

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bisphenol A (BPA) is a synthetic chemical resin used worldwide for producing plastic products, notably polycarbonate plastic food-storage containers, some water bottles, bottle tops, and epoxy resin lacquer linings of metal food cans (1). BPA leaches from polycarbonate bottles and food containers, including canned foods, and thus becomes integrated into the food chain (2-4). Adult animals tolerate acute and high doses of bisphenol (e.g., multiple doses at > 2-50 mg/kg body weight [bw]/day) without noticeable phenotypic changes (5). Recent studies have shown that in utero, perinatal, or neonatal exposure of laboratory animals (rats and mice) to bisphenol is harmful, even at physiologically relevant doses. Such "low-dose" concentrations are below the current lowest observed effect level (LOAEL, 50 µg/kg/day) for in vivo studies. The harmful effects of BPA include disruptions of 1) central nervous system development, differentiation and function, 2) reproductive function (such as, follicle development), 3) thyroid hormone function, 4) prostate and mammary gland morphology, 5) fetal oocyte meiosis and 6) immune system function (4, 6-8). Early prepubertal exposure to BPA accelerated the onset of puberty but decreased reproductive parameters in female mice (4). Biologically active, orally administered, BPA in neonatal mice results in concentrations that are 10-fold higher than adults (9). Thus, BPA may be harmful to human children (7).
BPA derivatives are present in resin-based dental sealants and composites that are increasingly used in both preventive and restorative oral health care. Mass spectrometric analysis confirmed the presence of BPA, bisphenol-A diglycidyl methacrylate (bis-GMA), bisphenol-A diglycidylether (BADGE), and bisphenol-A dimethacrylate (bis-DMA) in the composites and sealants (10). After hydrolysis of composites and sealants in alkaline (pH = 13) and acidic media (pH = 1) after heating (100℃ for 30 min), extensive breakdown of the oligomers such as bis-GMA, BADGE, and bis-DMA into BPA was observed. BPA level was increased to 3-12 times higher than before hydrolysis (10). Composite resin dental materials are used for fillings due to demand for aesthetic restorations, and concern about the potential neurotoxic and nephrotoxic effects of mercury present in amalgam fillings. Although elemental mercury from amalgams results in some exposure, the exposure is low. Several careful, prospective, epidemiologic studies using resin-based dental materials as a control group have found no adverse effects on neurodevelopment or kidney function (11-13).
Resin-based dental sealants are the most common protective coating for permanent molars and have demonstrated effectiveness in preventing (evidentiary level 1a) (14, 15) and arresting the progression of dental caries (16, 17). The number of children receiving sealants during routine pediatric dental care is increasing steadily, stimulated by federal programs at the Centers for Disease Control and Prevention and the Maternal and Child Health Bureau in the USA and school-based dental programs (18). In the United States from 1999-2004, the percentage children with sealants ranged from 20.3% to 41.0%, depending on age. On average, 11-yr-olds had 3 for 6 sealed permanent teeth and 19-yr-olds had 5 for 12 (18). In Korea, the Oral Health Act, administrative organization, and public oral health programs provided the budget to establish public programs in urban and rural areas to seal fissures. Since 2002, 210,000 children in rural and underprivileged urban areas have had fissures sealed every year. In 2000, the prevalence of 9 to 11-yr-olds with pit and fissure sealant did not exceed 20%, however, it rose to more than 40% by 2006 (19).
In clinical fillings with sealants and composite resins, the compounds are solidified by polymerization before use. However, unpolymerized monomers may be dissolved in saliva, resulting in patient exposure (10, 20, 21). Research shows that BPA leaches from dental sealant into the saliva. Bis-GMA was suggested to be the source of BPA release. The possibility of BPA being absorbed systemically through the blood should be a concern to all oral health care professionals because of its known xenoestrogenic effects.
Dental professionals and the public must know whether dental sealants and resins that contain BPA pose a hidden risk of BPA exposure. Well designed studies are needed to clarify the relationships between dental sealant/resin and salivary BPA level. However, previous studies have either been in vitro, in vivo, or in smaller-scale clinical studies. Large-scale population based study is needed and the role of potential confounders (such as demographic factors and behavioral factors) should be investigated. Therefore, we designed an age and gender matched case-control study to test the hypothesis that dental sealant/resin is associated with salivary BPA level. This study aimed to elucidate whether BPA in saliva of Korean children depends on the number of surfaces filled with dental sealants and/or resin, and to determine the cut-off level at which BPA in saliva poses higher exposure risk.
