

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Knee pain is a common physical complaint in the elderly. Nguyen et al. (1) reported an increasing trend in the prevalence of knee pain in the United States after they evaluated data from the National Health and Nutrition Examination Surveys between 1971 and 2004 and from the Framingham Osteoarthritis Study between 1983 and 2005. Kim et al. (2) investigated 504 community residents of Chuncheon, Korea, aged ≥50 yr, and reported that the prevalence of knee pain was 46.2% (32.2% in men, 58.0% in women) and increased with age in women.
The prevalence of knee osteoarthritis (OA) in elderly Koreans has been reported by several researchers. Cho et al. (3) reported that the prevalence of radiographic OA was 38.1% in residents aged ≥65 yr in Seongnam, Korea. Kim et al. (4) reported that prevalences of radiographic OA and symptomatic OA were 37.3% and 24.2%, respectively, in residents aged ≥50 yr in Chuncheon. Although OA is the most common cause of knee pain in elderly people (5), disorders other than OA may also cause knee pain in this population. It has also been reported that radiographic changes correlate poorly with pain and that knee pain is a better predictor of disability than radiographic changes (6).
Previous studies that investigated the epidemiology of knee pain or OA in elderly Koreans were limited to some local areas in Korea. Thus, arguments could be raised against the representativeness of these results. Additionally, there is no reported study presenting severity profiles of knee pain in Koreans. We investigated epidemiological indices of knee pain and its severity-prevalence, risk factors, and impact on quality of life-in a representative sample of elderly Koreans.
MATERIALS AND METHODS
Subjects
The Korea Center for Disease Control and Prevention has conducted the Korea National Health and Nutrition Examination Survey (KNHANES) on a random sample of the general Korean population to assess health and nutritional status through interviews and health examinations. The fifth KNHANES was conducted from 2010 to 2012, assessing the whole nation each year without overlapping of survey areas or participants. A multistage stratified probability sampling was used according to geographical area, gender, and age groups, based on the Statistics Korea registries.
Fig. 1 is a flowchart that shows the inclusion of subjects in this study. Of the 8,958 participants in the fifth KNHANES conducted in 2010, a total of 3,273 was aged ≥50 yr. We excluded 203 persons who did not respond to the question about the presence of knee pain and 16 persons who did not report the severity of knee pain or reported a pain score of 0 even though they reported that they had knee pain. Finally, 3,054 elderly persons were included in the analysis.
Data collection
A questionnaire was distributed to the participants to evaluate demographic, socioeconomic, lifestyle, and health status information, including presence of knee pain and its severity. Subjects were divided into three age groups: 50-59, 60-69, and ≥70 yr. Educational level was categorized as college graduation or below. Occupations were categorized as a manual or non-manual occupation. An occupation demanding physical or heavy exertion was defined as a manual occupation.
For smoking status, subjects were classified into former or current smokers vs non-smokers. Alcohol consumption was classified according to frequency by modifying the definitions used by Anttila et al. (7). Those who drank alcohol at least once per month in the past year were defined as frequent drinkers. Those who drank alcohol less than once per month or who did not drink in the past year were defined as infrequent or non-drinkers. Regular exercise was defined as practicing high-intensity physical activities (strenuous or gasping activities such as running, high-speed cycling, and swimming) for at least 20 min at one session and at least 3 days per week, or practicing moderately intense physical activities (slightly strenuous or gasping activities such as slow swimming, badminton, and table tennis) for at least 30 min at one session and at least 5 days per week, or walking for at least 30 min at one session and at least 5 days per week.
The presence of hypertension was defined as a systolic blood pressure ≥140 mmHg, a diastolic pressure ≥90 mmHg, or taking anti-hypertensive medication(s). The presence of diabetes mellitus was defined as a fasting glucose level ≥126 mg/dL, a history of taking oral hypoglycemic agent(s) or insulin injection, or physician-diagnosed diabetes mellitus. The presence of obesity was defined as a body mass index (BMI) ≥25 kg/m2, calculated by dividing weight (kg) by the square of height (in meters).
Participants aged ≥50 yr underwent knee radiography; the radiographs were evaluated using the Kellgren-Lawrence grading scale: grade 1, doubtful narrowing of joint space and possible osteophytic lipping; grade 2, definite osteophytes and possible narrowing of joint space; grade 3, moderate multiple osteophytes, definite narrowing of joint space, some sclerosis, and possible deformity of bone contour; and grade 4, large osteophytes, marked narrowing of joint space, severe sclerosis, and definite deformity of bone contours (8). To maintain quality control of the radiographic examinations, the radiology technicians were taught how to use the digital x-ray machine and the standard radiography procedures before they participated in the survey. Two independent radiologists examined the radiographs; if the two reported different Kellgren-Lawrence grading scales for a radiograph and the difference was greater than 2, then the radiograph was transferred to a third radiologist for final determination of the scale value (9). Radiographic OA was defined by a Kellgren-Lawrence grade 2 or higher radiographic change.
