

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is a major cause of morbidity and mortality in hospitalized patients. PE is the third most common fatal vascular disorder following coronary artery disease and cerebrovascular accident (1); it is also the leading cause of preventable hospital death and a major cause of maternal mortality (2, 3). In addition to the clinical impact of VTE on morbidity and mortality, the economic burden of the disease is considerable (4). Thus, VTE is a major public health concern in developed countries.
For the treatment of VTE, thromboprophylaxis has been recommended based on the four following factors: the high incidence of VTE in hospitalized patients; the difficulty of early diagnosis due to vague symptomatology; the cost-effectiveness of medical prophylaxis; and the high mortality of PE without early diagnosis and prompt management. Furthermore, data from numerous clinical trials have demonstrated that appropriate prophylaxis to prevent VTE is safe and effective in both surgical and medical patients. Based on these results, several evidence-based guidelines have been proposed for VTE prevention (5-8). Recently, the American College of Chest Physicians (ACCP) issued the evidence-based clinical practice guideline for antithrombotic therapy and prevention of thrombosis, which provides improved guidelines in an American setting (9th edition) (6).
The incidence of VTE is lower in the Korean population than in the Caucasian population; however, it appears to be rapidly increasing in response to the widespread adoption of the Western lifestyle. Additionally, the large proportion of the Korean population is comprised of the elderly, and advanced age has been recognized as a risk factor for VTE (9). After we proposed the first Korean Guideline for the Prevention of VTE in 2010 (10), awareness of the significance and risk of VTE has been increasing among both the public health community and physicians in Korea. However, the previous guidelines were not based on clinical evidence, but on a consensus of the opinions of the expert panel of the Korean Society of Thrombosis and Hemostasis with references of the second edition of the Japanese guidelines for the prevention of VTE, and the ACCP guidelines (8th edition).
We recently revised the Korean guidelines for VTE prevention based on the Health Insurance Review and Assessment Service (HIRA) database (11) and new ACCP guidelines (6). These guidelines were established to reflect Korean VTE epidemiology and serve as practical recommendations for physicians in Korea. They focus on patients undergoing major surgery and are intended to assist physicians in balancing the risks of death and morbidity from VTE against the complications and disadvantages of prophylaxis. Unfortunately, the extended content of these guidelines can be too much complex for physicians. This article represents a simplified, practical version of the revised guidelines that provide an overview of the key issues that are relevant to physicians. These guidelines stratify patients into 4 risk groups (very low, low, moderate, and high) according to the actual VTE risk and recommend an optimal VTE prophylaxis for each group.
GENERAL RECOMMENDATIONS
Risk stratification
The VTE risk of all hospitalized patients should be assessed using an accepted risk stratification method. Additionally, the method for risk stratification should be simple, efficient, and cost-effective. Classic risk factors for VTE include cancer, surgery, prolonged immobilization, fractures, puerperium, paralysis, use of oral contraceptives, antiphospholipid antibody syndrome, and other acquired or hereditary thrombophilic conditions. Most hospitalized patients have at least one risk factor for VTE, and decisions regarding the risk of VTE should include considerations of current and future thrombotic risks (12).
The ACCP Evidenced-Based Clinical Practice Guidelines (9th Edition) for the Prevention of VTE suggests a risk stratification model based on the symptomatic VTE rate (13). This model classifies patients into very low risk (<0.5%), low risk (0.5%-1.5%), moderate risk (1.5%-3.0%), and high risk (>3%) groups, depending on the symptomatic VTE rate. Because the ultimate target of VTE prevention is symptomatic VTE, this approach is both simple and practical. Thus, we used this risk-stratification method in the development of our revised guidelines.
Non-pharmacologic thromboprophylaxis
Ambulation increases venous blood flow and reduces venous stasis. Early ambulation is a simple measure that should be applied as standard practice to prevent VTE in all patients. Mechanical prophylaxis, including graduated compression stocking (GCS) and intermittent pneumatic compression (IPC), focuses on reducing venous stasis and blood stagnation by promoting venous blood flow through external compression. Mechanical methods have an additional advantage in that they are not associated with a risk of bleeding. Mechanical prophylaxis is recommended as an alternative to or in combination with pharmacological prophylaxis. The benefits of decreasing VTE risk were similar irrespective of the mechanical method used.
