

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The incidence of thyroid cancer has increased in several European countries (1-3), the United States (4), Canada (5), and Australia (6) during the past several decades. In Korea, the incidence of thyroid cancer has been increasing rapidly (7) and is now the highest in the world (8).
Radiation exposure is the only accepted risk factor for developing thyroid cancer, particularly during childhood (9, 10). Other factors that have been proposed as risk factors, such as diet (11), reproductive issues (12), genetic factors (13), smoking, alcohol intake (14), and weight gain (15), remain controversial. However, neither radiation exposure nor other factors explain the recent steep increase in the incidence rate of thyroid cancer. According to some studies, changes in diagnostic practices may be one of the major causes for this increase (2, 16). Indeed, the introduction of ultrasonography and fine-needle aspiration biopsy have improved the rate at which small nodules (17, 18) and radiographic "incidentalomas" are detected (19). However, it remains unclear whether the increased rate of thyroid cancer has resulted primarily from higher detection rates (20).
To date, few studies have examined the relationship between thyroid cancer and socioeconomic status (SES) (21-25). Some of these extant studies have suggested that higher SES is a risk factor for a diagnosis of thyroid cancer because individuals with higher SES may undergo health check-ups more frequently (26). However, most studies have been conducted with Caucasian patients; and to our knowledge, only one study has been conducted with a Korean population (27). That study used data from the Korean National Health Insurance Cancer Registration and examined the association between family income and cancer incidence. However, their data were not representative of the Korean population as a whole as the study included only self-employed individuals and medical aid beneficiaries; moreover, they focused only on family income. Thus, we used the Korean National Health and Nutrition Examination Survey (KNHANES) data collected from a representative sample of the Korean population to examine associations between the prevalence of thyroid cancer and SES, defining the latter in terms of monthly household income and educational level.
MATERIALS AND METHODS
Study subjects
The current study was based on the KNHANES data collected between 2010 and 2011, the first and second periods of KNHANES V (2010-2012). The KNHANES is a health survey conducted by the Korea Centers for Disease Control and Prevention using a nationwide, population-based, cross-sectional design (28). After the first KNHANES was conducted in 1998, the second, third, fourth, and fifth surveys were conducted in 2001, 2005, 2007, and 2010-2012, respectively. The field surveys were conducted by specially trained interviewers at mobile centers and in subjects' households. The health interviews and health examinations were performed in specially designed and equipped mobile centers that traveled to locations throughout the country.
A total of 17,476 subjects were enrolled, and the response rate was 81.2% (8,598/10,938 in 2010 and 8,878/10,589 in 2011). The current survey excluded 4,170 respondents aged 19 yr or younger and 1,030 whose data were unavailable. We therefore analyzed data from a total of 12,276 subjects (5,277 men and 6,999 women) in the current study.
Study measures
The subjects were interviewed by trained examiners using a questionnaire including items asking about monthly household income, years of education, marital status, smoking habits, alcohol intake, physical activity, and history of thyroid cancer. Body weight was measured to the nearest 0.1 kg with subjects dressed in light clothing. Height was measured to the nearest 0.1 cm with participants in their stocking feet. Place of residence was categorized into urban and rural areas. Smoking status was defined based on self-reported cigarette use; never-smokers had smoked fewer than 100 cigarettes in their lifetimes, and subjects who had smoked 100 or more cigarettes were classified as past or current smokers based on current smoking habits. Alcohol intake was assessed with questions about drinking behavior during the month prior to the interview. Answers to the question about physical activity were coded as "yes" when subjects performed moderate or strenuous exercise on a regular basis (moderate exercise: more than 30 min in one session more than five times per week; strenuous exercise: more than 20 min in one session or more than 30 min of walking in one session more than five times per week.
The prevalence of thyroid cancer was assessed with the following question: "Before study enrollment, were you ever diagnosed by a doctor with thyroid cancer?" Subjects who answered "yes" were classified as patients with thyroid cancer.
SES was assessed based on monthly household income and educational level. Monthly household income was categorized into quartiles: lowest (<USD 918.3), medium-lowest (USD 918.3-1,836.5), medium-highest (USD 1,826.6-3213.9), and highest (USD≥3,214.0). Participants were also divided into four categories according to the number of years of schooling: elementary school (<7 yr), middle school (7-9 yr), high school (10-12 yr), and university (≥13 yr).
