

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cholera, a rapidly dehydrating diarrhoeal disease, is spread mainly by food and water contaminated through the fecal material of infected carriers or persons (1, 2). The main symptoms of cholera are acute and profuse watery diarrhea with vomiting for a period of one or few days. Within 3-4 hr of starting the symptoms, a healthy person may become severely dehydrated and may die within 24 hr if a proper treatment is not given immediately (1). Cholera is one of prevalent endemic diseases particularly in South-Eastern Asia and Africa. Approximately 3-5 million people are affected by this disease, and 100,000-130,000 deaths are reported in every year throughout the world (3). The rate of cholera in endemic areas varies from around 1 to 8 per 1,000 population and children aged of 2-9 yr are in high risk of infection (1, 2).
Cholera is caused by the ingestion of toxigenic serogroups of Vibrio cholerae, a Gram-negative, rod-shaped non-invasive mainly waterborne bacterium. There are more than 200 serogroups of V. cholerae available in nature. However, the disease is mainly caused by the serogroups O1 and O139 (1, 2). O1 strains are divided into two biotypes (e.g., classical and El Tor). The classical biotype has been discovered during the cholera outbreaks in India, and was responsible for the previous six pandemics in modern history. El Tor causes more asymptomatic cases as compared to the classical strain, and is responsible for the seventh pandemic that started in 1961 and continues till today. V. cholerae O1 strains are further divided into two serotypes (e.g., Ogawa and Inaba) based on their phenotypic differences in O1 antigen. In 1992, V. cholerae O139 strain was found that caused extensive epidemics in Bangladesh and India, and subsequently in other parts of South Asia. This strain, a genetic derivative of El Tor biotype in which the O1 biosynthetic genes were replaced by the O139 biosynthetic genes, appears to be associated with more severe cholera disease (1, 2).
Enteric vaccination has already been regarded as the most effective approach to control such illnesses as well as to prevent cholera in endemic countries with limited public health and sanitary facilities (4). Injectable vaccine is not recommended by the World Health Organization (WHO) mainly because of its limited efficacy and short duration of protection. To maximize the intestinal secretory antibody response and long-lived efficacy of cholera vaccine, the manufacturing technology of vaccine has been shifted from parenteral (injectable) to oral of which the antigens could be delivered directly to the mucosal surface (2). At present, two types of oral cholera vaccines (OCV) are available in the market i.e., 1) Dukoral and 2) Shanchol and mORCVAX. The latter two are identical vaccines in terms of strains but have been formulated by different manufacturers using dissimilar methods. Dukoral is a monovalent vaccine based on formaldehyde and heat-killed whole cell (WC) of V. cholerae O1 (classical and El Tor, Inaba and Ogawa) plus recombinant cholera toxin B subunit. However, Dukoral is not licensed for children aged <2 yr who are severely affected by cholera (1, 2). Consequently, the Vietnamese Government developed a WC based OCV (named as ORCVAX) with the assistance of Dukoral's innovator in Sweden. ORCVAX was shown to be safe and immunogenic against the serogruops of O1 and O139. However, the use of ORCVAX internationally was limited since the national regulatory authority of Vietnam is not approved by WHO. Furthermore, the vaccine was not produced according to the standards of Good Manufacturing Practice (GMP) (2).
With the goal of making an ideal low-cost OCV that could be used in cholera-endemic countries, the International Vaccine Institute (IVI), Seoul, Korea in cooperation with VaBiotech reformulated the Vietnamese ORCVAX in 2004 in order to comply with the guidelines of WHO. They replaced the high toxin-producing strain (classical Inaba 569B) with the two strains (Classical Inaba Cairo 48 [heat-inactivated] and Classical Ogawa Cairo 50 [formaldehyde-inactivated]) available in the original Swedish vaccine, and doubled the quantities of lipopolysaccharide (LPS) antigen. To use this reformulated vaccine in cholera endemic countries and enable its procurement by the United Nation (UN) agencies, IVI transferred their OCV manufacturing technology initially to Shantha Biotechnics, India (1, 2). Shantha's OCV (i.e., Shanchol) has already been proved to have a safety and immunogenicity profile (5, 6), and gives considerable protection efficiency against both biotypes and serotypes of O1 and O139 of V. cholerae (7). Shanchol is also indicated for the active immunization against cholera to anyone aged of ≥1 yr, and is eventually obtained WHO pre-qualification in September 2011.
