabetes or dyslipidemia (8, 9).
Another mechanism of microalbuminuria is associated with generalized vascular dysfunction through arterial stiffness (5, 6, 7). It is not clear whether the cause of microalbuminuria is an independent action of arterial stiffness and insulin resistance or dependent interaction of them (10). So, it is important to verify the independency between arterial stiffness and insulin resistance to understand the mechanism of microalbuminuria occurrence. Arterial stiffness is a useful marker of vascular damage and cardiovascular disease (CVD) risk (5, 7). Pulse wave velocity (PWV) is an indicator of arterial stiffness and a marker of atherosclerosis (11). Of the various PWV parameters, carotid-femoral PWV (cfPWV) is the noninvasive gold standard of arterial stiffness (12), but brachial-ankle pulse wave velocity (baPWV) is a promising new measure for screening large samples for arterial stiffness due to its technical simplicity and short sampling time (8, 9, 11). In addition, baPWV is useful as a means of estimating the atherosclerotic disease of arteries (13).
Several studies have shown that arterial stiffness is a risk factor for microalbuminuria (10, 14, 15, 16, 17). As an example, the Taichung study performed in Taiwan targeting a middle aged community population showed the strong association between albuminuria and arterial stiffness, especially on hypertensive or diabetic subjects (10, 18). However, the prevalence of hypertension and diabetes varies depending on the population characteristics; therefore, results may be different in Korea. In addition, a study revealing the association between albuminuria and arterial stiffness existed targeting participants visiting the health promotion center for health screening (15). However, there is no study of the general population in Korea. Besides, results of epidemiologic evidence are easy to generalize, so this study is further needed.
The purpose of this study was to assess whether baPWV is an independent risk factor of microalbuminuria regardless of insulin resistance in the elderly population (over-40 yr).
MATERIALS AND METHODS
Subjects
From February 2005 to December 2006, a total of 1,841 people aged over 40 yr, living in Yangpyeong, Gyeonggi-do, Korea, were invited to participate in the baseline Multi-Rural Cardiovascular Cohort Study conducted in Korean rural communities. Arterial stiffness has been measured in the Multi-Rural Cardiovascular Cohort since 2005 as part of the Korean Genetic Epidemiology Study. Participants responded to a questionnaire which included sociodemographic information, past medical history (defined as "diseases diagnosed by medical doctors") and lifestyle behavior, including smoking, alcohol consumption, daily physical activity and dietary patterns. Participants also underwent a complete physical examination including height, weight, waist circumference and blood pressure. Blood chemistry such as fasting blood glucose and lipid profile, urinalysis and baPWV measurement was carried out. Definitions of history of hypertension and diabetes mellitus were based upon whether they had been diagnosed by a medical doctor and included taking drugs. Hypertension was defined as systolic blood pressure (BP)≥140 mmHg, diastolic BP ≥90 mmHg, or taking antihypertensive drugs. Diabetes mellitus was defined as fasting plasma glucose≥126 mg/dL, having diabetes mellitus history or taking antidiabetic drugs. We excluded participants who fitted the following exclusion criteria: history of cardiovascular disease, stroke or cancer (n=149), presence of macroalbuminuria or overt proteinuria (n=22) and incomplete data (n=22). Finally, a total of 1,648 participants were included in the study. The study was approved by the Institutional Review Board of Hanyang University Medical Center and all participants gave their informed consents.
Brachial-ankle pulse wave velocity
BaPWV was measured with an automatic apparatus (VP-2000; Colin Corporation, Komaki, Japan). Participants rested for at least 5 min to stabilize their heart rate and were then examined in a supine position with a pneumatic cuff connected to a plethymographic sensor to determine volume pulse waveform and an oscillometric pressure sensor to measure blood pressure placed on both upper arms and ankles, and electrocardiogram electrodes placed on both wrists. The average of the left and right side baPWV values was used in the analysis. Subjects were divided into the following four quartiles with respect to baPWV values: <1,325 cm/s, 1,325-1,515 cm/s, 1,515-1,765 cm/s, >1,765 cm/s; males were divided into <1,379 cm/s, 1,379-1,557 cm/s, 1,557-1,796 cm/s, >1,796 cm/s; and females into <1,285 cm/s, 1,285-1,489 cm/s, 1,489-1,724 cm/s, >1,724 cm/s.