Pharmacologic thromboprophylaxis
Pharmacological prophylaxis is both reasonable and cost-effective and is therefore recommended as the initial form of prophylaxis in most patients without a high risk of bleeding. Effective pharmacological prophylaxis may include low-molecular-weight heparin (LMWH; 20-100 U/kg (0.2-1 mg/kg) subcutaneously [SC] daily), low-dose unfractionated heparin (LDUH; 5,000 U every 8-12 hr SC), fondaparinux (2.5 mg SC daily), rivaroxaban (10 mg orally daily), dabigatran (150 mg orally each day), apixaban (2.5 mg every 12 hr orally), aspirin (100 mg orally each day), and warfarin (daily doses to maintain an international normalized ratio [INR] of 1.5-2.5) (Table 1). The duration of prophylaxis depends on the perceived benefits of anticoagulation versus the risks of bleeding and overall cost. Currently, dabigatran and apixaban are not approved by the Korean FDA for thromboprophylaxis.
Stratification of VTE risk in hospitalized patients
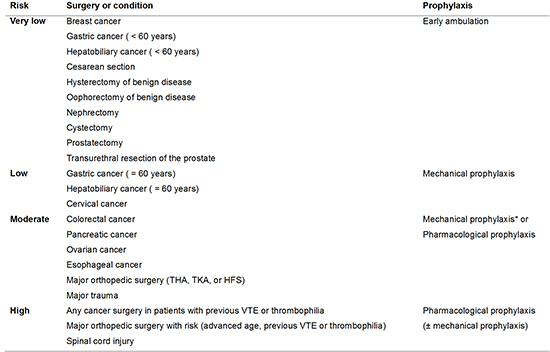
Based on the risk stratification for individual patients, the risk of VTE can be stratified from very low to high (Table 2). However, the prophylactic treatment selected is not solely procedure-specific, but depends on the individual's level of risk based on careful risk assessment. We defined patients at very low risk as those undergoing surgery for breast cancer, gastric cancer (<60 yr), or hepatobiliary cancer (<60 yr); cesarean section, hystectomy, or oophorectomy for benign disease; and transurethral resection of the prostate, nephrectomy, cystectomy, or prostatectomy for benign or malignant disease. For patients undergoing gastric cancer surgery (≥60 yr), hepatobiliary cancer surgery (≥60 yr), or hysterectomy (cervical cancer), we define these patients as low risk. Moderate-risk patients are defined as those undergoing surgery for colorectal, pancreatic, ovarian, or esophageal cancer; total hip arthroplasty (THA); total knee arthroplasty (TKA); or hip fracture surgery (HFS). If the moderate risk patients have an addition risk factor, including previous VTE or thrombophilia, we define these patients as high-risk patients.
Thromboprophylaxis according to risk stratification
We recommend the selection of an optimal prophylactic treatment based on VTE risk levels. Generally, mechanical prophylaxis is recommended for low or moderate risk patients, and pharmacological prophylaxis is recommended for moderate or high-risk patients. For patients with very low risk of VTE, we recommend early ambulation or exercise only; for patients with low risk of VTE, we recommend mechanical prophylaxis with GCS or IPC; for patients with moderate risk of VTE, we recommend mechanical or pharmacological prophylaxis; and for patients with high risk of VTE, we recommend pharmacological prophylaxis with or without a mechanical method.
Grade of recommendation
We adopted the quality of evidence and strength of recommendations from the 9th ACCP guidelines (13). The grade of recommendation indicates the strength of the guideline and the degree of consensus agreement. We define the Grade 1A as a strong recommendation with high-quality evidence; Grade 1B as a strong recommendation with moderate-quality evidence; Grade 1C as a strong recommendation with low- or very-low-quality evidence; Grade 2A as a weak recommendation with high-quality evidence; Grade 2B as a weak recommendation with moderate-quality evidence; and Grade 2C as a weak recommendation with low- or very-low-quality evidence (Table 3).
GENERAL SURGERY
The principles of risk stratification for general surgery are based on the type of surgery (cancer or non-cancer), the type of cancer (gastric, colorectal, hepatobiliary, or breast), age (<60 yr, and ≥60 yr), and the presence of previous VTE. According to these principles, patients were classified into four risk groups.
We define the very-low-risk group as patients scheduled for non-cancer surgery or breast cancer surgery and patients (<60 yr) scheduled for gastric or hepatobiliary cancer surgery. For very-low-risk patients, we recommend early and frequent ambulation (Grade 2C). For patients (≥60 yr) undergoing gastric or hepatobiliary cancer surgery, we recommend mechanical prophylaxis with GCS or IPC (Grade 2C). We recommend mechanical prophylaxis with GCS or IPC for patients undergoing colorectal or pancreatic cancer surgery, but pharmacological prophylaxis with LMWH or LDUH may also be used for patients with a low risk of bleeding (Grade 2C). If patients undergoing any cancer surgery have an additional risk factor, including previous VTE or thrombophilia, we recommend pharmacological prophylaxis with LMWH or LDUH (Grade 1B) (Table 4).