Knee pain in the fifth KNHANES was defined as the presence of pain in the knee joint lasting 30 or more days during the most recent 3 months. Participants with knee pain were asked to rate their pain severity on a 10-point numerical rating scale (NRS), where 0 was the absence of pain and 10 was the most severe pain. Although the pain severity score was a numeric, the distribution was extremely skewed. More than half of the subjects reported a score of 0 (i.e., no knee pain). The extreme skew creates a potential problem with treating this variable as an interval level variable and modeling it with linear regression. Thus, we transformed the severity score into an ordered variable with four levels: none, mild, moderate, and severe. The cutoff points between mild, moderate, and severe pain levels were based on the study by Jones et al. (10). They assigned a NRS to a four-level metric after extensively reviewing literature, consultations with several pain experts, and consideration of pain guidelines and recommendations. The assignments were as follows: 0=no pain, 1-3=mild, 4-6=moderate, and 7-10=severe.
In the fifth KNHANES, EQ-5D was used to measure quality of life. It is a measure of health status developed by the EuroQol Group. It consists of five questions on mobility, self-care, pain, usual activities, and psychological status, with three possible answers for each item (1=no problem, 2=moderate problem, 3=severe problem) (11). A summary index with a maximum score of 1 (EQ-5D index) can be derived from these five dimensions by conversion using a table of scores. The maximum score of 1 indicates the best health state, in contrast to the scores of individual questions, where higher scores indicate more severe or frequent problems (12).
Data analysis
The prevalence of knee pain and profiles of its severity in elderly Koreans were calculated and represented diagrammatically. Logistic regression analysis was used to estimate crude and adjusted odds ratio (OR) for knee pain with regard to risk factors. The PROC LOGISTIC procedure in the SAS statistical package (ver. 9.3; SAS Institute, Inc., Cary, NC, USA) was used to conduct logistic regression analysis for knee pain.
The proportional odds model is an extension of logistic modeling and is used for assessing proportionality where the response variable takes on values in a set of ordered categories. It was used to estimate crude and adjusted proportional odds ratio (POR) for severity of knee pain with regard to risk factors. If POR for a specific risk factor is 2.0, the subjects are 2.0 times more likely to report a greater severity of knee pain. The PROC GENMOD procedure was used to calculate PORs for severity of knee pain, with a multinomial distribution and cumulative logit link function (13).
The EQ-5D index was analyzed and compared between subjects with knee pain and without knee pain, and between subjects with individual severity profiles and without knee pain using Student's t-test. Overall and gender-specific quartiles of EQ-5D indices were created. The lowest quartile represented the worst EQ-5D indices. Crude and adjusted ORs for belonging to the worst group of EQ-5D indices with regard to knee pain or severity profiles were calculated. The PROC LOGISTIC procedure was used to conduct logistic regression analysis for belonging to the worst group of EQ-5D indices.
RESULTS
The average age of the subjects was 63.6±9.1 yr. Of the subjects, 56.3% were women; 10.2% were college graduates; 34.2% had manual occupations; 15.9% were current smokers; 43.5% consumed alcohol; 50.7% performed regular exercise; 48.8% had hypertension; 16.9% had diabetes mellitus; 34.6% had obesity (BMI≥25 kg/m2); 31.1% had hyperlipidemia; 39.0% had radiographic OA, defined as the presence of Kellgren-Lawrence grade 2 or more radiographic change (Table 1).
The prevalence of knee pain in all subjects was 23.1% (11.7% in men, 31.9% in women). As age increased, the prevalence of knee pain increased. In every age group, women had a higher prevalence of knee pain than men (Fig. 2).
The prevalences of mild, moderate, and severe knee pain in all subjects were 4.3%, 9.1%, and 9.7%, respectively. Those in men were 2.8%, 5.4%, and 3.5%, respectively; those in women were 5.4%, 12.0%, and 14.4%, respectively (Fig. 3).
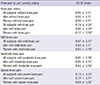
Crude ORs showed significantly higher risk of knee pain in those ≥60 yr old, women, those with a low level of education, hypertension, obesity, or radiographic OA. Current and former smokers or those who frequently consumed alcohol had significantly lower risks for knee pain. The adjusted ORs revealed that those ≥60 yr old, women, and those who had a low level of education (less than college), a manual occupation, obesity, or radiographic OA had significantly higher risks for knee pain, compared with those without (Table 2).
Based on the crude PORs, those ≥60 yr old, women, those with a low level of education, hypertension, diabetes mellitus, obesity, or radiographic OA reported greater severity of knee pain. Former and current smokers or those who frequently consumed alcohol were more likely to report lower severity of knee pain. The adjusted PORs revealed that those ≥60 yr old, women, and those who had a low level of education (less than college), a manual occupation, obesity, or radiographic OA had a risk for reporting greater severity of knee pain, compared with those without (Table 3).