Blood pressure and blood chemistry
Blood pressure was measured twice, with a 5-min interval, after at least a 5-min rest, on the right side arm in a seated position, using a mercury sphygmomanometer. Two trained observers performed the measurements in a standardized manner according to a written protocol covering preparation of subjects, arm level, peak inflation pressure, inflation and deflation rate, reading the scale, and measurement of systolic and diastolic blood pressure by Korotkoff sound I and V, respectively. We used the mean of the two measurements in the analysis.
All blood samples were taken after overnight fasting for at least 8 hr. Fasting blood glucose, total cholesterol and triglycerides were analyzed enzymatically using an automatic analyzer (Hitachi 747 automatic analyzer, Hitachi, Tokyo, Japan). High density lipoprotein cholesterol (HDL-C) was measured directly and low density lipoprotein cholesterol (LDL-C) was estimated using the Friedwald's method (19). Serum insulin levels were analyzed with a Gamma Counter (Packard, Ramsey, Minnesota, USA) and an insulin RIA Kit (Biosource, Nivelles, Belgium) using immunoradiometric assays (IRMA). Insulin resistance was measured with thehomeostatic model assessment (HOMAIR) using serum glucose and insulin levels. It was obtained from the following formula (20):
Microalbuminuria
First-voided morning spot urine samples were collected from all participants and stored in a -20℃ deep-freezer. Urinary albumin and creatinine were assayed by turbidimetric immunoassay and radio-immunoassay using an ADVIA Centaur Immunoassay System (Siemens Healthcare Diagnosis, Tokyo, Japan), respectively. We calculated urinary albumin to creatinine ratios (UACR) using urinary albumin and creatinine concentrations from the same samples, and categorized them in the same way for men and women (6) into 3 groups: 1) UACR less than 30 mg/g, normoalbuminuria; 2) UACR 30-300 mg/g, microalbuminuria; 3) higher than 300 mg/g, macroalbuminuria or overt proteinuria.
Statistical analysis
All analyses were gender stratified due to the different characteristics of men and women. Age adjusted comparison of general characteristics according to baPWV were conducted by the general linear model for continuous variables, and by the Cochran-Mantel-Haenszel test for categorical variables. Participants were classified into those with normoalbuminuria and those with microalbuminuria, and their general characteristics and clinical results were compared using Student's t-test and the chi-square or Fisher's exact test. UACR, triglyceride, HOMAIR and baPWV data were transformed to a normal distribution using natural logarithms to improve normality. Multivariate logistic regression analysis was performed to determine associations with baPWV by adjusting for significant variables in the univariate analysis. Odds ratios (ORs) were calculated by multivariate logistic regression analysis. P values less than 0.05 were considered statistically significant. All statistical analyses were performed with SAS 9.2 (SAS Inc., Cary, NC, USA).
RESULTS
General characteristics of the study population
General characteristics of the study population by gender are described in Table 1. The average age of the subjects was 60.9±10.5 yr; and 677 individuals (41.1%) were male. Body mass index (BMI) was 24.6±3.2 (kg/m2). Systolic blood pressure (SBP) was 123.7±17.3 mmHg and diastolic blood pressure (DBP) 79.8±10.7 mmHg. HOMAIR was 2.6±1.5, UACR 12.6±33.5 mg/g and baPWV 1,521.9±451.1 cm/s. Prevalence of microalbuminuria in the total study population was 9.9%; 8.3% in men, and 11.0% in women. There were no statistically significant differences in the history of diabetes mellitus (DM), physical activities, or prevalence of microalbuminuria between genders. However, BMI, total cholesterol, triglyceride, fasting insulin, HDL-C, LDL-C, HOMAIR, frequency of histories of hypertension, were all significantly higher in women than men. On the other hand, waist circumference, SBP, DBP, fasting blood glucose, triglyceride and baPWV were higher in men than women. Also, the proportion of men that smoked or drank alcohol was higher than that in women.