ORTHOPEDIC SURGERY
Patients undergoing major orthopedic surgery, which includes total hip arthroplasty (THA), total knee arthroplasty (TKA), and hip fracture surgery (HFS), are at particularly high risk for VTE. Although routine prophylaxis is adopted these high-risk patients, the rate of clinically overt VTE in these patients remains at approximately 1.8% (14). Recently, a prospective study reported that the rate of symptomatic VTE is 1.5% in Asian patients who have a major orthopedic surgery without VTE prophylaxis (15). The HIRA database also revealed that the rate of symptomatic VTE is 1.08% for TKA, 0.98% for THA, and 1.60% for HFS. Based on these results, we classified the patients scheduled for major orthopedic surgery into the moderate-risk group for VTE.
We recommend pharmacological or mechanical prophylaxis for patients scheduled for major orthopedic surgery for at least 10-14 days (Grade 2A). We recommend pharmacological prophylaxis (LMWH, fondaparinux, dabigatran, apixaban, rivaroxaban, LDUH, warfarin, or aspirin) for patients undergoing TKA and THA, and mechanical prophylaxis for patients with a risk of bleeding. For patients undergoing HFS, we recommend pharmacological (LMWH, fondaparinux, LDUH, warfarin, or aspirin) or mechanical prophylaxis. For all patients undergoing major orthopedic surgery, we recommend mechanical prophylaxis (Grade 2B). If the patients have an additional risk factor, including advanced age, general anesthesia, previous VTE, or cancer, we recommend pharmacological prophylaxis (Grade 2B). Early ambulation should be encouraged for all patients after surgery (Grade 1A). Routine screening is not recommended in these patients (Grade 1A) (Table 5).
NEUROSURGERY
Neurosurgical patients are at an increased risk of both thrombosis and bleeding. The incidence of DVT and subsequent PE in neurosurgery patients has been reported to be as high as 25%, and the PE mortality rate has been reported to range from 9% to 50% (16, 17). The important risk factors in neurosurgical surgery are the type of surgery (cranial, spinal, or vascular), duration of surgery, cancer, infection, immobilization, venous stasis, chronic lower extremity swelling, lower extremity trauma, advanced age, CHF, obesity, and sleep apnea. The HIRA database revealed that the rate of DVT is 0.14% and the rate of PE is 0.24% in patients who have undergone brain tumor surgery. We recommend mechanical prophylaxis for all neurosurgery patients (Grade 2C). If the patients have an additional risk factor, including advanced age, female, previous VTE, or brain cancer, we selectively recommend pharmacological prophylaxis (Grade 2C). Patients should be closely monitored for signs of bleeding during pharmacological prophylaxis (Grade 1A).
UROLOGIC SURGERY
The important risk factors for the development of VTE in urological surgery patients are advanced age, obesity, cancer, and previous VTE. The HIRA database shows that the rate of VTE is 0.35% in kidney cancer patients who underwent nephrectomy, 0.17% in bladder cancer patients with cystectomy, 0.22% in prostate cancer patient with prostatectomy, and 0.06% in prostate hyperplasia patients who received transurethral resection of the prostate. Based on these results, we classified patients with these urologic surgeries into the very-low-risk group.
We recommend early and frequent ambulation for transurethral resection of the prostate (Grade 2A). For cancer patients undergoing nephrectomy, cystectomy, and prostatectomy, early and frequent ambulation is recommended (Grade 2B). For patients with previous VTE or thrombophilia and elderly patients (≥60 yr) scheduled for major urologic surgery under general anesthesia, we recommend mechanical prophylaxis or pharmacological prophylaxis (LMWH or LDUH) or a combination of both pharmacological and mechanical prophylaxis (Grade 2B).
OBSTETRIC AND GYNECOLOGIC SURGERY
The incidence of VTE is higher during pregnancy and may occur at any stage of pregnancy or in the weeks following delivery. The risk factors for VTE in pregnant women include previous VTE, a family history of VTE, presence of anti-phospholipid antibody, age ≥40 yr, prolonged bed rest, placenta previa, Cesarean section, and lower-extremity varicosities. The HIRA database shows that the incidence of pregnancy-associated VTE is 0.82 per 10,000 deliveries (18).
