

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Rituximab-Cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) is considered a standard treatment of diffuse large B-cell lymphoma (DLBCL). Although DLBCL is a clinically and genetically heterogenous group of diseases, a recently updated follow-up analysis confirmed that DLBCL is a potentially curable disease with R-CHOP chemotherapy (1). Therefore, the effort to minimized treatment-related morbidity and mortality is the one of the most important issues in treating patients with DLBCL.
Febrile neutropenia (FN) is the most serious hematologic toxicity of chemotherapy containing myelotoxic agents. The prompt administration of empiric antibiotics is crucial in patients with FN because infection can progress rapidly (2). Prolonged neutropenia and FN increase not only disease-related morbidity and mortality but also medical costs (3). Moreover, FN can delay and reduce chemotherapy delivery (4). Since chemotherapy delivered at less than 90% of the planned relative dose intensity (RDI) has been associated with impaired outcomes in aggressive DLBCL treated with CHOP (4), prophylaxis and the proper management of neutropenia and FN to maintain planned doses of chemotherapy during chemotherapy cycles seem inevitable to guarantee a favorable outcome of DLBCL treated with R-CHOP.
Variable degrees (7%-65%) of FN have been reported among the patients treated with CHOP±R chemotherapy (5, 6). The National Comprehensive Cancer Network (NCCN) and European Organization for Research and Treatment of Cancer (EORTC) guidelines assess the risk of FN considering patients' own risk factors and the chemotherapy regimen itself and then recommend primary prophylaxis with granulocyte colony-stimulating factor (G-CSF) in patients with a >20% risk of FN (7). According to the guidelines, an R-CHOP-21 regimen itself is an intermediate risk for FN (7). Therefore, it is important to recognize what are the high-risk features of FN in patients treated with an R-CHOP regimen. Older age, poor performance status, advanced disease, comorbidities, low baseline blood cell counts, and low body surface area/body mass index are well-known general risk factors of FN based on studies with variable chemotherapy regimens (8). However, a few studies have been reported regarding risk factors of FN in patients treated with CHOP specifically (9, 10, 11). Moreover variable patient risk factors for FN were not identical among studies. There was only one large observational study including DLBCL patients treated with R-CHOP in which the researchers analyzed the risk factors of FN (12). Even in that study, because many patients had already received primary G-CSF prophylaxis, the risk factors for FN could not be identical to those of patients without primary G-CSF prophylaxis. Although the reported adverse events of CHOP and R-CHOP chemotherapy were similar, it is unclear whether risk factors of FN obtained mainly from studies with non-Hodgkin's lymphoma (NHL) patients treated with CHOP could be applied directly to patients treated with an R-CHOP regimen. In addition, all previous studies were conducted with Western populations. Therefore, in this study, patterns of neutropenia and risk factors of FN specific to an R-CHOP regimen in Asian DLBCL patients were analyzed.
MATERIALS AND METHOD
Patients
A total of 181 patients who were diagnosed with DLBCL and treated with R-CHOP chemotherapy at Ajou University Hospital between January 2004 and December 2013 were analyzed. Patients received at least 4 cycles of R-CHOP chemotherapy with or without G-CSF support in this study. The R-CHOP regimen (rituximab 375 mg/m2, cyclophosphamide 750 mg/m2, doxorubicin 50 mg/m2, vincristine 1.4 mg/m2, all on day 1 and prednisone 40 mg/m2 daily for 5 days) was administered every 3 weeks. Considering compliance of patients, extending interval of each chemotherapy-cycle to 4 week was allowed in our protocol. Blood samples for laboratory testing were collected on day 1. Revisiting outpatient clinic on day 8 was mandatory to all patients. On day 8, blood samples and body temperature of patients was collected. Prophylactic antibiotics and G-CSF were not used. All FN patients was admitted to a hospital and had at least two aerobic and anaerobic blood cultures before receiving antibiotics. In FN patient, G-CSF (filgrastim, 5 µg/kg) was administered until recovery of absolute neutrophil count (ANC) occurs.