Although it is expected that the total production capacity of IVI reformulated OCVs (Shanchol and mORCVAX) might be 30 million doses per year by 2015, it is not enough to meet the projected demand for the vaccination of human in endemic countries of cholera (8). To address this supply constraint, IVI transferred the OCV manufacturing technology to EuBiologics Co., Ltd. Our manufactured OCV (i.e., study/investigational drug) is fully identical to Shanchol in terms of manufacturing process, quality, composition and route of administration. Although the effectiveness of this study drug against the bio- and serotypes of V. cholerae are expected to be same as Shanchol, we are not certain about this fact as the phase I clinical trial of the study is planned to conduct in Korea, which is a non-endemic country of cholera. On the other hand, the clinical trials of Shanchol were conducted mainly in India and Bangladesh, which are the cholera endemic countries. Furthermore, it is mandatory to assure the safety and immunogenicity profile of our OCV by phase I & III clinical trials in order to fulfill the requirements of WHO, and thus to provide this cholera vaccine for the use in the vaccination programs supported by the international donor agencies in cholera endemic countries. This study reports the assessment of the safety, tolerability and immunogenicity of our OCV in adult Korean male. Upon achieving the successful outcome from this study, phase III clinical trial of this OCV with a large number of subjects will be conducted in the Philippines.
MATERIALS AND METHODS
We conducted an open-label, non-comparative phase I clinical study in order to evaluate the safety, tolerability, and immunogenicity of the investigational product, where no specific control group was considered. The investigational drug (OCV) was orally administrated to 20 healthy adult Korean male volunteers with age of at least 20 yr. The study was conducted at the Clinical Trials Center, Chungnam National University Hospital (CTC, CNUH), Korea from 24 September 2012 to 7 February 2013.
Preparation of study drug/vaccine
The study drug, consists of bivalent WC bulks of formaldehyde-inactivated V. cholerae O139 bacteria and heat- or formaldehyde-inactivated V. cholerae O1 bacteria, was manufactured by processes of fermentation, concentration, washing and inactivation. The formulation of this vaccine has been developed by the IVI, Seoul, Korea considering the fact to meeting the requirements of WHO. The final bulk was prepared in EuBiologics Co., Ltd., Chuncheon, Korea by mixing of five individual bulks obtained through the fermentation of different strains of V. cholerae with phosphate buffer, preservative and purified water. The study drug is a liquid suspension of inactivated V. cholerae and does not contain the B subunit of cholera toxin that is available in Dukoral. Finally, 1.6 mL of final bulk (i.e., a yellow to yellowish color) was filled into each glass vial of 2 mL, which was closed with a rubber stopper covered with an aluminum flip-off seal. The study drug was stored in a refrigerator at 2℃ to 8℃. The detailed composition of this vaccine is mentioned in Table 1. In order to comply with the requirements of WHO, the antigens content (expressed as Lipopolysaccharide ELISA Units, L.E.U.) in OCV were standardized using ELISA specific for V. cholerae O1 and V. cholerae O139 LPS antigens (9). The study drug was also tested for the content of toxin where no detectable toxin (limit of detection 1 ng/mL) was found. The LPS, toxin assays and all other lot release assays were performed at EuBiologics Co., Ltd. The Lot number of study drug is "Euvichol-12001".
Study participants and eligibility
A total of 25 healthy adult male volunteers were screened in this study; and their written consent was taken prior to enrolment. Subjects who satisfied all the inclusion and exclusion criteria of the protocol were finally selected for this clinical trial. Briefly, subjects with history of hypersensitivity to other vaccination, immunization with other vaccine within 2 months, diarrhea or abdominal pain within 1 week, using anti-diarrheal and antibiotics within 2 weeks prior to the start of the study were excluded from the study. However, five of them were failed to meet the eligibility criteria assessed by clinical laboratory tests. Therefore, only 20 subjects were considered at the end.
