

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Streptococcus pneumoniae (pneumococcus) is an important pathogen with high associated morbidity and mortality worldwide. It causes otitis media, sinusitis, pneumonia, and invasive pneumococcal diseases (IPD). Diagnosis of IPD requires pneumococcus isolation from a normally sterile site, such as blood, cerebrospinal fluid (CSF), and pleural or ascitic fluid. The incidence of IPD in developed countries is estimated to be 8-34 cases per 100,000 inhabitants with geographical variance (1), and the mortality rate ranged from 10% to 30% (2-4). Despite the availability of vaccines and antibiotics, a 2008 report from the World Health Organization (WHO) indicated that S. pneumoniae is responsible for approximately 1.6 million deaths annually, particularly among young children and the elderly (5).
Pneumococci are spherical, Gram-positive bacteria, which have many virulence factors, including capsular polysaccharides, pneumolysin, pneumococcal surface protein A (PspA), pneumococcal surface protein C (PspC), and pneumococcal surface adhesin A (PsaA). Among these, capsular polysaccharides are considered to be the most important virulence factor as they surround pneumococci and shield them from phagocytes. Currently, 94 capsular serotypes, including the recently reported serotypes 6C, 6D, 11E, and 20A/20B, have been identified (6-9). Each serotype is distinguished by serological response (the ability to react with specific antibodies against the capsular antigen), the chemical structure of capsular polysaccharides, and other related genetic mutations. Based on these pathogenic mechanisms, a serotype-specific pneumococcal polysaccharide vaccine (PPV) was developed, which contained pooled capsular polysaccharides of various serotypes. In 1983, a 23-valent PPV (PPV23) was approved, expanding serotype coverage to more than 85% of the organisms causing IPD at the time (10). However, the poor immunogenicity of T-cell-independent PPV23 in infants led to development of the pneumococcal conjugate vaccine (PCV). Covalent coupling of the polysaccharide to a protein carrier effectively converts the T-cell-independent Type 2 polysaccharide into a T-cell-dependent antigen; carrier proteins include a non-toxic mutant of diphtheria toxin (CRM197), as well as other proteins such as protein D of non-typeable Haemophilus influenzae (11). The first 7-valent PCV (PCV7) was licensed in the United States (US) in 2000 and introduced to Korea in 2003. This PCV included capsular polysaccharides of serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F, representing approximately 80%-90% of IPD in children (12). With serotype shifts resulting from vaccine pressure, however, the protective coverage of PCV7 was reduced, and PCV7 did not include serotypes 1, 3, and 5, which are common in Europe, Asia, and Africa (13, 14). Therefore, a 13-valent PCV (PCV13), which included serotypes 1, 3, 5, 6A, 7F, and 19A, was introduced for children in 2010 and later licensed for adults in 2012.
Thus, pneumococcal capsules play the most important role in pathogenesis, and they have a great implication in vaccine development. Of note, serotype distributions of pneumococcal capsules vary geographically and temporally in terms of nasopharyngeal carriage, pathogenicity and clinical presentation (13, 15). This article will review the serotype-specific characteristics of pneumococcus with regard to the epidemiological and clinical aspects, including carriage rate, invasive disease potential, clinical presentation, and antibiotic resistance.
PNEUMOCOCCAL CARRIAGE RATE
Pneumococcus exists only in the nasopharynx of humans, and it has no natural reservoir in animals. Humans are the exclusive targets of pneumococcal diseases, with transmission only coming from other human carriers. Thus, carriage is essential for the propagation of pneumococcal diseases, and its epidemiology is important. Pneumococcal colonization may be influenced by multiple factors. Although these factors are not entirely clear, there is no doubt that the local host immune response plays an important regulatory role in the trafficking of pathogens in the nasopharynx. Poorly immunogenic serotypes tend to colonize for longer periods, and the low carriage rates in adults suggest the existence of immunological protection after previous exposure (16).