MATERIALS AND METHODS
Study design, ethical considerations and subjects
A case-control (1:1) study was used to test the hypothesis. The Community Child Centers (CCC) in Korea have provided comprehensive childcare including group meal service and various afterschool educational program to children in poverty since 2006, according to the Child Welfare Act. The CCCs council in Busan composed of 8 branches. Two or three CCCs from each branch were selected to ask to join this study. The selection criteria of CCC were following; 1) the number of children engaged in the program of each CCC is over 10 and 2) the expected compliance of CCC is high. Eighteen CCCs were asked to join this study and 13 CCCs were accepted for the survey. A total of 302 children were collected from the 13 CCCs (sampling 13 to 44 children per each CCC). Exclusion criteria were three-fold: subjects 1) having no salivary flow, 2) no response or missing data, and 3) refusal for participation by children and/or caregivers.
Selection criteria for case was determined at the number of tooth surfaces filled with sealant/resin over 4 because 4 first molars were usually sealed with dental sealants for prevention of dental caries. Among the total 302 participants, those who had 4 or more tooth surfaces filled with dental sealant/resin were 62. We selected 62 cases (subjects with more than 4 tooth surfaces filled with dental sealant/resin) and 62 controls (subjects with no teeth filled dental sealant/resin) by matching on age ± 1 yr and gender.
Oral examination
Following WHO criteria, the state of dentition and the number of tooth surfaces filled with dental sealant/resin were determined by the same clinician. Tooth surfaces filled with dental sealant/resin were examined using disposable instruments: plane mirrors and CPITN probes. No radiographs were taken. The one-week interval test-retest intra-examiner reliability had a κ-index of 0.958 for 42 subjects.
Saliva collection and preparation
All subjects were instructed to refrain from eating or drinking for a minimum of two hours before the saliva samples were collected (i.e., between 15:00 and 17:00). Individuals rinsed their mouths with water and stimulated whole saliva samples were collected using 50 mL ice-chilled Falcon screw cap tubes. Stimulated whole saliva samples were obtained after subjects had chewed for 5 min on wax blocks provided in the commercial kits. To evaluate the amount of BPA in saliva, collected stimulated whole saliva was centrifuged at 13,000 rpm at 4℃ for 10 min. The supernatant was aliquoted into 1.5 mL Eppendorf tubes and frozen at -80℃ until use.
BPA measurement
Salivary BPA level was measured using the Ecologiena® supersensitive BPA ELISA Kit (Tokiwa Chemical Industries Co. Ltd., Tokyo, Japan). To the antibody-coated microplates, 100 µL of standard BPA or sample with conjugate solution was added at room temperature for one hour. The reaction solution was removed and plates were washed three times with 300 µL of washing solution. One hundred microliters of color solution was added to each well for 30 min. The reaction was stopped by adding 100 µL of stop solution. The optical density (OD) was measured using an ELISA plate reader (Sunrise™, Männedorf, Switzerland) with a 450-nm filter.
Assessment of confounders
Age, gender, salivary flow rate, salivary buffer capacity, frequency of snacking, and frequency of tooth brushing were selected as confounders. In order to obtain information regarding age, gender, frequency of snacking, and frequency of tooth brushing, the participants were interviewed face-to-face by a trained interviewer: How old are you? (continuous variable); What is your gender? (male/female); How frequently did you eat snack last one week? (no/once in a week/twice in a week/three times in a week/once in everyday/twice in everyday/more than three times in everyday); When did you brush your teeth yesterday? (before breakfast/after breakfast/before lunch/after lunch/before dinner/after dinner/after snack/before bedtime). Salivary flow rate was measured as volume per min. Salivary buffering capacity was evaluated using Dentobuff strips (Orion Diagnostica Co. Ltd, Epsom, Finland).
Statistical analysis
The dependent variable was the number of tooth surfaces filled with dental sealant/resin (0 vs > 4). The independent variable was salivary BPA level. Scores for salivary buffering capacity were evaluated using the Dentobuff chart. The scores were categorized into three groups: 0 = low, 1 = medium, and 2-3 = high. Frequency of snacking was categorized into four groups: no = 0, once in a week = 1, twice in a week = 2, three times in a week = 3, more than once in everyday = 4. Frequency of toothbrushing was calculated by the sum of multiple answers (continuous variable). Subjects were described using frequency distributions for categorical variables and mean with standard deviation (SD) for continuous variables. A chi-square test was used to assess differences in categorical variables, and t-test was used for continuous variables, depending on the presence of dental sealant/resin (0 vs > 4 surfaces). Analysis of covariance (ANCOVA) was used to evaluate the association between salivary BPA level and dental sealant/resin filled tooth surfaces, adjusting for confounders (age, salivary flow rate, salivary buffering capacity, frequency of snacking, and frequency of tooth brushing). BPA level was divided into nine groups based on salivary BPA level at the 10th, 20th, 30th, 40th, 50th, 60th, 70th, 80th, and 90th percentiles. Logistic regression models of each BPA group were applied to evaluate the relationships between salivary BPA level and dental sealant/resin. Logistic regression models conditional for age ± 1 yr and gender were performed. In case-control studies, selection bias introduced by the matching process can occur whether or not there is confounding by the matched factors (age and gender in this study) in the source population. Therefore, odds ratios (OR) and 95% confidence intervals (95% CI) were used to evaluate the conditional logistic regression (22). We made Pair-ID variable after matching by using age and gender. The Pair-ID variable was used as group or strata to perform conditional logistic analysis.