Study design and method
Twenty screened subjects were admitted to the CTC, CNUH by 4 pm on the day (D-1) before the first dosing day (D0, Visit 2). They were remained fasting from 10 pm on D-1. Drinking water was also prohibited between 1 hr of pre-dose and 2 hr of post-dose. At around 8 am on D0, the study drug (1.5 mL) was orally administered into the subjects. The OCV was personally administered by a sub-investigator (physician) or clinical trial pharmacist, and the dosing was confirmed by an oral examination. Afterward, the vital signs and electrocardiogram (ECG) in subjects were measured as scheduled. At 8 am on D1 (after 24 hr of first dosing), subjects who completed the hospitalization schedule were discharged as they were found to have no safety problem. They were again admitted to the CTC, CNUH by 4 pm on the day (D13, Visit 3) before the second dosing day (D14) and remained fasting from 10 pm on D13. At around 8 am on D14, the OCV was transferred into a syringe and administered orally into the subjects. The vital signs and ECG were measured thereafter. At 8 am on D15 (after 24 hr of second dosing), subjects were discharged after completing the hospitalization schedule as no safety problem was observed. Subsequently, they made outpatient visits to the CTC, CNUH for Visit 4 (D28±2 days) and Visit 5 (D42±5 days) and were performed the above-mentioned tests. The visiting schedule for each subject is given in Fig. 1.
Safety and tolerability assessments
The safety was assessed in subjects who received at least 1 dose of investigational product. The symptoms and signs of adverse events, duration (onset and completion dates), severity (mild, moderate, severe), causal relationship with the study drug, the actions taken for the adverse events, and outcome were recorded by the sub-investigators and principal investigator. In the case of any adverse events those are not demonstrated by the medical diagnosis terms, the symptoms and signs occurred in subjects were recorded by preferred terms (PTs) listed in the Medical Dictionary for Regulatory Activities (MedDRA, version 15.1). They are presented by system organ class (SOC) in the clinical study report. However, the symptoms and signs observed in the subjects prior to the participation in this study were not recorded as an adverse event. The principal investigator or sub-investigators followed the subjects with an adverse event until the event was resolved or abnormal clinical laboratory findings were returned to baseline or the observed change was satisfactorily explained.
Vital signs (blood pressure, pulse rate and body temperature) were measured throughout the study in order to screen the eligibility of subjects as well as on the days of administrating the study drug i.e., after 0.5 hr, 1 hr, 2 hr, 3 hr, 4 hr, and 6 hr of post-dose. 12-lead ECG was conducted in all subjects during screening, just before the pre-dose, and after 6 hr of post-dose. The parameters i.e., ventricular rate (VR) (beats/min), PR interval (msec), QRS duration (msec), and QT/QTc interval (msec) were measured by an autoanalyzer. The results were based on the comprehensive reading findings calculated through the internal algorithm of the autoanalyzer and the clinical findings observed by a physician. Safety of subjects was also assessed by the clinical laboratory tests and physical examination. Blood was collected as scheduled from the subjects using an aseptic technique, and samples were tested by hematology/blood chemistry, blood coagulation test, urine test, serology (Hepatitis B/C & HIV). However, serology was conducted only during screening. All the test results were recorded in the Case Report Form (CRF) with the consent of the principal investigator. The investigator's opinion was also noted in the case of any findings that were outside the reference range. All the analysis was performed at the relevant department of the study site that has been received the quality control certification from the Korean Association of Quality Assurance for Clinical Laboratory. The analytical personnel were well experienced about similar kind of study and performed all the tests according to the standard operating procedures (SOPs) of the study site.
Immunogenicity assessment
The immunogenicity of investigational drug was evaluated by serum vibriocidal assay. In this study, the anti-V. cholerae O1 and O139 antibodies was measured in the sera of subjects administered with the study drug at day 0, day 14, and day 28. Approximately 7 mL venous blood of each subject participated in this study was collected into a plain (non-heparinized) tube. After separating the serum from blood, 0.5 mL aliquots were transferred into sterile micro-centrifuge tubes. All the serum samples were shipped frozen to the IVI and stored -70℃ until the vibriocidal assay was performed. Serum vibriocidal antibodies to V. cholerae O1 (T19479 [El Tor Inaba] and X25049 [El Tor Ogawa]) and O139 (CIRS 134-SR) strains were performed in the laboratory of Clinical Immunology, IVI using a microtiter technique (10, 11). Briefly, the mentioned strains of V. cholerae O1 and O139 were grown in Brain Heart Infusion (BHI) and Luria-Bertani (LB) plus streptomycin (Sm) media, respectively, at 37℃ until reaching mid-log phase. V. cholerae O1 and O139 were harvested by centrifugation, and cells were resuspended in sterile saline (0.85% NaCl) solution and PBS, respectively. Two different mixtures containing the resuspended bacteria and the guinea pig complement (C300-500; Rockland, Gilbertsville, PA, USA) were prepared. The bacterial mixtures were thereafter added to a 96-well microtiter plate (Nunc, Roskilde, Denmark) with the test sera diluted properly by sterile saline and PBS, respectively, and incubated the plates for 60-70 min at 37℃. The initial dilution of all test sera were at 1 in 2.5 for V. cholerae O1 and at 1 in 10 for V. cholerae O139, respectively, and 2-fold serially further diluted.