Age-adjusted characteristics according to baPWV quartiles
Table 2 presents age-adjusted characteristics according to baPWV quartiles. Age, SBP, DBP, fasting blood glucose, triglyceride, HOMAIR and history of hypertension were significantly different among the quartiles in both men and women. History of alcohol consumption was significantly different among the quartiles in men only. DM history was significantly different among the quartiles in women.
Comparison of the normoalbuminuria and microalbuminuria groups
Table 3 compares characteristics of the normoalbuminuria and microalbuminuria groups. Age, fasting blood glucose, the proportion of history of hypertension and DM were significantly higher in the microalbuminuria group in both sexes. SBP, DBP and total cholesterol were significantly higher only in women of the microalbuminuria group, while HOMAIR was significant higher only in men (P=0.013 in men vs. P=0.055 in women).
BaPWV values were higher in the microalbuminuria group than the normoalbuminuria group in both men (1,538, 1,370-1,777 cm/s vs. 1,776, 1,552-2,027 cm/s, P<0.001) and women (1,461, 1,271-1,687 cm/s vs. 1,645, 1,473-1,915 cm/s, P<0.001).
Odds ratios and 95% Confidence intervals (CI) of microalbuminuria stratified by diseases status
Table 4 shows adjusted ORs and 95% CIs of microalbuminuria according to baPWV quartiles stratified by hypertension and diabetes status adjusted for age, pulse rate, systolic and diastolic blood pressure, fasting blood glucose, total cholesterol, triglyceride and HOMAIR. Especially, the OR of microalbuminuria was 4.46 (95% CI, 1.27-15.63) according to baPWV 4th quartiles (Q4) in women without hypertension.
Relationship between baPWV and microalbuminuria
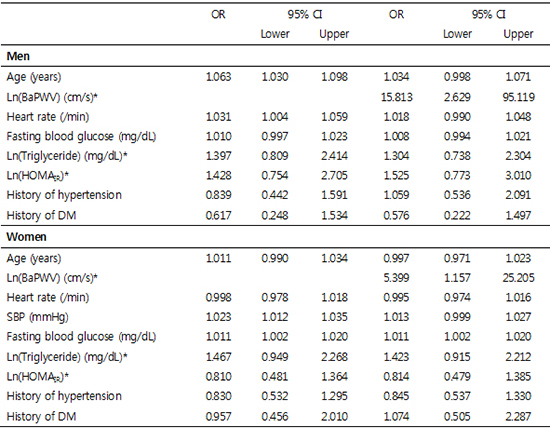
Results of multivariate logistic regression analyses are described in Table 5. Five models were used to estimate the relationship between baPWV and microalbuminuria. BaPWV, triglyceride and HOMAIR data were log-transformed and used for analysis. In model I, which was adjusted for age, no variables were independently associated with microalbuminuria in both men and women. In model II, HOMAIR was also included. Log (baPWV) (OR, 18.784; 95% CI, 3.245-108.741) and log (HOMAIR) (OR, 2.153; 95% CI, 1.194-3.882) were both independent risk factors of microalbuminuria in men, but log (HOMAIR) (OR, 1.187; 95% CI, 0.753-1.868) was not an independent risk factor in women. In model III, in case of men, which was also adjusted for fasting blood glucose, log (baPWV) (OR, 15.830; 95% CI, 2.687-93.248) was an independent risk factor; however, (HOMAIR) (OR, 1.560; 95% CI, 0.794-3.063) was not. Fasting blood glucose was a significant risk factor in both men (OR, 1.012; 95% CI, 1.001-1.023) and women (OR, 1.011; 95% CI, 1.003-1.019). Fasting blood glucose and HOMAIR were included in same model, because there were judged not to have multicolinearity between them (r, 0.532; P<0.001). In model IV, which included additional variables such as history of hypertension or diabetes, only log (baPWV) (OR, 17.539; 95% CI, 2.969-103.626) was significant in men, and log (baPWV) (OR, 13.428; 95% CI, 3.776-47.758) and fasting blood glucose (OR, 1.011; 95% CI, 1.002-1.020) in women. Finally, in model V, also adjusted for clinical parameters such as SBP (women), log (triglyceride), log (baPWV) (OR, 15.813; 95% CI, 2.629-95.119) was the only independent risk factor in men, while log (baPWV) (OR, 5.399; 95% CI, 1.157-25.205) and fasting blood glucose (OR, 1.011; 95% CI, 1.002-1.020) were significant in women, just as model IV.