RESULTS
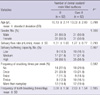
There were no differences in age and frequency of tooth brushing in subjects with or without dental sealant/resin. There were significant differences in salivary buffering capacity and frequency of snacking among subjects with and without dental sealant/resin (Table 1).
Although the salivary BPA level did not differ among subjects without dental sealant/resin and those with dental sealant/resin (0.42 µg/L and 0.90 µg/L, respectively, P = 0.293), the adjusted BPA level was significantly different (0.40 µg/L and 0.92 µg/L, respectively, P = 0.026) (Table 2).
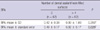
In the logistic regression model, subjects with a BPA level below 70th percentile had an OR less than 1; subjects with a BPA level between the 70th and 80th percentiles had an OR similar to 1, which is not significant. Subjects with a BPA level in the 90th percentile (over 0.952 µg/L) had a crude OR of 3.34 (95% CI 0.86-12.99, P = 0.082). After adjusting for age, gender, salivary flow rate, salivary buffering capacity, frequency of snacking, and frequency of tooth brushing, the adjusted OR increased to 4.58 and became significant (95% CI 1.04-20.26, P = 0.045) (Table 3). However, in the conditional logistic model, the significance disappeared (Table 4).
DISCUSSION
We addressed that there was a difference between sealant/resin group and no selant/resin group. There might be a possibility that dental sealant/resin is a source of BPA by evaluating the relationship between salivary BPA level and the presence of tooth surfaces filled with dental sealant/resin. Moreover, the 90th percentile BPA group had a strong association with sealant/resin group. This suggested that the cutoff BPA level might be almost 1.00 µg/L. To the best of our knowledge, this is the first study to assess salivary BPA levels due to dental sealant/resin in Korean children. Moreover, this study provides the first reference range of BPA exposure in Korean children. The major strengths of this study are 1) oral and other salivary examinations were performed clinically by a dentist and a trained dental hygienist, 2) the association was controlled for various potential confounders, including demographic features, salivary factors, and important behavioral factors, 3) relative large number of children (n = 302) were surveyed, and 4) a conditional logistic regression model was applied to avoid selection bias. Although there was no association in our age and gender matched study, salivary BPA was detected in all samples (0.002 to 8.305 µg/L).
Several animal studies have revealed effects directly related to hormonal disruption, including decreased number of off-spring and decreased birth weight after high concentration prenatal exposure (23), delayed onset of puberty (24), and increased aggression (25). Although the estrogenicity of BPA has been demonstrated in vitro and in vivo, only a few studies have examined the estrogenicity of BPA derivatives. These studies have primarily been performed in vitro and have found bis-DMA but not bis-GMA (the more common ingredient of most dental resins) to be estrogenic (26, 27).
Dental resins are composed primarily of BPA derivatives, rather than pure BPA. These derivatives are liquid monomers that polymerize into solids after either chemical or light curing. BPA is not used in dental resins because moisture from saliva inhibits polymerization hydrolyzing the 2 end hydroxyl groups, although BPA may be present as an impurity. Thus, bis-GMA, a BPA derivative, is the most common base for dental resin. Bis-GMA has methyl methacrylate groups added to the hydroxyl groups of BPA via a glycidyl spacer. Other BPA derivatives traditionally used in dental resins include bis-DMA and BADGE as well as bisphenol-A ethoxylate dimethacrylate (bis-EMA) and urethane-modified bis-GMA. Other monomers such as triethylene glycol dimethacrylate (TEGDMA) and urethane dimethacrylate (UDMA) are frequently added to the resin to maximize viscosity (28).
Although pure BPA is not a component of dental resin, it has been detected in saliva after resin placement as a result of bis-DMA hydrolysis by salivary esterases (29). Although bis-DMA hydrolysis leaves BPA, bis-GMA does not undergo this reaction, presumably because the chemical structure prevents hydrolysis at the ester linkage (28, 29). BADGE forms BADGE-diol by hydrolytic ring-opening of the two epoxide rings and is excreted in both free and conjugated forms and is further metabolized to various carboxylic acids, including two containing a methylsulphonyl moiety (30). However, other study reported breakdown of bis-GMA, BADGE, and bis-DMA into BPA (10). Further study is needed to determine whether hydrolysis of other BPA derivatives used in dental sealant/resin yields BPA.
