

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
During recent several decades, Koreans have experienced a lot of disasters such as Seongsu Bridge collapse, Sampoong Department Store collapse, Daegu Metro fire, and several natural disasters. Following these traumatic events, some people suffer from psychiatric disoders such as acute stress disorder (ASD) and posttraumatic stress disorder (PTSD).
ASD develops as a response to the experience(s) of a terrifying or traumatic life stressor within 2 days of the incidence (1). It is characterized by an array of symptoms that are also observed in PTSD: avoidance, re-experiencing, and hyper-arousal. Although PTSD and ASD appear to be somewhat identical in terms of symptomatology, the main difference between the two diagnoses is the time elapsed since the traumatic incidence: a diagnosis of ASD can only be given within a month posttrauma whereas PTSD is diagnosed from the first month after the events (2). In addition to the time contingencies regarding two diagnostic criteria, ASD diagnosis requires at least three kinds of dissociation to be experienced, while in PTSD the dissociative symptoms are counted as a part of avoidance symptoms (2). That is, criteria concerning dissociations are more strictly mandated in ASD diagnosis than in PTSD. The rationale underneath such requirement is that dissociative symptoms appearing immediately after a trauma represent pathological responses, which in turn keeps the victim from processing information about the incident properly, hence probably increasing the chance of developing PTSD later (3). Thus, not only the shared diagnostic criteria among ASD and PTSD but also the diagnostic criteria of dissociation in ASD should be assessed thoroughly if one aims to identify among the victims of trauma who would likely to go on suffering PTSD.
Up to date, there are several Korean translated assessment tools to evaluate PTSD symptoms such as The Korean version of the Impact of Event Scale-Revised (IES-R) (4), the Korean version of the Davidson Trauma Scale (5), the Korean version of the Startle, Physiological arousal, Anger, and Numbness (6). However, no assessment tool is available for ASD in Korea.
Reviewed several instruments of assessing acute stress disorder in the literature, Cardeña and his colleagues (7) noticed that there are no inclusive measure of ASD that takes both peritraumatic dissociation and overlapping symptoms into account for expanding diagnostic significance of ASD. Thus, from previous versions of 98-item Acute Stress Reaction Questionnaire (SASRQ), Cardeña et al. (7) modified it into the current 30-item version for the sake of accurate diagnosis of ASD, better predictability of PTSD diagnosis, and easier, more efficient administration of the test.
Relatively recent inclusion of ASD diagnosis in Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) (2), along with the culturally pervasive self-help tendency of Korean population with regard to psychiatric/psychological problems, diagnosis of ASD as well as PTSD is currently new and scarce at best. Although the diagnostic criteria for ASD and PTSD have just been revised in the Diagnostic Statistical Manual Version 5 (DSM-5) that has very recently released (8), in the meanwhile, it is helpful to have a measure that can move forward research of ASD in Korea and among other Korean speaking populations.
Thus, the present study aimed to produce Korean version of SASRQ that was based on the DSM-IV diagnostic criteria and to evaluate its psychometric properties.
MATERIALS AND METHODS
Study population
Our sample consisted of 2 groups: graduate students of counseling psychology at Ewha Woman's University (Group 1) and employees at Cheorwon Fire Station, Province of Gangwon (Group 2). Prior to the main study, every participant candidate was asked to complete a set of questionnaires for screening. Questionnaires used for screening are Beck Depression Inventory (BDI) (9), and Spielberger's State Trait Anxiety Inventory (STAI) (10). Only Group 1 was included in the assessment and analysis of test-retest reliability. Screening data from mental health of employees working at the fire station were used in this analysis. Those subjects who scored over 24 on BDI and over 61 on STAI were withdrawn from the study (9, 11). Also, subjects who have any past or current psychiatric illness were excluded; out of 113 participant candidates recruited, total 13 were excluded. All subjects were interviewed by trained psychiatrists and were ascertained to be free of major psychiatric problems.