Human serum (HSQC) and rabbit serum (anti-4260B) were used as the control sera (with known range of vibriocidal titer) for the determination of serum vibriocidal antibodies to V. cholerae O1 and O139 strains, respectively. All the test sera and controls were placed at 56℃ for 30 min to inactivate complement before adding them into the microtiter plates. BHI and 4*LB (+ Sm) media were added to each well of microtiter plates and incubated at 37℃ for 3-5 hr in order to determine the vibriocidal antibodies against V. cholerae O1 and O139, respectively. Finally, the optical densities of resulting suspensions were measured at 600 nm with a microplate reader (Spectramax 190, Molecular Device, Sunnyvale, CA, USA). The titers of vibriocidal O1 and O139 antibodies were defined as the reciprocal of the highest dilution of serum that gave complete inhibition of visible growth of V. cholerae O1 and the dilution of serum that caused 70% killing V. cholerae O139, respectively. The serum vibriocidal antibody titers were determined with mean of the two tests and the assay was repeated whenever more than two-fold difference was noted between the results of duplicates. The statistical analysis (e.g., geometric mean, standard deviation [SD], min, max, median, 95% confidence interval [CI] for antibody titers) was conducted to compare the antibody titers and fold increase in regards to the baseline titers. Vibriocidal titers <2.5 for V. cholerae O1 and <20 for V. cholerae O139 were considered as 1.25 and 10, respectively, for the statistical analysis. Antibody titers in sera collected on day 14 and 28 were divided by the baseline titers (D0) in order to obtain the fold-rise. Seroconversion was defined as a four-fold or greater increase in titer between pre- and post-vaccination sera.
Data management and statistical analysis
The data management for this study was implemented according to the guidelines of International Conference on Harmonization - Good Clinical Practice (ICH-GCP) and Korea Good Clinical Practice (KGCP). The adverse events and various test findings were reviewed, incorporated and comprehensively judged by a sub-investigator. For safety assessment, the probability of observing at least 1 adverse event with the incidence of 15% in 20 subjects is 95%. In the case of antibody titers, geometric mean, SD, min, max, median and 95% CI are calculated. The means of titers are calculated as geometric mean titer (GMT), and after log-transformation when necessary, analyzed and exponentiated. CRFs and all the relevant data were monitored by the study coordinator as designated by the EuBiologics Co., Ltd.
Ethics statement
The protocol for this clinical study (UBC101) was also approved by the Korea Food and Drug Administration (KFDA) and institutional review board (No. CNUH-2012-08-012) of the Clinical Trials Center, Chungnam National University Hospital on 31 July, 2012 and 29 October 2012, respectively. This study was registered with the Clinical Trials Registry (http://clinicaltrials.gov/, Identifier: NCT01707537).
RESULTS
Safety assessment
The safety of study drug was assessed based on the adverse events measured by the clinical laboratory tests, vital signs, ECGs, and physical examinations in all the subjects who took part in this study. Since this drug is orally administered unlike other vaccines, adverse events were not classified as local and systemic events. However, a total of 7 adverse events occurred in 6 subjects i.e., 2 events of headache, 1 event each of toothache, blood creatine phosphokinase increase, liver function test abnormality, musculoskeletal pain, and tooth extraction. Based on severity, toothache and blood creatine phosphokinase increase were considered as Grade 3, tooth extraction was Grade 2, and the rest of the events were Grade 1. The causal relationship for 2 events of headache and 1 event of other adverse events was designated as 'Probably related' and 'Possibly related', respectively. For other events not mentioned above, the causal relationship was 'Probably not related'. However, no serious adverse event occurred.