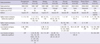
Pneumococcal carriage occurs early in life, usually with a prevalence of about 30%-60% in infants and 1%-10% in adults (17, 18). In some cases, more than 95% of children can be colonized with up to six different serotypes by the age of two (19). The prevalence of co-colonization by multiple serotypes was estimated to range from 1.3% to 48.8% (20, 21). Geographical factors, study population, and different detection techniques may be responsible for this variation (21). The epidemiology and clinical significance of co-colonization needs better clarification. As children grow older, the prevalence of pneumococcal carriage decreases, and the distribution of colonizing serotypes changes to those found in adults. Before the age of nine, the carriage rate is maintained above 30%-40%, but it declines progressively afterward (Table 1) (22-24). However, the carriage rate is quite variable according to the local epidemiology, trending toward higher carriage rates in impoverished communities with low vaccination rates. Studies by Mackenzie et al. and Hill et al. showed remarkably high carriage rates (≥ 30%), even in young adults (Table 1) (25, 26). In Korea, the pneumococcal carriage rate was estimated to be 34.3% among children aged 5 yr or younger before the introduction of PCV7 (27), and it was 16.5% among those aged 18 yr or less in the era of PCV7 (28). Considering the difference in study populations, there is a limitation to comparing the results of these two studies (Table 1), and data on Korean adults is not available.
Common colonizing serotypes differ between young children (< 5 yr) and adolescents/adults. Before the introduction of PCV7, serotypes 19F, 6A, 6B, and 23F were prevalent in young children aged less than 5 yr, while serotypes 3 and 23F were relatively common in adolescents and adults (22, 23, 29). After the introduction of PCV7, these were replaced by non-vaccine serotypes, including 19A, 6C, 11A, 15A, and 15B/C (28, 30).
The duration of colonization can range from days to months and depends on the serotype (31). Serotype 1 is rarely found to colonize the nasopharynx, and serotypes 4, 5, and 7F also colonize to lesser degrees (32, 33). These serotypes are able to initiate colonization of the nasopharynx, but colonization may be much shorter in duration compared to other serotypes. Sleeman et al. (33) estimated the duration of pneumococcal carriage among common colonizing serotypes. The duration ranged from 5.9 weeks for serotype 15C to 19.9 weeks for serotype 6B.
Causative mechanisms of carriage rate remain unclear. Several mechanisms have been postulated, most of which hinge on interactions between the bacteria and host immune defenses. Serotype-specific polysaccharide capsules protect against immune-mediated clearance in several ways, including blocking the deposition and function of opsonins (34), trapping by neutrophil extracellular traps (NETs), and clearance by mucus (35, 36). Both the prevalence of carriage and virulence appear to be directly related to the degree of encapsulation. In a murine study, Weinberger et al. (37) demonstrated higher carriage rates among serotypes with larger capsules. Furthermore, those serotype capsules containing more carbon molecules per polysaccharide repeat unit tend to be smaller and more prone to nonopsonic killing. Authors from this study suggest that low-carbon polysaccharide repeats would require less energy to manufacture and afford a lower "metabolic cost," allowing a larger polysaccharide bulk and therefore improved fitness for carriage.
INVASIVE DISEASE POTENTIAL
Pneumococcal capsule types are known to be associated with many important pathogenic processes, including complement deposition, inflammation, and binding to the C-type lectin of host phagocytes (38, 39). In an animal study by Briles et al. (40), a very strong association was demonstrated between capsular serotype and virulence (the ability of an isolate to kill mice and the length of time between inoculation and death). In mice, serotypes 3, 4, 6A, and 6B were virulent; serotype 1 isolates were marginally virulent; and serotypes 14, 19, and 23 were avirulent. Clinically, global surveillance demonstrates that a limited number of capsular serotypes cause more than 70%-80% of IPD (41), and the invasive property of pneumococci seems to be determined by capsular serotype rather than genotype, as determined by multilocus sequence typing (MLST) (42). Genetic elements may contribute to the heterogeneity of invasive disease potential among the same serotype (43).