Procedures and assessment instruments
The 30-item SASRQ with 10 items on dissociation; 6 each on re-experience, avoidance, and hyperarousal; and 2 items on impairment in functioning was produced by Cardeña et al. (7). The scale can be scored either on 5-point likert scale or on a dichotomous format. As a result of reviewing six studies calculated Cronbach's alpha for current version of SASRQ, the internal consistency was found to be generally good to excellent, with alpha ranged between 0.64 and 0.95. Test-retest reliability for 3-4 week was r=0.69 in a study of non-traumatized undergraduate students (7).
The comparability of Korean version of Stanford Acute Stress Reaction Questionnaire (SASRQ-K) and the original SASRQ has been validated by stringent translation and back-translation procedures. First, the SASRQ was translated into Korean language by two psychiatrists. It was then back-translated by a bilingual person to validate the translation. Lastly, the back-translated version was reviewed by the original author. The content of the final SASRQ-K was further verified by back and forward-translations until the meaning of each item matched the originals. Finally, SASRQ-K was established after the confirmation was made by the original author. The scale was scored on 5-point likert scale format.
A 21-item BDI (12) was used to assess depressive symptoms and to screen participants out. The Korean version of BDI was demonstrated to have generally good psychometric properties, with its internal consistency being 0.85 (9).
The STAI (13), a self-report scale consists of 20 items each for measuring state and trait anxiety, was also used for screening the participant candidates. The Korean version of the STAI was shown to exhibit excellent psychometric properties, and its internal consistency was at α=0.91 (10).
The IES-R (14) is a revised version of IES with an inclusion of additional 7 items to the original. It is a self-rating scale that measures the frequency of posttraumatic stress disorder symptoms experienced within the previous week. IES-R was used in this study to evaluate convergent validity of SASRQ-K. According to Lim et al. (4), the Korean version of the IES-R reported to show good psychometric properties, with internal consistency and test-retest reliability being α=0.93 and r=0.91, respectively.
A Global Measure of Perceived Stress Scale (PSS) (15) is a 14-items self-rating scale that assesses individual's perceived level of stress following a stressful life event(s). PSS is among the last instruments adopted for demonstration of convergent validity of SASRQ by measuring its relevance to it. Coefficient alpha reliability of PSS ranged 0.84-0.86 in three different groups and the test-retest correlation was 0.85 within 2-day interval (15).
Statistical analysis
Internal consistency was estimated using Cronbach's alpha. Test-retest reliability was assessed by calculating the intra-class correlation coefficient. The concurrent and divergent validity between SASRQ-K and other measures was evaluated using Pearson correlation coefficients. All statistical analyses were performed using SAS/PC version 9.2 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Description of the sample
The socio-demographic characteristics of participants are presented in Table 1. Majority of the participants were male (70%), working class (73%), with college education (57%).
Internal consistency
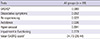
Internal consistency of full-scale and subscales of SASRQ-K were evaluated with Cronbach's coefficient α. As shown in the Table 2, α yielded high estimates of reliability in Group 1 and 2 (α=0.98). In addition, subscales of SASRQ-K resulted in moderate to high levels of α, which fell within a range of 0.78 and 0.95.
Test-retest reliability
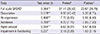
SASRQ-K was administered to participant Group 1 twice with an interval of 2 weeks. Test-retest reliability of full-scale and subscales of SASRQ-K were estimated, and the results are as follows: total and subscale SASRQ-K scores demonstrated moderate to good level of test-retest reliability, with the coefficient r fall in a range of 0.466-0.709; however, the last subscale (impairment in functioning) of SASRQ-K failed to show reliability (r=0.237) (Table 3).
Convergent validity
Convergent validity of SASRQ-K was demonstrated by evaluating correlations among the total score of SASRQ-K and those of two other questionnaires assessing PTSD symptoms: IES-R and PSS. Total score of SASRQ-K found to be positively correlated with PSS (r=0.811, P<0.001) and IES-R (r=0.520 P<0.001).