In summary, baPWV was the only factor examined that was independently associated with microalbuminuria in both genders and in all the models studied here.
DISCUSSION
The present study showed that elevated baPWV was an independent risk factor of microalbuminuria in both genders regardless of potential confounders. Fasting blood glucose was an additional independent risk factor of microalbuminuria in women. On the other hand, the effect of HOMAIR was not statistically significant after adjusting for various confounding factors.
In this study, the prevalence of microalbuminuria was 9.9% (163/1,648) overall; and 8.3% (56/677) in men and 11.0% (107/971) in women. This result is similar to a previous study performed in Sweden (21). However, the prevalence found here is bigger than in a population-based study conducted in Korea (15), which might be explained by age and prevalence of chronic disease according to the subjects' old age in the present study (2). In addition, the prevalence of microalbuminuria was different according to gender. The prevalence of microalbuminuria was higher in women. However, the prevalence of women might be higher within an insignificant range (P=0.066). Afterward, further study is needed in association with the difference of prevalence according to gender.
Blood pressure in the present study was lower than the previous study performed in Taiwan by about 10 mmHg in the group without microalbuminuria and by about 20 mmHg in the microalbuminuria group (10). The prevalence of albuminuria was also lower than the Taiwan study; however, fasting blood glucose levels were very similar. The mean value of baPWV in microalbuminuria was lower than the Taiwan study by >100 cm/sec. The relative contribution of hypertension and diabetes to the relationship between arterial stiffness and microalbuminuria may be affected by the blood pressure level in the population (22).
In our study, SBP, DBP, fasting blood glucose and hypertension history increased with increasing baPWV after adjusting for age. This is consistent with a study performed in Japan (23). However, in the Taichung community health study in Taiwan, BMI, waist circumference, total cholesterol and HOMAIR, as well as the variables which were significant in our study, all increased with increasing baPWV (10).
The effects of gender, age, BMI, central obesity and smoking on microalbuminuria are controversial (24). Of these factors, none was related to the presence of microalbuminuria in our study. In fact, BMI and central obesity were not related to microalbuminuria in several previous studies (14, 16, 17).
There is evidence that insulin resistance plays an important role in the development of microalbuminuria (25); and insulin resistance is also reported to be positively related to high arterial stiffness (26). However, in the present study, we attempted to incorporate arterial stiffness into the previously-known microalbuminuria model explained by insulin resistance. Insulin resistance was consistently independent of their relationship with microalbuminuria even after adjusting for potential factors related to microalbuminuria. These findings suggest that arterial stiffness might be important in the development of microalbuminuria. So that independent action of arterial stiffness needs to be included in the microalbuminuria model for future study.
In the present study, considering only women, not HOMAIR but fasting blood glucose was an independent factor in addition to arterial stiffness. Regarding gender differences, Utsunomiya et al. (27) found that central obesity and HOMAIR were important factors increasing UACR in men, but not in women. A gender-specific hormonal effect was suggested as a possible factor. However, in our study HOMAIR was not related to microalbuminuria in the general population or in subjects with hypertension or diabetes. This outcome was similar to the results of a Dutch study performed by Jager et al. (28). In the model including baPWV or arterial stiffness for predicting microalbuminuria, fasting blood glucose suggests that the effect of HOMAIR is partly mediated by increased arterial stiffness on women, as shown in Table 2.