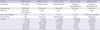
Some serotypes commonly colonize the nasopharynx, thereby having a greater temporal opportunity for invasion. In comparison, some serotypes are more likely to cause invasive disease with each episode of colonization. Several parameters have been used to estimate the serotype-specific invasive disease potential: invasive odds ratio (OR), invasive capacity (IC), and attack rate. Among them, invasive OR has been used most frequently in the literature (29, 42-46). Invasive OR is calculated by reference to all the other serotypes as follows: OR = (ad)/(bc), where a is the number of invasive A serotypes, b is the number of carriage A serotypes, c is the number of invasive non-A serotypes, and d is the number of carriage non-A serotypes. IC is calculated as the ratio of IPD incidence to carriage prevalence, while the attack rate is defined as the ratio of IPD incidence to the incidence of acquisition for each serotype (33, 47). Both are expressed as the number of IPD cases per 100,000 carriages or acquisitions. Sleeman et al. (33) classified a high attack rate as 20 or more IPD cases per 100,000 acquisitions, and a low attack rate as less than 10 IPD cases per 100,000 acquisitions. Table 2 summarizes studies about the relationship between pneumococcal serotype and invasive disease potential. Some serotypes (1, 4, 5, 7F, 8, 12F, 14, 18C, and 19A) were considered highly invasive, while others (6A, 6B, 11A, 15B/C, and 23F) were generally less invasive in most studies (29, 33, 42, 43, 45-47). Serotype prevalence was variable between studies, which may be due to geographic and epidemiologic differences. Serotype 6B was highly invasive according to the report by Hanage et al. (44), but was not as invasive in other studies (29, 33, 42, 43, 45, 46). Also, reports of the invasive disease potential of serogroup 9 (9A, 9V, 9N, and 9L) showed some variation (29, 33, 42-46). Except for the study by Yildirim et al. (47), all the studies of Table 2 were conducted before the widespread use of PCV7. Recently, Scott et al. (24) assessed changes in the serotype-specific invasive disease potential during the PCV7 era and found no remarkable change in the invasive potential among serotypes. Although the serotype-specific IPD incidence might be proportional to the carriage prevalence, it is important to continue monitoring the change in the serotype-specific invasive disease potential.
CLINICAL PRESENTATIONS
Different pneumococcal serotypes are known to cause different clinical presentations of pneumococcal diseases. Globally, serotypes 3, 6A, 6B, 9V, 14, 19A, 19F, and 23F were reported to cause acute otitis media (AOM) in young children, according to a recent review (48). Particularly, serotype 19A pneumococcal AOM increased predominantly after the introduction of PCV7 (49, 50). Serotypes 3, 11A, and non-typeable (NT) pneumococci are associated with acute conjunctivitis (46). Regarding IPD, serotypes 1, 5, and 7F usually affect healthy young adults with a low mortality rate, while serotypes with low or intermediate invasive potential are more likely to affect the elderly with underlying comorbidities (32, 51, 52). Yildirim et al. (53) compared the incidence and serotype distribution of IPD among children less than 18 yr of age between the early (2001-2006) and late (2007-2010) periods of the PCV7 era in the US. The overall IPD incidence rate was 7.5 cases per 100,000 inhabitants, without a statistical difference between these two periods, although the proportion of bacteremic pneumonia among all IPD cases was almost three-fold greater in 2009-2010 compared to the early period. IPD due to serotypes 19A and 7F increased during the late period of the PCV7 era, representing 41% and 20% of all IPD cases in the same period, respectively. Changes in the distribution of serotypes may affect the clinical presentation of IPD.