We suggest that a thrombosis risk assessment be carried out in all women during pregnancy (Grade 1A). Early ambulation should be encouraged for all postpartum women (Grade 1A). For postpartum women without any risk factor for VTE, we do not recommend mechanical or pharmacological prophylaxis regardless of delivery mode (Grade 2A). Further, we do not recommend routine thrombophilia testing (Grade 1B). For pregnant women with hereditary thrombophilia, positive anti-phospholipid antibody, or previous VTE, antepartum plus postpartum prophylaxis is recommended (Grade 1B). Warfarin is contraindicated during pregnancy (category X) (Grade 1A) (19). However, warfarin can replace LMWH after delivery for postpartum thromboprophylaxis (20) (Grade 1B).
The risk factors for VTE associated with gynecologic surgery are giant uterine myoma, previous surgery for an ovarian tumor, ovarian cancer, uterine or cervical cancer, severe intrapelvic adhesions, ovarian hyperstimulation syndrome, hormonal therapy, and particularly protracted lymph node dissection requiring transfusion (21). The HIRA database revealed that rates of VTE are 0.02% for hysterectomy associated with benign disease, 0.59% for hysterectomy associated with cervical cancer, 0.05% for oophorectomy associated with benign disease, and 1.21% for ovariectomy associated with ovarian cancer. We recommend early and frequent ambulation for very-low-risk patients (hysterectomy or oophorectomy with benign disease) (Grade 2B). For low-risk patients undergoing hysterectomy with cervical cancer, mechanical prophylaxis is recommended (Grade 2B). For moderate-risk patients undergoing oophorectomy with ovarian cancer, we recommend pharmacological prophylaxis with LMWH or LDUH (Grade 2B). If moderate-risk patients are at risk of bleeding during anticoagulation therapy, we recommend mechanical prophylaxis (Grade 2B).
MAJOR TRAUMA AND SPINAL CORD INJURY
VTE can cause significant morbidity in patients experiencing major trauma and occurs in up to 50% of patients without prophylaxis (22). Previous studies have identified several risk factors for VTE including age, male gender, pelvic fractures, lower extremity fractures, traumatic brain injury, increased Injury Severity Score, chest injury, operative interventions, and acute spinal cord injury (SCI) (23, 24). We recommend mechanical or pharmacological prophylaxis for major trauma patients (Grade 2C). If the patients have a high risk of bleeding (intracranial bleeding, lung injury, liver injury, spleen injury, and retroperitoneal bleeding associated with pelvic bone fracture), mechanical prophylaxis (GCS or IPC) should be implemented (Grade 2C). When the risk of bleeding has been eliminated, we recommend that pharmacologic prophylaxis with LDUH or LMWH be substituted for the mechanical prophylaxis (Grade 2C). Usually, pharmacological prophylaxis can be used within 36 hr of trauma (Grade 2C). We recommend that pharmacological prophylaxis be continued for 3 months following trauma (Grade 2C).
Patients with SCI have been shown to be at higher risk for DVT than many other trauma patients. Overall, the incidence of DVT without prophylaxis is estimated to be 40% based on a meta-analysis of DVT in patients with acute spinal cord injury (25). Moreover, prevention of VTE is important because PE is a leading cause of death in SCI patients (26). We recommend pharmacological prophylaxis with LDUH, LMWH, or warfarin for SCI patients without a risk of bleeding (Grade 2C). If the patient is contraindicated for pharmacological prophylaxis, mechanical prophylaxis (GCS or IPC) should be implemented (Grade 2C). We recommend that prophylaxis be continued for 3 months (Grade 2C); however, the duration can be decreased after ambulation (Grade 2C). If patients are complicated with spinal or epidural hematoma, mechanical prophylaxis (GCS or IPC) should be implemented for several days (Grade 2C). When the risk of bleeding has decreased, we recommend that pharmacologic prophylaxis (LDUH or warfarin) be substituted for the mechanical prophylaxis or be combined with mechanical prophylaxis (Grade 2C).
NEURAXIAL ANESTHESIA
Neuraxial anesthesia is a comprehensive term used for spinal, epidural, and caudal blocks. The risk for the development of spinal or epidural hematoma may be elevated by the concomitant use of anticoagulants and antiplatelet agents (27, 28). The established risk factors for spinal or epidural hematoma after neuraxial blockade include an underlying hemostatic disorder, an anatomically deformed vertebral column, traumatic insertion of a needle or catheter, repeated insertion attempts, concomitant anticoagulation, continuous use of epidural catheters, and old age (29, 30).
