

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Latent carcinomas are carcinomas found in autopsy specimens, and latent thyroid carcinomas are defined as tumors 1.5 cm or less in diameter and not suspected clinically (1). Although no autopsy studies of the Korean population have been published, a PubMed search of autopsy reports from the 1960s onwards revealed that small foci of thyroid carcinoma were often present in the thyroid glands of individuals who died of unrelated illness (2). However, few comparative studies have been performed, because of differences in definitions, the pathological sectioning techniques used, and the pathological criteria used to diagnose thyroid cancer (2).
The prevalence of latent thyroid carcinomas, which are frequently minute and occult, has been reported to range from 1.0% to 35.6% in different systematic autopsy series, this incidence is much higher than that of clinically evident carcinomas of the thyroid (1, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16). Papillary thyroid carcinoma (PTC) is a common thyroid malignancy, accounting for 86%-90% of thyroid cancer, and has indolent clinical characteristics. Papillary thyroid microcarcinomas (PTMCs), defined by the World Health Organization (WHO) as papillary thyroid carcinomas of maximum diameter of ≤1.0 cm (17), account for 30%-40% of PTCs, although recently their incidence is increasing rapidly (18). Most PTMCs are found incidentally, with some changing in clinical behavior to become clinical cancers (19).
At present, the relationship between latent PTCs and PTMCs is unclear, as in the treatment of patients with latent PTCs. There are two important questions with regard to latent PTCs. First, what is the relationship between latent papillary thyroid carcinomas and PTMC? Second, what should the therapeutic attitude be toward a patient in whom PTMC is discovered?
Because of the indolent behavior of PTMCs and the good prognosis of patients with these tumors, treatment of PTMCs is sometimes confused with that for latent PTCs. However, there is no evidence of similarity between PTMCs and latent PTCs. Despite this, autopsy studies have had a negative influence on the choice of therapy in patients with PTMC (20).
This study aimed to review the literature of latent PTCs discovered at autopsy and describe the available pathologic and demographic differences from a group of PTMCs the reported in a previous publication.
MATERIALS AND METHODS
Study subjects
The clinicopathologic features of PTMCs have been described previously in the Korean Journal of Head & Neck Oncology in 2008 (18). Between January 2000 and December 2005, 1,355 patients with PTMC treated at the Thyroid Cancer Center, Yonsei University College of Medicine, Seoul, Korea were evaluated (Group I).
To identify patients with latent PTCs, the MEDLINE database was searched via the PubMed (http://www.ncbi.nih.gov/sites/entrez/) on 24 February 2011 for the MeSH headings "occult", "latent", and "thyroid cancer". We carefully reviewed all potentially relevant articles, and studies were included in the analysis if they met all of the following criteria: 1) including papillary thyroid carcinoma, 2) performing autopsy, 3) providing available clinicopathologic characteristics, 4) where participants always included general population of both sexes without age restriction, and 5) written in English.
Of the identified articles, 15 were included in this study (Table 1). These 15 papers described 8,619 autopsy specimens, 989 of which (11.5%) had latent PTCs (1, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16).
A meta-analysis was performed to identify differences between the clinicopathologic features of PTMCs evaluated in our institution (Group I) and those of latent PTCs evaluated in autopsy studies (Group II).
Statistical analysis
Categorical variables were summarized as counts and percentages, and continuous variables as means. Comparisons between PTMCs and latent PTCs were performed using the one sample t-test, assuming a mean age of 47.3 in patients with PTMCs, whereas Pearson's chi-square test was used to compare gender, tumor size (with cut-offs of 0.5 cm for PTMCs versus 1-3 mm cut-off value for latent PTCs), mutifocality, and cervical lymph node metastasis. All statistical analyses were performed using SAS 9.2 software (SAS Institute Inc., Cary, NC, USA). A P value less than 0.05 was considered statistically significant in all tests.