Independent variables and operational definition
Demographic and clinical characteristics of all patients included age, sex, height, weight, body-surface area (BSA), comorbid conditions (which was categorized by the comorbidity component of the Chalson Comorbidity Index), a history of previous cancer diagnosis and treatment, hepatitis B virus (HBV) carrier status, and bone marrow involvement; they were retrieved from the medical record database of hospital. In addition, baseline complete blood cell count (CBC), lactate dehydrogenase (LDH), and albumin levels were collected. Age was dichotomized as less than 65 or ≥65 yr. BSA was categorized as less than 1.9 m2 and ≥1.9 m2. ECOG performance status was categorized as less than 2 or ≥2. Comorbid condition, HBV carrier status, and bone marrow involvement were categorized as either present or absent. Serum LDH level (reference range: 100-200 U/L) was categorized as ≤200 or more than 200 U/L, and serum albumin level was classified as ≤3.5 or more than 3.5 mg/dL. Baseline ANC was categorized as less than 1,500/µL and ≥1,500/µL. Baseline hemoglobin was categorized as <12 g/dL and more than 12 g/dL because baseline hemoglobin <12 g/dL was an independent risk factor of FN with CHOP or R-CHOP chemotherapy in previous studies (11, 12). Disease stage was categorized with the Ann Arbor staging system. The relative dose-intensity (RDI) for each agent was defined as the proportion of the standard dose-intensity actually delivered. The average relative dose-intensity (ARDI) was calculated by averaging the delivered RDIs of cyclophosphamide and doxorubicin. Fever was defined as a single oral temperature measurement of ≥38.3℃, or a temperature of ≥38℃ sustained over a one-hour period. FN was defined as the occurrence of fever in a state of grade 4 neutropenia (ANC<0.5×109/L) (7, 13, 14).
Statistical methods
The demographic and clinical characteristics of all patients were analyzed using descriptive statistics. A one-way ANOVA with post-hoc analysis by Tukey's honestly significant difference (HSD) was applied for comparison of mean ANC after each cycle of chemotherapy. Univariate associations between the neutropenia or FN and individual explanatory variables were analyzed with Cox regression. Stepwise logistic regression analyses were applied to determine variables significantly associated with the occurrence of neutropenia and febrile neutropenia. Variables associated with the presence of neutropenia or FN in the univariate analysis at a P value of <0.15 were tested as the independent variables in the logistic analysis. The SPSS 13.0 software program was used for statistical analysis. Two-sided P values of less than 0.05 were considered statistically significant.
RESULTS
Patient characteristics
Baseline demographics and disease characteristics are summarized in Table 1. The median age of the 181 patients (111 males and 70 females) was 57 yr (range 17-78 yr) at diagnosis, and 35.3% (64/181) of patients were over 65 yr old. In addition, 14.4% (26/181) patients had a history of diagnosis and treatment of another malignancy, and 5.5% (10/181) of patients had comorbidities (1 case of coronary artery disease with congestive heart failure, 1 case of coronary artery disease with diabetes mellitus, 5 cases of diabetes mellitus, 1 case of end stage renal disease, 1 case of dementia and 1 case of connective tissue disease). HBV markers were tested in 175 patients and 14.9% (26/175) patients were hepatitis B surface antigen (HBsAg) carriers with normal liver tests; 50.8% (92/181), 22.1% (40/181), 11.6% (21/181), and 15.5% (28/181) of patients were low, intermediate low, intermediate high, and high risk on the IPI (International Prognostic Index), respectively. In 95.6% (173/181) of cases, a bone marrow biopsy was performed at diagnosis. Of these, bone marrow involvement of DLBCL was detected in 7.5% (13/161) of cases. Baseline median serum LDH levels and ANC were 211 U/L (range 92-1,239) and 3.81×109/L (range 0.34-18.56), respectively.