A recent meta-analysis evaluated serotype-specific case fatality rates (CFRs). This study revealed that serotypes 1, 7F, and 8 were associated with lower mortality, whereas serotypes 3, 6A, 6B, 9N, and 19F were associated with increased mortality (54). In a nationwide, population-based cohort study of IPD in Denmark over the period of 1977-2007, serotypes 3, 10A, 11A, 15B, 16F, 17F, 19F, 31, and 35F were associated with highly increased mortality as compared with serotype 1 (adjusted odds ratio ≥ 3, P < 0.001) (55). Van Hoek et al. (56) estimated the CFRs of IPD by serotype and age group (< 5, 5-64, and ≥ 65 yr) in England from April 2002 to March 2011. Among patients younger than 5 yr, CFR was low (overall 3%), with the highest rate occurring with serotype 6A (7%), followed by 19F (5%), 9V (5%), and 3 (5%). In the age group of 5-64 yr, the overall CFR was 10%; serotypes 31 (33%), 11A (30%), and 19F (21%) had the highest CFRs, while serotypes 1 (3%), 7F (4%), and 8 (6%) had the lowest rates. Patients aged 65 yr and older had the highest CFR (overall 30%); serotypes 19F (41%), 31 (40%), and 3 (39%) were associated with the highest CFRs, whereas serotypes 1 (17%), 7F (20%), and 12F (21%) were associated with lower CFRs.
Pneumonia
S. pneumoniae is the most common cause of community-acquired pneumonia (CAP) in children and adults (57). While the majority of pneumococcal pneumonia cases are non-bacteremic (60%-80%), bacteremic pneumonia is more severe (58-60). Bacteremic and non-bacteremic pneumonia are considered to be different clinical entities. In mice, several thousand colony-forming units (CFUs) of S. pneumoniae of serotypes 2 or 3 in the lungs result in bacteremia and death, whereas S. pneumoniae of serogroup 19 is unable to induce bacteremia after lung infection and results in a nonprogressive course unless tens of millions of CFUs are inoculated (61).
According to a recent meta-analysis, pneumococcal serotype 14 was the most prevalent etiologic agent of pneumococcal CAP, followed by serotypes 1 and 5, in Latin America and the Caribbean (Table 3) (62). Since PCV7 was not adopted into the national immunization program in the Latin America and Caribbean regions during the study periods, it was not possible to determine the serotype shift between the pre- and post-vaccination eras. In the studies which included the post-PCV7 periods, serotype 1 was predominant, followed by serotypes 19A and 3. The prevalence of serotype 14 was decreased to around 5% (60, 63, 64).
Among adults, Burgos et al. (65) reported that serotype 14 was still one of the most common causes of pneumococcal pneumonia in Spain, even after PCV7 introduction. Likewise, in a UK study, Bewick et al. (66) also reported that the most common serotypes were 14, 1, 8, 3, and 19A in adult pneumococcal CAP, while serotypes 19A, 3, and 6A/C were the most prevalent in IPD. They emphasized that cohort studies of IPD alone may underestimate the true prevalence of serotype 14. In comparison, Cilloniz et al. (60) reported serotypes 1 and 19A as the predominant agents of invasive pneumococcal pneumonia in Spanish adults. Although the vaccination rate and secular trend affect the outcomes, there may be some differences in the serotype distributions between invasive and non-invasive pneumococcal pneumonia, particularly among adults. As for the serotype distribution in pneumonia, no data was available from Asian countries.
Necrotizing pneumonia is a complicated pneumococcal infection, which is associated with a significant increase in morbidity and mortality. In the pre-antibiotic era, studies of autopsy cases described a necrotizing change in about 5% (0.7%-27%) of cases, and a recent large-series study (using computed tomography) reported its occurrence in 6.6% of adult pneumococcal pneumonia cases (67). Serotype 3 strains have been recognized as the most common etiologic agents (63, 67, 68).
Empyema
Serotypes 1, 3, 7F, 14, and 19A are known to be associated with empyema complications after pneumococcal infection (69-72). Empyema was considered rare in children, but it has been increasing worldwide over the last decade (69, 73-75). Lee et al. (76) evaluated 62 Korean children with empyema, where serotype 19A was most frequently identified (46.2% of pneumococcal empyema). In a recent US study of 49 cases of pediatric empyema, serotypes 3 (26.5%) and 19A (22.4%) were the most common etiologies, followed by serotypes 7F (14.3%) and 1 (12.2%) (77). However, many studies showed that most pediatric empyema cases were more directly linked to non-PCV7 serotype 1, due to selective PCV7 pressure (64, 78, 79). According to the MLST of serotype 1 isolates, sequence types (ST) 227, ST228, and ST304 were genotypes that previously existed, while ST306 was newly detected after PCV7 introduction (78, 80). Serotype 1 pneumococcal empyema was also common in adults aged between 18 and 50 yr; according to the report by Burgos et al. (81), more than 40% of pneumococcal empyema were caused by serotype 1. It is also possible that serotype 1 is associated with empyema due to the zwitterionic polysaccharides found in its capsule, which have been related to abscess formation in animal models (32).