Statistical analysis
All statistical analyses were performed using SPSS version 15.0 (SPSS, Inc., Chicago, IL, USA). All data were expressed as means±standard deviations (SDs) or as percentages (categorical variables). Differences in baseline variables according to monthly household income and educational level were compared using analyses of variance (ANOVA) for continuous variables and chi-square tests for categorical variables. Univariate and multivariate logistic regression analyses were used to calculate odds ratios (ORs) for the potential risk factors for thyroid cancer. Statistical significance was set at P<0.05.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki guidelines, and informed consent was obtained from each subject. All examination protocols were approved by the institutional review board of the Korea Centers for Disease Control and Prevention (No. 2010-02CON-21-C and No. 2011-02CON-06-C). Informed consent was waived by the board.
RESULTS
Baseline characteristics of subjects
The baseline characteristics of the 12,276 subjects (71 patients with thyroid cancer and 12,141 non-patients) are presented in Table 1. The mean (±SD) age was 50.3±16.5 yr, and the mean weight was 62.3±11.5 kg. In terms of marital status, 1,660 (13.5%) participants were single, 9,179 (74.8%) were married, 312 (2.5%) were divorced, and 1,113 (9.1%) were widowed. With respect to place of residence, 5,627 (45.8%) subjects lived in urban areas, and 6,649 (54.2%) lived in rural areas. A total of 2,603 (21.3%) participants currently smoked, and 8,778 (71.5%) consumed alcohol. Among individuals with thyroid cancer, five (7.0%) had household incomes in the lowest, 18 (25.4%) in the medium-lowest, 23 (32.4%) in the medium-highest, and 25 (35.2%) in the highest quartiles (Fig. 1). Eleven (15.7%) patients with thyroid cancer had <7 yr of education, 11 (15.7%) had 7-9 yr of education, 30 (42.9%) had 10-12 yr of education, and 18 (25.7%) had ≥13 yr of education (Fig. 2).
Characteristics of subjects according to monthly household income
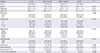
Table 2 presents the characteristics of subjects according to monthly household income. The data show that younger age and increased height and weight tended to be associated with higher monthly household income. Higher household income was also associated with more education, residence in urban areas, history of alcohol intake, and history of diagnosis with thyroid cancer.
Characteristics of subjects according to educational level
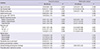
Table 3 presents the characteristics of the subjects according to educational level. The data show that younger age and increased height and weight tended to be associated with more education, which was also associated with higher monthly household income, residence in urban areas, histories of smoking and alcohol intake, and physical activity.
Univariate and multivariate logistic regression analyses of potential risk factors for thyroid cancer
Table 4 presents the ORs for thyroid cancer according to the univariate and multivariate logistic regression analyses. The multivariate logistic regression analysis revealed that older age (OR, 1.03; 95% confidence interval [CI], 1.00-1.05), being female (OR, 8.16; 95%CI, 2.99-22.24), being overweight (OR, 1.04; 95%CI, 1.01-1.06), monthly household income (OR, 3.27; 95%CI, 1.16-9.20 for medium-highest household income vs lowest household income; O,R 3.30; 95%CI, 1.16-9.34 for highest household income vs lowest household income), educational level (OR, 2.74; 95%CI, 1.16-6.46 for 10-12 yr vs <7 yr), and alcohol consumption (OR, 1.89; 95%CI, 1.08-3.32) were significant risk factors for thyroid cancer.
DISCUSSION
The current study examined whether the prevalence of thyroid cancer was correlated with SES using data from the 2010-2011 KNHANES. The data suggested that monthly household income and educational level were significant risk factors for thyroid cancer after adjustment for other covariates.
To date, few studies have examined the association of thyroid cancer with SES. Sprague et al. (25) conducted an ecological study using thyroid cancer registry data from Wisconsin for 1980-2004. These authors reported that the incidence of thyroid cancer was higher in counties with higher household incomes and higher education levels. According to a cohort study of residents of the San Francisco Bay area, higher educational level was an independent risk factor for developing thyroid cancer (24). Additionally, research examining data on thyroid cancer in Caucasian people living in Los Angeles County from 1972 to 1995 found that higher levels of monthly household income and education were significant risk factors for thyroid cancer (23). A study examining the association between cancer incidence and family income in a Korean sample (27) reported that higher income was associated with a higher risk of thyroid and prostate cancers in men and of thyroid cancer in women compared with other cancers, such as stomach, liver, and lung cancer. However, according to a case-control study conducted in Canada, SES and occupational prestige were not significant risk factors for developing thyroid cancer (21), which is not consistent with our results. Although we do not know the reason for this inconsistency, that study differed from the present research in several ways. First, subjects in the Canadian study completed mail-in questionnaires and were not interviewed by trained examiners. Second, the correlation between the incidence of thyroid cancer and monthly household income was analyzed in men only because no data were available for women.