We recommend against concomitant administration of medications affecting hemostasis, such as antiplatelet drugs or warfarin, during anticoagulation with LMWH or UFH (Grade 1B). The presence of blood during needle and catheter placement does not necessitate postponement of surgery. We suggest that initiation of LMWH therapy in this setting should be delayed for 24 hr postoperatively and that this consideration be discussed with the surgeon (Grade 2C). For patients receiving prophylactic doses of LMWH, we recommend a delay of at least 10-12 hr after the time of needle insertion (Grade 1C). For patients receiving therapeutic doses of LMWH, we recommend a delay of at least 24 hr before the time of needle insertion (Grade 1C). For patients receiving twice-daily dosing of LMWH, the first dose of LMWH should be administered no earlier than 24 hr postoperatively (Grade 1C). If the epidural catheter is left indwelling overnight, administration of LMWH should be delayed for 2 hr after catheter removal (Grade 1C). We recommend that the anticoagulant therapy be discontinued (ideally 4-5 days before the planned procedure) and the INR must be normalized before initiation of neuraxial block (Grade 1B). As prophylaxis with warfarin is initiated, we suggest that neuraxial catheters should be removed when the INR is less than 1.5 (Grade 2C). Cyclooxygenase-2 inhibitors have a minimal effect on platelet function and should be considered in patients who require anti-inflammatory therapy in the presence of anticoagulation (Grade 2C). We recommend an interval between the last dose of clopidogrel or aspirin and neuraxial blockade of at least 7 days (Grade 1C).
MEDICAL CONDITIONS
Hospitalized patients with acute medical conditions are at a significant risk of VTE. Previous studies have shown that in the absence of prophylaxis, a significant proportion of acutely ill medical patients develop VTE, with DVT and PE incidence of 10-30% in general medical patients (31-33). Despite extensive studies in medical patients, the morbidity and mortality of VTE remains significant. The risk of VTE was determined by assessing the probability of VTE in acutely ill medical patients according to predisposing risk factors (age>70 yr, obesity, long-term immobility, tobacco use, varicosities, dehydration, estrogens, cancer, previous DVT, paraplegia, congenital or acquired thrombophilia, and inflammatory bowel disease) and acute medical illnesses currently under treatment (chronic obstructive pulmonary disease exacerbation, mechanical ventilator therapy, infection, congestive heart failure, and cerebrovascular attack) (34-36).
We recommend routine assessment for VTE risk and bleeding risk in all acute medically ill patients (Grade 1A). The physician should decide the optimal VTE prophylaxis according to the number of VTE risk factors, level of VTE risk, and risk of bleeding (Grade 2C). For acutely ill medical patients who have one or more additional risk factors, including congestive heart failure, myocardial infarction, cerebrovascular attack, metastatic cancer, or previous VTE, we recommend pharmacological prophylaxis or mechanical prophylaxis (Grade 2C). The majority of patients admitted to the intensive care unit have multiple risk factors for VTE. These patients should be routinely assessed and offered pharmacological prophylaxis or mechanical prophylaxis (Grade 2A). For metastatic cancer patients who have previous VTE or thrombophilia, we recommend pharmacological prophylaxis (Grade 2A). Mechanical prophylaxis can be used when there is a contraindication to anticoagulation (Grade 1A) (Table 6).
SUMMARY
These guidelines emphasize strategies for the prevention of VTE in Korean patients experiencing surgery, pregnancy, trauma, cancer, and acute medical illness. Based on VTE risk factors (age, immobility, history of VTE, co-morbid illness, and type of surgery or trauma), patients can be stratified into very-low-, moderate-, and high-risk groups. For high-risk patients (any cancer surgery with previous VTE or thrombophilia, major orthopedic surgery with additional risk, and SCI), pharmacological prophylaxis is recommended. Mechanical prophylaxis should be used primarily in patients with a high risk of bleeding. For moderate-risk patients (colorectal or pancreatic cancer surgery, major orthopedic surgery without additional risk, and major trauma), prophylaxis with a mechanical method (GCS and/or IPC) or a pharmacological method can be used. For low-risk patients (gastric cancer surgery [≥60 yr], hepatobiliary cancer surgery [≥60 yr], and hysterectomy [cervical cancer]), mechanical prophylaxis is recommended. For very-low-risk patients, early and frequent ambulation is the only recommended prophylactic treatment. In conclusion, this article outlines the revised Korean guidelines issued for primary VTE prevention and provides a useful reference for clinicians. These guidelines must be updated based on results of well-controlled studies conducted in Korea. Our guidelines aim to define and clarify an optimal strategy for VTE prevention for patients with VTE risk; however, the ultimate decision should be individualized and determined by the physician.





 XML Download
XML Download