All subjects, all men, or all women with knee pain had significantly lower EQ-5D index scores than all subjects, all men, or all women without knee pain. All subjects or all women with mild knee pain had significantly lower EQ-5D index scores than all subjects or all women without knee pain. Men with mild knee pain had lower EQ-5D index scores than men without knee pain, but the difference was not significant. All subjects, all men, or all women with moderate knee pain or severe knee pain had significantly lower EQ-5D index scores than all subjects, all men, or all women without knee pain (Table 4).
All subjects, all men, or all women with knee pain had significantly higher risks for belonging to the worst EQ-5D index quartile compared with all subjects, all men, or all women without knee pain, unadjusted or after adjusting for other risk factors. All subjects or all women with mild knee pain had significantly higher risks for belonging to the worst EQ-5D index quartile compared with all subjects or all women without knee pain. Men with mild knee pain had a higher risk for belonging to the worst EQ-5D index quartile than men without knee pain, but the difference was not significant. All subjects, all men, or all women with moderate or severe knee pain had significantly higher risks for belonging to the worst EQ-5D index quartile compared with all subjects, all men, or all women without knee pain (Table 5).
DISCUSSION
We analyzed data from the fifth KNHANES, conducted in 2010. The KNHANES is a nationwide survey, and data are obtained from subjects who are randomly sampled from the general Korean population. Thus, we consider that our study is representative of the prevalence of knee pain and its severity profile in the general Korean elderly population.
The prevalence of knee pain in the present study (23.1% in all subjects, 11.7% in men, and 31.9% in women) was lower than that reported by Kim et al. (2) (46.2% in all subjects, 32.2% in men, and 58.0% in women), who investigated the prevalence of knee pain in community residents of Chuncheon, aged ≥50 yr. The difference in prevalence between the two studies may be attributable to the definition of knee pain and the residence distribution (community residents vs nationwide sample). Also, age differences between the two studies should be considered. The mean age of subjects in the present study was significantly lower than that reported by Kim et al. (data not shown).
Old age, female gender, a low level of education, manual occupation, obesity, and radiographic OA were significant risk factors for knee pain. A prospective study of knee pain and its risk factors revealed that age, previous knee injuries, being overweight, and knee-straining work were risk factors for knee pain (14). No association with age, education, manual occupation, or obesity was reported by Kim et al. (2). Differences in study design, subjects, and adjustment of variables may explain the discrepancies between studies. Further studies to identify risk factors for knee pain are required.
According to the crude ORs, smoking and alcohol consumption significantly reduced the risk of knee pain. However, the adjusted ORs indicated that their influence on the study variables was insignificant. Generally, men smoke and drink alcohol more than women. The prevalence of musculoskeletal disorders is lower in men than in women (15). Thus, the apparently lower risk for knee pain associated with smoking and alcohol consumption, based on the crude ORs, probably resulted from the confounding effects of gender. The association of smoking and alcohol consumption with joint pain in previous reports is inconsistent. Felson et al. (16) found a protective association between smoking and OA when studying knee OA in the first U.S. Health and Nutrition Examination Survey and elderly members of the Framingham Heart Study cohort. They suggested that smoking, or some unidentified factor associated with smoking, modestly protects against development of knee OA. However, Amin et al. (17) reported that men with knee OA who smoke have greater cartilage loss and more severe knee pain than men who do not smoke. Maxwell et al. (18) reported that alcohol consumption is inversely associated with the risk and severity of rheumatoid arthritis. However, Adamson et al. (19) reported an inconsistent association between alcohol consumption and joint pain among men and women in the West of Scotland Twenty-07 study.
To our knowledge, this is the first reported study to present a severity profile of knee pain in elderly Koreans, risk factors that worsen the severity of knee pain, and the influence of the severity of knee pain on quality of life. This study revealed that a considerable number of elderly Koreans suffer from mild, moderate, or severe knee pain.
This study showed that the risk factors for knee pain were also risk factors for worse pain severity. Creamer et al. (20) reported that helplessness, education, and BMI were important factors in determining pain severity in knee OA. Our results are similar to theirs. People with a lower level of education generally work in manual occupations. Compared with office work, manual work usually requires high physical loads, resulting in various musculoskeletal disorders, including knee pain, and worsening severity of musculoskeletal disorders. Obesity is an emerging epidemic, and weight loss has been shown to improve pain and function in knee joints with osteoarthritis (21). Among the risk factors for knee pain and its severity, manual occupation and obesity are modifiable factors. Thus, workplace environment modifications, and weight loss programs for patients with knee pain, focusing especially on those with manual workers and those with high BMIs, may reduce the prevalence of knee pain or at least the severity of knee pain.
Excluding men with mild knee pain, participants with knee pain had significantly lower quality of life than participants without knee pain. Thus, the management of knee pain, even mild knee pain, is important for improving quality of life in the elderly population. Considering the trend toward an ageing population in Korea, early interventional approaches are needed to reduce the medical, social, and economic burdens of knee pain.







 XML Download
XML Download