Meningitis
S. pneumoniae is estimated to cause more than 60,000 meningitis-associated deaths and long-term disabilities in children five years of age or younger worldwide annually (82). The incidence of pneumococcal meningitis is highest in children under one year of age, but data on the serotype distribution remain insufficient in Asian countries. According to surveillance in Ugandan children aged less than five years, the most common serotype was 6A/6B (40%), followed by 22A, 23F, 14, and 19A (83). Previously, serotypes 1, 3, and 5 were rarely reported in cases of meningitis (52). However, recent studies in the African meningitis belt revealed that 60%-80% of pneumococcal meningitis was caused by serotype 1, with higher incidence and case fatality ratios compared to meningococcal meningitis (84). Compared to the US and Europe, where a bimodal age distribution is observed, the pneumococcal meningitis epidemiology of the African meningitis belt is quite different. Serotype 1 is predominant, and older children and working-age adults are more likely to be infected, with a high case fatality rate. Such differences might be due to the properties of the African lineage of serotype 1, rather than the general characteristics of serotype 1 (85). MLST has identified three clonal lineages of serotype 1, and these were geographically segregated. As for travelers to African meningitis belt areas, PCV13 vaccination is recommended in addition to the meningococcal vaccination.
Serotype prevalence in the US has undergone a significant shift since routine immunization with PCV7 commenced. Comparing data from 1998-1999 to 2004-2005, there has been a significant reduction in pneumococcal meningitis among the PCV7 serotypes, from 59 to 23 percent of cases (P < 0.001) (86). Non-PCV7 serotype disease has expectantly increased, from 28 to 65 percent (P < 0.001), with a preponderance of the increase being attributed to serotypes 19A and 22F (86). Despite the observed serotype shift, the overall incidence of pneumococcal meningitis in the US has decreased by 30 percent to 0.79 cases/100,000 (86).
Peritonitis
Primary pneumococcal peritonitis in children has been recognized for more than a century (87, 88). Its peak incidence occurs in children between the ages of 5 and 7 yr, and it is more common in girls than in boys (89). Pneumococcal peritonitis is usually associated with nephrotic syndrome in children, while it is related to cirrhosis in adults (90-92). In healthy adults, pneumococcal peritonitis is unusual, but it typically occurs in young women as a result of serotype 1 pneumococci (93, 94), causing pelvic abscesses or other reproductive tract infections. Pneumococci are still common etiologic agents of spontaneous bacterial peritonitis in cirrhotic patients; however, there is no published data on the serotype distribution.
Hemolytic uremic syndrome
Hemolytic uremic syndrome (HUS) is characterized by the triad of microangiopathic hemolytic anemia, thrombocytopenia, and acute renal failure. Typical HUS usually follows an episode of gastroenteritis with enterotoxigenic Escherichia coli. Although S. pneumoniae-associated HUS (SP-HUS) occurs after bacterial infection, similar to typical HUS, the clinical outcomes are worse than typical HUS, with a higher dialysis requirement (82% vs 42%) and mortality rate (< 11% vs < 5%) (95). SP-HUS is known to occur exclusively in children after IPD, with a low incidence rate (0.4%-0.6%) (96, 97). However, SP-HUS is often mistaken for disseminated intravascular coagulation (DIC), and, as result, not all SP-HUS cases may have been reported. Nevertheless, case reports are increasing after the introduction of PCV7 (98-100).