RESULTS
This study included 1,355 cases of PTMC (Group I) and 989 cases of latent PTCs from 15 autopsy reports (Group II). The clinicopathologic results of PTMCs reported in the Korean Journal of Head & Neck Oncology are listed in Table 2.
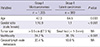
We compared the following variables between two groups; patient age, sex distribution, multifocality, and cervical lymph node metastasis. These variables and results of statistical analyses are listed in Table 3.
Mean patient age was 47.3 yr in Group I and 65.4 yr in Group II (P=0.003), and sex distribution (male:female) was 1:10.9 in Group I and 1:1 in Group II (P<0.001) with statistical significance.
Tumor diameter was not comparable between the two groups: the majority (67.3%) of patients in Group I had tumors larger than 0.5 cm in diameter, and whereas tumors with tiny diameters that were described as small foci (<1-3 mm) were common in Group II.
Multifocality was significantly less frequent in Group I than in Group II (24.7% vs 30.5%, P<0.001). The rates of cervical lymph node metastasis rate were higher in Group I than in Group II (33.4% vs 10.0%) but the difference was not statistically significant.
DISCUSSION
Of the 8,619 thyroid glands obtained in 15 autopsy studies, 989 (11.5%) were positive for latent PTC (Table 1). However, the prevalence of latent PTC has been found to vary considerably, from 1.0% to 35.6%. Comparing this prevalence among autopsy studies is complicated by differences in methods of examination, section intervals (ranging from 4 µm to 4 mm), diagnostic criteria, and sample selection. In particular, different methods of examination can have a profound effect on the observed prevalence of carcinoma (1).
One factor that may cause a spurious increase in the rate of latent PTC at autopsy is bias of the entire series in favor of thyroid carcinoma or a related disease (1). We, however, did not directly select for PTC at autopsy, because almost all of the latent carcinomas were small and clinically occult. There also was no evidence of indirect selection for patients with thyroid carcinoma. Another factor related to an increased prevalence rate is that the incidence of thyroid carcinoma is fundamentally very high.
This can be explained by the two-stage theory. A thyroid carcinoma may arise in response to various factors, including environmental and genetic factors, but its growth may be deficient and it may lack clinical characteristics. Subsequently, other factors may promote the development of clinical thyroid carcinoma (21, 22). This two-stage theory explains the small size, described as foci, and the sclerotic characteristics of the latent PTCs.
The latent PTC group contained a high proportion of very small tumors. Most (67.3%) patients with PTMC had tumors larger than 0.5 cm in diameter, whereas most latent PTCs were small foci (<1-3 mm in size). Moreover, most of the latent PTCs showed sclerotic patterns, indicating that these tumors had arisen a long time prior to autopsy.
Papillary carcinomas arise as non-sclerosing tumors; during further growth, stromal fibrosis (non-encapsulated sclerosing tumors) occurs or a fibrous capsule (encapsulated tumors) forms with various degrees of cellular infiltration, with the latter likely associated with a host reaction (10).
In contrast to the marked female predominance of clinical thyroid carcinoma, the prevalence of latent carcinomas did not differ significantly between men and women. Also, whereas most hospital-based series have found a slight male predominance, we observed a 1:1 ratio of latent PTCs in males and females. Moreover, patients with latent PTC were older than those with PTMC. Older age and male predominance, however, may be caused by a selection bias in patients with latent PTCs, since these studies were based on autopsy data.
Multifocality was significantly more prevalent in patients with latent PTC than in those with PTMC (30.5% vs 24.7%, P<0.001). In contrast, cervical lymph node metastasis was more prevalent in patients with PTMC than in those with latent PTC (33.4% vs 10.0%), probably because lymph node status was not fully examined in autopsy studies.
In conclusion, despite the limited ability to compare variables between patient with PTMC and those with latent PTC, and despite selection bias, there are differences between these groups, indicating that latent PTCs and PTMCs should be considered distinct entities. The choice of therapy in patients with PTMC should not be influenced by the concept of latent PTCs. Future autopsy studies should include molecular and metabolic markers.


 XML Download
XML Download