Pattern of neutropenia and FN after R-CHOP chemotherapy in patients with DLBCL
Every patient received a median of 6 (range 4-8) cycles of R-CHOP chemotherapy and the median interval of each chemotherapy cycle was 28 (range 19.6-50) days. A total of 60.2% (109/181) of patients experienced at least one episode of grade 4 neutropenia (ANC<0.5×109/L) during chemotherapy and of these, 42.2% (43/109) of patients progressed to FN (Table 2). There was no statistically different incidence of FN between R-CHOP-21 (24.6% [16/65]) and R-CHOP-28 (23.3% [27/116]) chemotherapy groups. Overall, 23.8% (43/181) of patients receiving R-CHOP experienced FN at some point during this study. In all 65 events of FN, blood cultures were performed, and 6 suspicious organisms (2 Gram (-) bacilli, 4 Gram (+) bacilli) of FN were identified. As shown in Table 2, a greater amount of G-CSF was administered to FN patients. Among FN patients, 27.9% (12/43) of patients received chemotherapy with unplanned dose reductions and 79.1% (34/43) of patients experienced median 14 days of treatment delays. As a result, in 9.3% (4/43) of FN patients, treatment was terminated early. There was no early termination of treatment in non-FN patients.
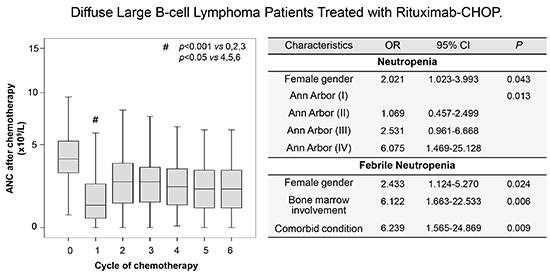
Initial ANC at the time of presentation and ANC before and 7 days after each cycle of chemotherapy was measured. When ANC after chemotherapy cycle was analyzed in 93% (161/181) of patients, ANC after the first cycle of chemotherapy was significantly lower than those after subsequent cycles (Fig. 1). Indeed, more than half of neutropenia (62.4%) occurred in the first cycle of R-CHOP. Forty-eight percent (48.8%) of patients experienced their first episode of FN in the first cycle of chemotherapy. In 34.9% of patients, more than 2 episodes of FN were occurred during whole chemotherapy cycles. However, interestingly, all patients experienced their first FN in the first cycle of chemotherapy never experienced FN again during subsequent cycles of chemotherapy. All FN patients were admitted to a hospital and empirical intravenous antibiotics including anti-pseudomonal β-lactam (cefepime) and aminoglycoside were administrated after sampling for sputum, blood and urine culture. In this study, there was no mortality related with FN.
Potential risk factors associated with neutropenia and febrile neutropenia
Univariate analysis of potential risk factors of neutropenia (ANC <0.5×109/L), and FN is shown in Table 3. Female gender (P=0.019), high Ann Arbor staging (P=0.001), IPI (P=0.003), and LDH above upper limit of normal (P=0.029) were all significantly associated with a risk of neutropenia. Among these factors, female gender (P=0.004) and higher Ann Arbor staging (P=0.015) and IPI (P=0.004) were significantly associated with episodes of FN. In addition, age ≥65 (P=0.044), patients with comorbidity (P=0.013), bone marrow involvement of lymphoma (P=0.003), and baseline serum albumin ≤3.5 mg/dL were significant risk factors of FN. However, baseline Hb <12 g/dL, ANC <1,500/µL and BSA <1.9 m2 reported risk factors of FN were not associated with episodes of FN in this study. These statistically significant variables associated with neutropenia and FN were included in the logistic regression model for multivariate analysis (Table 4). Multivariate analysis shows that only female gender (odds Ratio [OR], 2.021; 95% confidence interval [CI], 1.023-3.993, P=0.043) and high Ann Arbor staging (OR, 6.075; 95% CI, 1.469-25.128, P=0.013) were risk factors for the occurrence of neutropenia. And female gender (OR, 2.433; 95% CI, 1.124-5.270, P=0.024) was a risk factor of FN as well. However, Ann Arbor staging was not an independent risk factor of FN based on multivariate analysis. Among the variables associated with FN in univariate analysis, patients with comorbidity (RR, 6.239; 95% CI, 1.565-24.869, P=0.009) and bone marrow involvement of lymphoma (RR, 6.122; 95% CI, 1.663-22.533, P=0.006), including the female gender, were independent risk factors for FN in this study.