The hypothesized pathogenic mechanism of SP-HUS suggests that neuraminidase-producing pneumococcus exposes the normally hidden Thomsen-Freidenreich antigens (T-Ag) of erythrocytes, platelets, and renal endothelial cells. Free T-Ag reacts with anti-T immunoglobulin, resulting in hemolysis, polyagglutination, endothelial damage, and thrombotic microangiopathy (101, 102). Positive T-Ag activation and a direct Coombs' test are predictive of SP-HUS after IPD, and these aid in differentiating typical and atypical HUS (95, 99).
Considering the pathogenic mechanism, SP-HUS development may not be dependent on the capsule serotype. Limited data suggest a weak association of SP-HUS with specific serotypes (1, 3, 6A, 7F, 12F, 14, 19A, 22F, and 23F), as well as a high concurrence with empyema (103, 104). In mouse models, pneumococcal neuraminidase expression was higher in the lungs than in blood and was greater in bacteria growing in biofilms than in planktonic forms, potentially explaining the strong association between SP-HUS and empyema (105). Pneumococcal serotypes with a high predilection to cause complicated pneumonia accompanying empyema may be major etiologies of SP-HUS. Before the introduction of PCV7, serotype 14 was the most common, but a serotype shift was observed, with increasing cases of serotypes 1, 3, 7F, and 19A, with serotype 3 being predominant (100, 106-108).
ANTIBIOTIC RESISTANCE
The ability of S. pneumoniae to undergo horizontal gene transfer leads to its genetic diversity and helps the organism adapt to environmental changes, including antibiotic pressure. Theoretically, the genotype should primarily correlate with antibiotic resistance. However, strategies for pneumococcal vaccines are actually based on serotype distribution, and therefore serotype-related antibiotic resistance has also been studied with interest. Herein, the relations between the pneumococcal serotype and genotype were addressed with regard to antibiotic resistance. Hsieh et al. (109) showed that different serotypes of S. pneumoniae possess different levels of genetic competence, which is the ability of a cell to take up extracellular DNA from its environment. Isolates belonging to serotypes 3 and 18C that were 100% sensitive to penicillin were significantly less competent than isolates belonging to serotypes 6B, 14, 19F, 9V, and 23F, which were frequently resistant to penicillin. Intriguingly, the capsule (cps) locus of S. pneumoniae is flanked by the pbp2x and pbp1a genes, which code for penicillin-binding proteins (PBPs) (110). PBPs are enzymes involved in cell wall synthesis and are targets for β-lactam antibiotics. Under the natural selection imposed by host immunity and antibiotics, the recombination events would involve PBP genes, as well as the cps operon, and would change both the serotype and the resistance profile of the strain.
The prevalence of antibiotic-resistant S. pneumoniae has increased worldwide and might be related to the spread of pediatric pneumococcal serotypes (6A, 6B, 9V, 14, 15A, 19F, 19A, and 23F). After the introduction of PCV7, the prevalence of PCV7 serotypes and serotype 6A were reduced and subsequently replaced by non-PCV7 serotypes, including serotype 19A. Although Spain23F-ST81 and Spain6B-ST90 were well-established multidrug-resistant clones in the 1980s and 1990s, their prevalence decreased after the introduction of PCV7 (111).
Serotype 19A is the most prominent serotype worldwide, both clinically important and multidrug-resistant (non-susceptible to ≥ 3 antibiotic classes) in the era of PCV7. More than 30% of serotype 19A isolates were multidrug resistant (112, 113). With dual macrolide resistance mechanisms (ermB and mefA), they showed resistance to erythromycin (high level, MIC ≥ 32 µg/mL), tetracycline, clindamycin, cefuroxime, and trimethoprim/sulfamethoxazole (114, 115). Erythromycin resistance was highly correlated with azithromycin and clarithromycin resistance (113). Although the resistance rate for penicillin is quite low (minimum inhibitory concentration [MIC] ≥ 8 µg/mL, < 5%) based on the revised 2008 Clinical and Laboratory Standards Institute (CLSI) breakpoint, multidrug-resistant serotype 19A isolates showed relatively high penicillin MICs (MIC50, 1.5 µg/mL) (116).