DISCUSSION
Recently, as media increasingly draw attention to various issues regarding mental health problems and their contributions to social issues such as suicide, domestic abuse, and violent crime (18), the public perceptions of psychological/psychiatric disorders and their treatments are now changing. While depression and schizophrenia are amongst the most publicly well-known psychiatric disorders, it was not until recently that PTSD has been subjected to any kind of public discussion in Korea.
Regarding its relatively new inclusion in DSM-IV in 1994 and lack of public knowledge and misbeliefs about mental disorders, ASD, let alone PTSD, is still barely known in Korea. Without awaring that ASD actually is a diagnosable disorder, it is presumable that considerable proportion of people who are going through difficult times following traumatic events might as well assume their acute stress symptoms as part of the 'normal' process which does not necessarily require medical attention or help. In order to prevent people from developing PTSD, identifying those who are at high risk of subsequent PTSD immediately after the trauma will be necessary. For decades, whether or not ASD precedes PTSD has been controversial, and there are mixed evidences regarding the issue (19-27). Because the diagnostic value of ASD is in prediction of PTSD, the clinical utility of this scale is at the stake of further research on this area. However, ASD may be important in itself as a form of suffering even for individuals who develop it in response to trauma do not later meet criteria for PTSD. With regard to this matter, development of SASRQ-K, which assesses ASD symptoms of peritraumatized people, has clinical significance.
Thus, a Korean version of SASRQ was developed to assess symptoms of acute stress disorder, hence to help identify people who suffer psychiatric symptoms following traumatic events and would subsequently develop posttraumatic stress disorder. Two groups recruited for the study showed some differences in demographical characteristics, but they are combined for statistical analysis since none of the factors found to be affecting the total scores of the scales used. To investigate psychometric properties of SASRQ-K, first we examined internal consistency. Both the full scale and subscales of SASRQ-K showed good to excellent internal consistency, with Cronbach alpha coefficient ranging between 0.78 to 0.98. Next, the test-retest scores at a 2-week interval were evaluated. In contrast to the full scale and 4 subscales, last subscale (i.e., impairment in functioning) of SASRQ-K failed to show significant correlation bewteen the pre- and post-test scores. Small sample size (n=27) used in the test-retest analysis, as well as the higher variability of the individuals in their functioning level in time may have affected the result. Unlike other symptoms measured by SASRQ, function is a construct that could be readily and widely affected by extraneous, environmental, situational factors and will likely wax and wane in severity with time; thus, we speculated the level of functions could vary in 2-week period with or without the experience of traumatic events.
Furthermore, convergent validity of SASRQ-K was demonstrated by examining its correlation with other scales. Total mean score of SASRQ-K were positively correlated with scales assessing posttraumatic stress disorder symptoms experienced within the previous week (IES-R, r=0.811). Correlation between SASRQ-K and PSS also showed significant correlations (r=0.520), thus the convergent validity was demonstrated. Finally, divergent validity was demonstrated by insignificant correlation with a scale measures social desirability (SDS, r=0.07).
However, results of this study are not without limitations. Firstly, because both groups of participants have distinctive backgrounds (i.e., graduate students and employees at firestation), and are mostly male and single, the findings should be interpreted cautiously. However, the fact that two very different groups of participants did not show significant differences in their total scores of SASRQ-K should be noted. Secondly, current study did not include clinical populations for comparison. Inclusion of patients with acute stress disorder in future study would enhance its value as a diagnostic tool.
In conclusion, SASRQ-K has reasonable internal consistency, test-retest reliability, convergent validity, and divergent validity. The development of assessment tool for ASD may help facilitate research regarding prevalence, etiology, diagnosis, and prediction of development of PTSD.

 XML Download
XML Download