DISCUSSION
Myelosuppressive chemotherapy-induced neutropenia with fever often results in hospitalization with the administration of empiric broad-spectrum antibiotics and has been associated with considerable morbidity and mortality along with increasing medical costs (15). Current guidelines state that chemotherapy regimens with the occurrence rate of FN, more than 20%, between 10 to 20%, and lower than 10% are considered high, intermediate, and low risk for FN, respectively (7, 16). These classifications of chemotherapy regimens are based on several clinical trials including only eligible patients. Therefore, hematologic toxicities are often underreported in these highly selected patients. Based on early clinical trials, an R-CHOP-21 regimen is regarded as an intermediate risk for FN in NCCN and EORTC guidelines (7). However, the occurrence rate of FN in several observational studies of an R-CHOP regimen including patients who had received primary prophylaxis of G-CSF was 17%-22% (4, 12, 17). In this study, 23.8% of patients experienced at least one episode of FN without primary prophylaxis of G-CSF. All of the above studies suggest that an R-CHOP regimen itself is a high risk of FN in real clinical situations.
Since the prophylactic administration of G-CSF is not mandatory in the intermediate risk group based on NCCN and EORTC guidelines, it is important to find out which patients have high-risk features related to FN. From several clinical trials with different cancer types, a variety of patient- and disease-related risk factors have now been implicated in the risk of developing FN, including older age, poor performance status, advanced disease, comorbidities, low baseline blood cell counts, and low body surface area/body mass index (8). Being older than 60 or 65 yr was found to be a risk factor most consistently associated with the development of FN in several studies including non-Hodgkin's lymphoma (NHL) patients (11, 12, 18, 19). However, in other studies including NHL patients treated with CHOP, age was not an independent risk factor for FN (20, 21, 22). One study that classified patients older than 70 further into 70-74 yr, 75-79 yr, and >80 yr of age showed that even more advanced age did not appear to increase the risk for FN (23). Instead, some studies have suggested that physiological age, as demonstrated by performance status, may be a better predictor of risk than chronological age itself (23). Actually, studies including NHL, breast, and lung cancer have shown that not old age itself but poor performance status is a risk factor for the development of FN. However, Salar et al. reported that old age and poorer performance status were both independent risk factors for FN in NHL patients treated R-CHOP regimen (12). Therefore, old age or poorer performance status could be a potential risk factor for FN. However, they could not be an absolute risk for FN in any chemotherapy regimen. In this study, being older than 65 yr was also a risk factor for FN in univariate analysis but not in multivariate analysis. And poor performance status was only associated with occurrence of neutropenia but not with episode of FN. Although different cut points were analyzed, several studies have shown that low BMI or low BSA is a risk factor for FN (11, 21, 24). However, low BSA (<1.9 m2) was not a risk factor in this study. Since BSA of Asian population is lower than that of Western population, variable different cut point of BSA (1.4-2.0 m2) were analyzed (data not shown). Nonetheless, none of cut point of BSA were associated with neutropenia or FN in this study.
In the studies with NHL (21, 25) and small-cell lung cancer (26), female gender has been found to be a risk factor for the development of FN. In this study, female gender was an independent risk factor for the development of neutropenia and FN after R-CHOP chemotherapy. Because most studies did not explore or discuss this issue, it is not easy to determine why females experience FN more frequently after chemotherapy. Nonetheless, we can carefully assume the answer with reference to the studies showing that drugs are more slowly cleared in female body for several reasons, including their differential distribution into fat, slower metabolism, or slower excretion of drugs. For example, doxorubicin has shown significant gender- and body composition-related differences in pharmacokinetic profile (27, 28). These pharmocokinetic differences of chemotherautic agents between males and females probably explain the sensitivity of myelosuppresion in female patients treated with an R-CHOP regimen.