In addition, some strains of recently identified serotypes 6C and 6D S. pneumoniae showed multidrug resistance (117-119). While serotype 6C was first described in 2006, it has been identified from isolates dating back to 1962 (117). Serotype 6D S. pneumoniae isolates were reported in several regions, including Korea, Japan, China, Hong Kong, Fiji, Australia, Finland, Poland, Peru, and Canada (7, 120-128).
Serotype 19A S. pneumoniae
Of note, serotype 19A pneumococci with multidrug resistance had already been reported in some regions before the introduction or widespread use of PCV7. According to a surveillance study in Korea, serotype 19A had already increased among children aged less than 5 yr before the introduction of PCV7 (8% increase between 1991 and 1997 and an 18% increase between 1997 and 2003) (116). The pre-existing ST320 genotype was responsible for the expansion of multidrug-resistant serotype 19A, which belonged to the clonal complex (CC) 320/271. ST320 serotype 19A isolates showed a higher rate of antibiotic resistance compared to non-ST320 isolates: penicillin (MIC ≥ 2 µg/mL, 47.8% vs 34.1%), cefuroxime (82.6% vs 63.7%), erythromycin (71.7% vs 65.9%), clindamycin (73.9% vs 59.3%), and trimethoprim/sulfamethoxazole (82.6% vs 64.8%) (113). Antibiotic abuse/overuse might facilitate the spread of multidrug-resistant serotype 19A strains. CC320/271 serotype 19A strains were not limited just to Korea, having become prevalent in several Asian countries. The Asian Network for Surveillance of Resistant Pathogens (ANSORP) study surveyed ten Asian countries (Korea, Japan, Hong Kong, Taiwan, Malaysia, Philippines, Thailand, Saudi Arabia, India, and Vietnam) during the period of 2008-2009 and found that 5.6% of clinical pneumonia isolates were serotype 19A pneumococci, and 51.6% of them were ST320 strains (129).
In the US and Canada, CC320/271-expressing serotype 19A emerged and expanded after PCV7 introduction, which may have arisen from a capsular switch with Taiwan19F-ST236 (130). The Active Bacterial Core Surveillance system of the US Centers for Disease Control and Prevention (CDC) reported that the proportion of IPD by penicillin non-susceptible S. pneumoniae (PNSP) expressing serotype 19A increased significantly during 2004-2008, reaching 43.7% (MIC ≥ 2 µg/mL) by 2008 (131). The proportion of CC320/271 serotype 19A isolates increased in parallel, from 20.9% to 32.9% of IPD isolates during 2005-2007. In 2007, 82.1% (202 among 246) of serotype 19A isolates belonged to CC320/271.
In Europe, ST230 and ST276, the members of CC230, have been identified as a major serotype 19A lineage responsible for causing IPD (111, 132). Compared to Korea and North America, the STs were diverse, and ST320 was infrequent. In a Portuguese surveillance study from 2001 to 2006, ST320 was absent, and ST230 was the most common genotype (133). A French study characterizing invasive isolates also identified ST276 as a representative clone (132). In Italy, the increased prevalence of serotype 19A was due to expansion of CC199 (ST416 and ST199) after PCV7 introduction (134). According to the Spanish Pneumococcal Reference Laboratory (SPRL) study, however, the prevalences of ST81 and ST202 were decreasing, while those of ST878 and ST320 showed increasing trends (135). During the study period, serotype 19A increased from 5.7% in 2000 to 16.8% in 2008 (135). Therefore, continuous monitoring is required to detect the spread of multidrug-resistant clones, and strict control of antibiotic use might be an important strategy to minimize further spread.