Over the past decade, studies have evaluated the levels of BPA, bis-GMA, and bis-DMA in saliva after applying dental sealants and composites with mixed results. In some studies, both in vitro (29, 31) and in vivo (10, 20, 21), BPA or BPA derivatives were detected, whereas in other in vitro study there was no detection over periods as long as 10 days after placing sealant (32).
Salivary BPA levels decreased over time across all 3 studies; with the highest exposures (range: 0.3-2.8 ppm) immediately after placing the sealant (33) and lower exposures (range: 5.8-105.6 ppb) with 1 hr (31). The longest duration of salivary detection in any of the studies was 3 hours after placing the sealant (21). Thus, BPA exposure after placing sealant is most likely an acute event. Presumably, within a short time after application, the unpolymerized monomer is completely absorbed into saliva, posing little risk of chronic low-dose BPA exposure. These studies, however, might not have been sensitive enough to detect extremely low doses of BPA that could leach from the resin over longer periods of time.
Calafat et al. (34) suggested that BPA exposure is widespread in the United States. BPA was present at 0.1 µg/L or higher in 95% of samples, and the 95th percentile concentration was 5.18 µg/L. In our study, the highest salivary BPA concentration was 8.305 µg/L, and the 95th percentile concentration was 3.867 µg/L. Our results were similar to or slightly lower than previous studies. The human exposure limit in the United States and the European Food Safety Authority's tolerable daily intake level of BPA is 50 µg per kilogram per day (35, 36). Our results were far below these doses. The salivary BPA level detected in this study could be negligible. However, there is some controversy regarding the safe level of BPA exposure. Vom Saal and Hughes (37) proposed the need for a new risk assessment for BPA based on more than 100 in vivo and in vitro study results indicating that a BPA level far below 50 µg can cause changes in the biologic functions of cultured cells and even in a living body. They insisted that there is a "low-dose effect" for BPA, and part-per-trillion doses of BPA can alter cell functions. Wozniak et al. (38) reported that BPA levels even as low as 1 pM or 0.23 part per trillion might elicit changes in cellular level signaling. This dose is below the detection limit of this study. Therefore, all BPA levels detected (even in the undetected samples) were in the range of doses that can cause cellular changes according to their reports. Through these debates, it appears best not to expose patients to BPA or, at least, to reduce it. Salivary BPA level was in the range of doses that can elicit the "low-dose effect." Accordingly, protocols to reduce this immediate release of BPA under the "low-dose effective level" will be needed to fully confirm the safety of composite resin and sealant treatment.
Our study had some limitations: 1) The subjects in our study were from a convenience sample of volunteers, thus they might be subject to selection bias and not representative of the general population of Korean children. 2) BPA exposure is repeated and frequent due to sources other dental fillers or sealants; contaminated food, drinking water from polyvinyl chloride pipes, copy paper, and dental materials, may account for more exposure than previously realized (34). Further study is necessary to quantify how dental sealants and resin-based composites contribute to the total BPA exposure. 3) Timing of the placement of sealant/resin is an important issue in measuring BPA in saliva. Also, different commercial sealant/resin has different BPA level in saliva. However, we did not obtain the information of the timing of the placement of sealant/resin and the manufacturer of the dental sealant/resin used in the study sample. 4) High performance liquid chromatography (HPLC) and gas chromatography/mass spectrometry (GC/MS) allowed precise analytical results (39). Because these methods required complex pretreatments and heavy equipments, it is undeniable that separation analysis by HPLC and GC/MS is too complex for frequent analysis near clinical practice. Two previous studies measured salivary BPA level using ELISA (20, 21). Although there were some weaknesses in ELISA system for the measurement of salivary BPA level, using an ELISA system allowed us feasibility such as measurement without pretreatment. However, validation test between HPLC or GC/MS and ELISA should have been performed. 5) The cross-sectional design prohibited us from inferring causal relationships. Additional studies are also needed to further assess whether BPA and its derivatives in saliva at concentrations released by dental materials are absorbed systemically and whether clinical techniques can be used to control these exposures. Large-scale studies could also determine if there is chronic, low-level leaching of BPA from dental materials as they wear over time. Additional epidemiologic studies may also determine if there is a correlation between sealant exposure and clinical and subclinical end points associated with BPA exposure.
In conclusion, salivary BPA level was in the range of doses detectable and there may be a relationship between salivary BPA level and dental sealant/resin in Korean children. These findings provide an incentive to minimize human exposure to BPA in dental materials.


 XML Download
XML Download