Vital signs (blood pressure, pulse rate and body temperature) were measured in each subject from the start of screening and during the study according to the planned schedule. However, no clinically relevant change was found in systolic/diastolic blood pressure and pulse rate while reviewing individually. The parameters of ECG (VR, PR interval, QRS duration, QT interval, and QTc interval) measured at each point were compared with the baseline data. However, there was no difference found before/after vaccination, and no clinically significant change (for example, arrhythmia) was observed from the comprehensive judgment based on the automatic ECG tracing and investigator's findings. In addition, all subjects had clinical laboratory tests during screening, Visit 4 and Visit 5. No clinically relevant change was observed in hematology, blood chemistry, blood coagulation test, and urology parameters before/after vaccination. Physical examinations were also performed during the study. However, no clinically meaningful change was noted, suggesting that there is no major safety problems related to this investigational drug.
Immunogenicity assessment
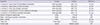
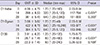
The vibriocidal antibody titers to 3 different strains of V. cholerae measured prior to the first dose (baseline, D0), before the second dose (D14), and 14 days after the second dose (D28) of OCV were ranged from <2.5-5,120, <2.5-10,240, and <2.5-480 for O1 Inaba, O1 Ogawa and O139, respectively. The geometric mean serum vibriocidal antibody titers (GMT), 95% CI and number of subjects were also measured at the above time points, which are presented in Fig. 2. In the case of all antibodies, a noticeable increase of GMT was observed in sera collected at D14 and D28 as comapred to D0. The descriptive statistics of antibody titers measured at the above-mentioned days are presented in Table 2. The antibody titers to V. cholerae O1 Inaba, O1 Ogawa, and O139 measured on D14 and D28 were divided by the baseline titers (D0) in order to obtain the geometric mean fold rise (GMF-rise). The antibody titers from baseline value measured in this study ranges from 1-4,096 for O1 Inaba, 1-8,192 for O1 Ogawa, and 1-384 for O139. When the baseline titer was <2.5, it was substituted with 1.25. Fig. 3 shows the GMF-rise from baseline titer to V. cholerae O1 Inaba, O1 Ogawa, and O139 measured on D14 and D28. The descriptive statistics of GMF-rise to mentioned 3 strains of V. cholerae is mentioned in Table 3.
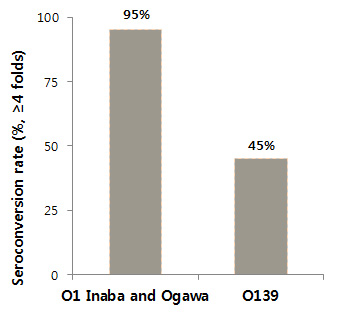
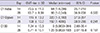
We calculated the percentages of subjects seroconverted (≥ 4-fold rise in serum vibriocidal titers) on day 14 and 28 after the study drug administration. In the case of vibriocidal antibodies against both O1 Inaba and O1 Ogawa strains of V. cholerae, 19 subjects (95%) showed a ≥4 fold increase on D28. The number of subjects with a ≥4 fold increase against V. cholerae O139 was 10 (50%) and 9 (45%) on D14 and D28, respectively (Table 4). The statistical analysis was also conducted to compare the antibody titers, fold rise from baselines and the titers between the dosing points. In the case of all three antibodies, the geometric mean titers (GMT) against V. cholerae measured on D14 showed a statistically significant (P value, <0.001) increase from the baseline, whereas no statistical difference was obtained in antibody titers measured on D28 from that of D14 (Table 2). The GMF-rise on D28 also exhibited no statistically significant difference from the GMF-rise on D14 (Table 3), indicating that the antibody titers significantly increased on D14 and maintained at a constant level till D28.
DISCUSSION
This study confirms that the killed whole cell OCV co-developed by IVI and EuBiologics Co., Ltd. is safe, well-tolerated, and immunogenic. No serious adverse event or safety problem was observed in 20 healthy adult Korean males while administering two oral doses at a 2 week-interval. Although a total of 7 adverse events occurred in 6 subjects, we found that the subject with Grade 3 toothache had already been prescribed for Noriss Tablet 125 mg (clonixin lysinate). In the case of subject with Grade 3 blood creatinine phosphokinase increase and Grade 1 liver function abnormality, the events might have occurred due to weight training. In the case of subject who was reported with Grade 1 tooth extraction, he did this surgery before joining in the clinical study; and the sub-investigator was not informed about this matter. In principle, no drugs other than the protocol-specified OCV were used during this clinical trial. Concomitant medication, when necessary for the treatment of an adverse event, was given and the reasons of their using were recorded in the CRF with duly signed by the principal investigator. If a drug had been arbitrarily taken by any subject without the consent of the principal investigator, the relevant subject was not considered in this study. However, we did not include a placebo group and a relatively small number of subjects were involved in this clinical trial. The comparative safety studies between our developed OCV and Shanchol will be conducted through Phase III clinical trial that has already been planned in the Philippines.