Serotype 6C/6D S. pneumoniae
In the late PCV7 period, the prevalence of serotype 6C pneumococci increased in the US, Spain, and Portugal (117, 119, 136). The rate of multidrug resistance increased, and the strains were genetically diverse. In the US, the two main clonal clusters were ST473 and ST1292 (117). Both STs were non-susceptible to erythromycin and trimethoprim/sulfamethoxazole, and ST1292 showed decreased susceptibility to penicillin and ceftriaxone. In Spain, the increase of serotype 6C prevalence was associated with the emergence of ST386/ST4310/ST4825, which were non-susceptible to penicillin, erythromycin, tetracycline and clindamycin (119). Considering that serotype 6C was more common in older children and adults, fluoroquinolone resistance should be monitored, although its frequency has remained low (119, 137).
While serotype 6D S. pneumoniae has been isolated in several regions, it is characteristically prevalent in Korea, comprising more than 10% of serogroup 6 isolates (138, 139). Among the three clones of serotype 6D S. pneumoniae found in Korea (ST189, ST282, and ST3171), ST189 and ST282 strains are related to CC81 (138). Ko et al. (118) reported that all ST282 isolates were non-susceptible to penicillin and cefuroxime, and more than 50% of them were resistant to trimethoprim/sulfamethoxazole. In comparison, ST3171 isolates showed resistance to only macrolides and clindamycin. Fortunately, ST282 strains have only been reported in Korea, and STs of serotype 6D pneumococci were very diverse worldwide: Japan (ST2924), China (ST982 and ST4190), Hong Kong (ST5085 and ST5086), Fiji (ST639, ST473, and ST4240), Australia (ST4241), Finland (ST5163), Poland (ST948, ST2181, ST1612, and ST4734), and Peru (ST6148) (118). While currently insignificant, the trend of antibiotic resistance in serotype 6D S. pneumoniae should be monitored with vigilance.
CONCLUSION
Pneumococcal serotype appears to be much more important in determining colonization, disease development, and clinical phenotype compared to the genetic background. Among the current 94 serotypes, a limited number of serotypes cause more than 70%-80% of IPD (41). Serotypes 1, 4, 5, 7F, 8, 12F, 14, 18C, and 19A are more likely to cause IPD (29, 33, 42, 43, 45-47). Though serotypes 1 and 19A are predominantly responsible for invasive pneumococcal pneumonia, serotype 14 is still one of the most common etiologic agents of non-bacteremic pneumococcal pneumonia among adults in the era of PCV7 (65, 66). Serotype 1 pneumococcal meningitis is prevalent in the African meningitis belt, with a high case fatality rate (84), while meningitis by non-PCV7 serotypes has increased, with a preponderance for serotypes 19A and 22F in the US since routine PCV7 immunization (86). New manifestations of IPD, such as pediatric empyema and HUS, became more common in the era of PCV7 (69, 74, 98-100). Serotypes 1, 3, and 19A pneumococci are likely to cause empyema and HUS (76, 81, 100, 106, 107).
In contrast to the capsular serotype, the genotype is more closely associated with antibiotic resistance. CC320/271 strains with serotype 19A are multidrug-resistant and prevalent worldwide, particularly in North America and many Asian countries (129, 131). Several clones of multidrug-resistant serotype 6C pneumococci emerged in the US and Europe, and a multidrug-resistant 6D clone (ST282) has been identified in Korea (117-119, 138, 139).
After the introduction of PCV7 for pediatric patients, pre-existing nonvaccine serotypes expanded (serotype 19A), and new serotypes were identified (serotypes 6C, 6D, and 11E). Interestingly, serotype 6D comprises more than 10% of serogroup 6 in Korea, although it remains relatively uncommon in other areas (138, 139). Meanwhile, PCV13 was introduced for children in 2010. In turn, it was additionally licensed for adults in 2012 as the first conjugate vaccine for adults. In addition to the economic aspects (vaccination rates and cost-effectiveness), serotype distribution should be monitored to detect the emergence and expansion of undiscovered serotypes and recombinant capsular clones.
The pneumococcal epidemiology of capsule types varies geographically and temporally (13, 15). Knowledge of the serotype distribution is necessary for conjugate vaccine usage, but the seroepidemiological data is inadequate in many countries including Korea. A nationwide serosurveillance system is vital to establishing appropriate vaccination strategies for each country.

 XML Download
XML Download