Many studies including NHL have found that abnormal laboratory values are important risk factors for FN. Salar et al. reported that lower baseline hemoglobin (<12 g/dL) was an independent risk factor for FN in NHL patients treated with an R-CHOP regimen (12), and Pettengell et al. reported that low baseline albumin (<3.5 g/dL) was an independent risk factor for FN in NHL treated with a CHOP regimen (18). Lyman et al. found that lower baseline ANC (<1,500/µL) was an independent risk factor for FN in NHL treated with various regimens (25). In this study, only low baseline albumin was associated with the occurrence of FN. However, none of the above potential risk factors were independent risk factors in this study.
Disease-related risk factors for FN can be categorized into tumor type, advanced disease, and genetic risk factors. Advanced disease status has been found to be a significant predictor of FN in studies with various cancers including NHL, breast, ovarian, lung, colorectal, and prostate cancer (8, 24). In this study, higher Ann Arbor staging was a risk factor for neutropenia and NF. Bone marrow involvement of DLBCL by bone marrow biopsy, which is known to be a poor prognostic factor independently of IPI (29) was reported as a risk factor for FN in NHL patients. Interestingly, in this study, an independent risk factor for FN is not advanced Ann Arbor staging, but rather bone marrow involvement of DLBCL confirmed by bone marrow biopsy.
The most serious outcome of FN is mortality. In this study, there was no mortality related with FN. Overall survival between patients never experienced FN and patients experienced at least more than one episode of FN was not different statistically. FN can lead to a delayed treatment schedule with early termination and induce a reduction of chemotherapy dose. In this study, patients with FN experienced longer treatment delays and more frequent dose reductions of chemotherapy. What is worse, almost one out of 10 FN patients experienced the early termination of treatment due to FN. Since in patients with aggressive non-Hodgkin lymphoma (NHL) reduced chemotherapy delivery has been associated with impaired outcomes (4, 30), dose reduction and early termination of treatment due to FN will lead to adverse outcomes in patients. Therefore, if FN can be prevented, medical costs will be decreased and patients' overall outcome can be improved. Many studies have already proven that primary prophylaxis with G-CSF can effectively reduce FN (17). Nevertheless, there is still controversy over the routine use of primary G-CSF prophylaxis in DLBCL patients treated with an R-CHOP regimen in terms of the cost-benefit. However, considering that most FN developed after the first chemotherapy cycle and those patients never experienced FN again in the rest of their chemotherapy cycles in this study, routine primary G-CSF prophylaxis can be cost-effective in DLBCL patients treated with R-CHOP.
In summary, 23.8% of DLBCL patients treated with R-CHOP experienced FN without primary prophylaxis of G-CSF in this study. Median 14 days of treatment delays were observed in FN patients and 27.9% (12/43) of patients with FN were received reduced dose of chemotherapy (ARDI <85%). Even in 9.3% (4/43) of patients, early termination of treatment was occurred due to FN. The presence of bone marrow involvement, comorbidities, and female gender were independent risk factors for FN. The present study showed that an R-CHOP regimen itself is associated with a high risk of FN without primary prophylaxis of G-CSF and suggested that the occurrence rate of FN will be increased in patients with the above risk factors. Therefore, routine primary prophylaxis of G-CSF is recommended to minimized treatment failure. After all, more studies to identify and validate the risk factors for FN and analyzing the cost-effectiveness of routine primary prophylaxis of G-CSF will be needed, along with considering racial and socioeconomic differences of DLBCL patients treated with R-CHOP chemotherapy.




 XML Download
XML Download