We found that our study drug induces significant vibriocidal responses after administrating 2 doses of OCV to subjects in Korea, a cholera non-endemic country. A considerable increase in GMT to V. cholerae O1 Inaba, O1 Ogawa, and O139 was observed in sera collected at day 14 and 28. In addition, the GMT-rises from baseline at day 14 and 28 were almost similar and ranged between 75-94, 108-115, and 7-8 fold higher for O1 Inaba, O1 Ogawa and O139, respectively. Alike GMF-rise, the percentages of subjects seroconverted on day 14 and 28 were almost similar. In this study, 90%-95% and 45%-55% of subjects seroconverted on day 14 and 28 against V. cholerae O1 and O139, respectively. It has been hypothesized that the first dose of OCV stimulates an immune response in the intestinal mucosa, which may inhibit the immune response of second dose. As high vibriocidal antibody titers are usually obtained after administrating of first dose, further increases may not be possible due to second dose. These phenomena have been observed in the case of previous clinical studies conducted with the similar kind of oral cholera vaccine where high vibriocidal titers diminished further immune responses (5, 12, 13).
Our results are comparable to or higher than the findings (V. cholerae O1 [90.5%] and O139 [11.1%]) obtained through the clinical study in Solna, Vietnam (9) and higher than the findings (53% and 10%, respectively) obtained through the clinical study in Kolkata, India (6). Such a difference is speculated to be attributable to the relatively low seroconversion rate in people living in the regions with cholera epidemics due to a high baseline titer and the absence of cholera epidemics in Korea over the past 20 yr.
We observed a lower immune response to V. cholerae O139 than that of V. cholerae O1. Approximately 95% of subjects exhibited a 4-fold or greater increase in serum antibody against both strains of V. cholerae O1 Inaba and Ogawa, whereas the percentage of seroconversion in the case of V. cholerae O139 was measured only 45%. Similar kinds of data have been found in previous clinical studies conducted with the mORCVAX and Shanchol. An epidemiological point of view, V. cholerae O139 is found only in Bangladesh and Kolkata in 1992, and caused extensive epidemics in some parts of southern Asia (1). However, there has not been found any report of causing cholera due to O139 since the 1990s. It has been reported that the lower immune responses to O139 may be occurred because of using much lower O139 antigenic content in vaccine as compared to O1 (14, 15). In addition, it has been reported that the two groups of V. cholerae (O1 and O139) comprising our OCV have LPS that differ in composition and amounts (16, 17). V. cholerae O139 possesses both LPS and capsular polysaccharide (CPS) present in the ratio of 1: 2, and LPS being the minor component (17). On the other hand, V. cholerae O1 does not possess CPS.
As this is a study of exploring the tolerability, safety and immunogenicity of oral cholera vaccine, it is different from the typical clinical studies at least in aspect of statistical hypothesis testing. We have already reported that the composition of our OCV is similar to Shanchol as the manufacturing technology of both vaccines has been transferred by IVI. Although the formulation of our study drug is similar to Shanchol, this study showed a different immunogenicity profile from that of obtained by Mahalanabis and his colleagues in Kolkata, India (6). This dissimilarity might be occurred due to the geographical differences of subjects considered in both studies. Our study was performed in Korea, a cholera non-endemic, whereas Kolkata is belonged to a cholera endemic country. In order to evaluate this finding further, we are presently conducting Phase III clinical study of OCV in the Philippines where Shanchol will be used as a comparator drug.
In conclusion, our newly developed vaccine is safe and tolerable in healthy adult males in Korea and achieved a suitable level of antibody increase against V. cholerae. A phase III clinical trial for this vaccine is currently ongoing in the Philippines. If we obtain the results of Phase III safe and effective against V. cholerae, this OCV will give an opportunity to prevent the disease in cholera endemic countries as well as to control the cholera outbreak throughout the world.



 XML Download
XML Download