During the past several decades, the incidence of thyroid cancer has increased in most industrialized countries (1-6). According to one study examining the incidence of cancer in countries in North and South America, Asia, Europe, and Oceania from 1973 to 2002, the incidence of thyroid cancer has increased five folds in men and nearly 10 folds in women (29). In Korea, the incidence of thyroid cancer has also markedly increased. Within the past 10 yr alone, it increased from 10.4 per 100,000 in 1999 to 87.4 per 100,000 in 2010 in women and from 2.1 per 100,000 in 1999 to 18.3 per 100,000 in 2010 in men (7).
Many studies have been conducted to explain the recent increase in the incidence of thyroid cancer. However, radiation exposure is the only accepted risk factor for developing thyroid cancer in consensus (9, 10), and it has been difficult to explain the dramatic increase in the incidence of this disease in terms of other factors that have been proposed as risk factors, such as diet (11), reproductive issues (12), genetic factors (13), smoking, alcohol intake (14), and weight gain (15). For this reason, some researchers have hypothesized that increased detection has led to the increased reported incidence of thyroid cancer (25). That is, it has been suggested that the recent increase in thyroid cancer actually reflects an increase in the detection rate that is attributable to improvements in such diagnostic modalities as ultrasonography and fine-needle aspiration biopsy (24, 25, 30).
According to our results, higher levels of monthly household income and education are significant risk factors for thyroid cancer. It is plausible that the correlation between higher SES and thyroid cancer can be explained by the fact that individuals with higher SES access health care services more easily than do those with lower SES (31). Additionally, it is also highly probable that this higher rate of healthcare service utilization may lead to diagnostic work-ups of the thyroid to further evaluate symptoms of thyroid disorders, such as menstrual irregularities, fatigue, and nervousness, which, although vague, are common (32). It can be inferred that the thyroid cancer of those in higher SES groups would be more likely to be detected than would that of those in lower SES groups. Thus, higher rates of detection may have led to the higher reported prevalence of thyroid cancer in higher SES groups (25).
However, it would be premature to conclude that the recent increase in thyroid cancer is attributable only to differences in detection according to SES. Indeed, the incidence of thyroid cancer may have actually increased due to as-yet-unknown risk factors (33). The Surveillance, Epidemiology and End Results (SEER) program conducted between 1980 and 2005 in the US raised doubts about the detection hypothesis because it found an increase in the incidence of the largest (>5 cm) as well as the smallest (≤1 cm) tumors (20). However, it is highly probable that the recent increase in thyroid cancer in the Korean population is attributable to increased detectability. First, the increase in thyroid cancer in Korea primarily involves papillary thyroid carcinoma and thyroid cancer <1 cm, and this increase occurred from 1995 to 2006 (34). Second, the 5-yr survival of patients with thyroid cancer increased from 94.2% to 99.8% from 1993 to 2010 (7).
This study has several limitations. First, its cross-sectional design precludes drawing conclusions about the direction of the observed association between the prevalence of thyroid cancer and SES. Second, data about thyroid cancer were obtained via a questionnaire study rather than a retrospective analysis of medical records. Third, we failed to obtain data about experiences with thyroid ultrasonography. Despite the above limitations, the current study provides valuable information in that it is the first to evaluate the correlation between the prevalence of thyroid cancer and SES using a representative sample of the Korean population.
In conclusion, our results, based on the 2010-2011 KNHANES data, show that higher levels of household income and education are significant risk factors for thyroid cancer. Our results indicate that the recent increase in the prevalence of thyroid cancer in Korea is attributable more to higher detection rates than to any increase in actual prevalence due to as-yet-unknown risk factors. Further prospective studies are needed to examine the correlation between the prevalence of thyroid cancer and histopathological data, including tumor size.




 XML Download
XML Download