Microalbuminuria is caused by endothelial damage that can arise by several mechanisms (7, 29), but the precise mechanism is not clear. Generally, microalbuminuria is seen as a pathological event related to microvascular abnormalities resulting from hemodynamic or metabolic processes (7, 10). Thus, hypertension is an important risk factor for microalbuminuria. Even if hypertension is not a direct cause of microalbuminuria, the prevalence of microalbuminuria is greatly elevated in individuals who have essential hypertension (25). This result implies that microalbuminuria is a marker of endothelial damage especially in hypertension (22). Another possible mechanism is related to insulin resistance. Metabolic changes caused by hyperglycemia, for example, chronic inflammation triggered by reactive oxygen species, inflammatory cytokines and growth factors, are associated with generalized and glomerular endothelial dysfunction (25). Several previous studies found that higher HOMAIR was associated with microalbuminuria (4, 8, 27). Recently, evidence has emerged that high pulse pressure may have an important effect on albuminuria. High pulse pressure leads to arterial stiffness (30); and kidney cells are passively perfused by pulsatile flow which can cause endothelial damage by disrupting small arteriolar vessels (31). It is not yet clear whether the two mechanisms i.e. the metabolic process-associated level of blood pressure and the pulsatile character of the arterial pulse, work independently (10, 25). Furthermore, an association between arterial stiffness and insulin resistance has been reported (32, 33). This relationship was also seen in women in the present study.
The results of our study do not support an independent role of HOMAIR as a parameter of insulin resistance related to microalbuminuria when arterial stiffness is adjusted for. Fasting glucose level may be an independent risk factor of microalbuminuria, but only in women with their more adverse metabolic and lipid profiles.
It is well known that baPWV is affected by the presence and severity of peripheral artery disease (PAD) (34). Therefore, the consideration of the ankle-brachial index (ABI) reflecting PAD might be needed in this study. We did a multiple logistic regression analysis except for participants with low ABI (<0.9, men n=21, women n=32) and high ABI (>1.2, men n=35, women n=16) (35); however, results were similar to that in Table 5. The reason for that is the subjects of this study are from the general population; therefore, the number of individuals with abnormal ABI is few.
This study has several limitations. First, it had a cross-sectional design. Therefore, it was unable to establish any causal relationship between arterial stiffness and microalbuminuria. Second, we used a single measurement of first morning spot urine to calculate urinary albumin to creatinine ratios. Urinary albumin excretion can be affected by several factors such as oral fluid intake (36), so a more accurate measure such as using 24-hr urine collections would be desirable. However, single void urine samples give good estimates of 24-hr urine albumin excretion (37). In addition, it has been reported that spot urine protein-creatinine ratio reflects the amount of 24-hr urinary protein excretion with high accuracy (38). Third, we did not consider the influence of drug treatment such as angiotensin converting enzyme inhibitor or angiotensin II receptor blocker, which are known to be able to reduce arterial stiffness (23, 39) because we had no information about medications taken by the patients.
Nevertheless, the strengths of this study are its relatively large sample size and the fact that it was not based on patients who visited hospitals but on a rural population. Therefore, this study can reflect the characteristics of the general population, especially elderly from rural communities. We were able to confirm a relationship between PWV and microalbuminuria. This study provides more useful and strong epidemiologic evidence of association between arterial stiffness and microalbuminuria in population of over 40 yr. Results show that there is a strong association between microalbuminuria and arterial stiffness regardless of insulin resistance in rural population groups past middle age. Also, high baPWV measurements may be a good indicator of microalbuminuria. In other words, baPWV may be a useful screening tool for predicting cardiovascular complications.


 XML Download
XML Download