

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The use of intravitreal injection of anti-vascular endothelial growth factor (anti-VEGF) agents has increased dramatically over the course of 5 yr and has become part of everyday praxis. Many anti-VEGF agents that suppress the activity of VEGF have been used for retinal diseases, especially for age-related macular degeneration (AMD).
Ranibizumab (Lucentis, Genentech, Inc., South San Francisco, CA, USA) is a fully humanized anti-VEGF antibody fragment that binds to all VEGF isoforms. It has been approved for the treatment of all angiographic subtypes of subfoveal neovascular AMD by the United States Food and Drug Administration (FDA) and the European Medicines Agency since 2006 and 2007, respectively (1, 2). However, the cost of ranibizumab is immense: monthly injections with a dose of 0.5 mg result in an annual cost greater than US $23,000 per patient (3).
In contrast to ranibizumab, bevacizumab was not developed for the treatment of AMD and consequently was not approved for this purpose. Similar to ranibizumab, bevacizumab (Avastin, Genentech, Inc.) is a recombinant humanized full-length antibody that binds to all isoforms of VEGF. It was approved by the FDA for intravenous injection to treat specific cancers such as metastatic colon and rectal cancer (4). For the past several years, it has been used off-label to treat VEGF-mediated retinal diseases such as neovascular age-related macular degeneration, diabetic retinopathy, and retinal vein occlusions with very encouraging preliminary results (5, 6). Bevacizumab has attracted more interest than have other anti-VEGF agents because of its low cost, considering the number of injections that are necessary at 4- to 6-week intervals (3, 7).
Systemic adverse effects have been an area of debate for intravitreal anti-VEGF medications, especially for the off-label use of bevacizumab. Ranibizumab was evaluated rigorously for safety during the FDA approval process, which ensures comparison with control groups. However, the safety of bevacizumab has not been evaluated as adequately as the safety of ranibizumab; therefore, the important question of whether the existing safety data justify the widespread intravitreal off-label use of bevacizumab has not yet been answered. Furthermore, few reports have compared the occurrence of systemic adverse events in patients treated with bevacizumab or ranibizumab in the same department (8-12).
The aims of this study were 1) to compare the incidence of systemic adverse events of intravitreal injections of bevacizumab versus ranibizumab performed by 1 referral hospital in a large series of patients during a 1-yr interval and 2) to evaluate whether intravitreal injection of bevacizumab constitutes a higher risk for systemic adverse events than does ranibizumab injection.
MATERIALS AND METHODS
We retrospectively reviewed the charts of 916 consecutive patients who received intravitreal bevacizumab or ranibizumab injections at the Seoul National University Bundang Hospital. The review period included all patients treated between April 2010 and June 2011. Although patients with a history of myocardial infarction or stroke during the 6 months prior to the study period were usually not treated, a final decision was made on the basis of a clinical risk/benefit evaluation for each case. The inclusion and exclusion criteria for treatment, retreatment criteria, and treatment strategy were maintained unchanged during the entire study period. The study was carried out in accordance with the tenets of the Declaration of Helsinki.
Baseline demographics and medical histories (including concomitant diseases) were reviewed, and changes in health status were recorded. All adverse events were confirmed by medical records or by direct information from the attending physicians. The variable "diabetes mellitus" included any type of diabetes mellitus, and the variable "hypertension" included any type of hypertension. Furthermore, any type of dyslipidemia was recorded and classified as "dyslipidemia," and any type of pulmonary disease (asthma, chronic obstructive pulmonary disease, or pulmonary fibrosis) was classified as "lung disease." Systemic adverse events were reviewed for at least 6 months after the injection.
Intravitreal injection methods
All injections were performed under standard sterile conditions. Under topical anesthesia with proparacaine (0.5%) eye drops, the bulbar conjunctiva and fornices were rinsed with 5% povidone-iodine, followed by application of a sterile drape and lid speculum. After application of a drop of 10% povidone-iodine, 0.05 mg (0.05 mL) ranibizumab or 1.25 mg (0.05 mL) bevacizumab was injected via the pars plana. The needle was removed carefully, and the injection site was compressed with a sterile cotton applicator to prevent reflux. Antibiotic eye drops were applied 4 times per day for 6 days after the injection.
Statistical analysis
Statistical analyses were performed using a commercially available software package (IBM SPSS Statistics 18; SPSS Inc., Chicago, IL, USA). Significant differences between the 2 groups were evaluated using the unpaired t test and Mann-Whitney test for normally distributed data and data that were not normally distributed, respectively. Differences in proportions were assessed using Pearson's chi-square test or Fisher's exact test, and the results are presented as the odds ratio (OR) and the 95% confidence interval (95% CI). To assess whether a variable had predictive value for the occurrence of a new systemic adverse event and to account for different follow-up times, Cox regression was performed with the outcome variable "new systemic adverse events" as the status variable and "time-to-event" as the time variable. Potential predictors (covariates) were diabetes mellitus, hypertension, dyslipidemia, angina, myocardial infarction, congestive heart failure, arrhythmia, cerebrovascular accident, dementia, cancer, lung disease, peripheral vascular disease, renal disease, gender, age at baseline, type of treatment (ranibizumab or bevacizumab), and total number of injections. The following 4 models were tested: model 1, adjusted for the treatment group; model 2, adjusted for the treatment group, age, and gender; model 3, adjusted for the treatment group, age, gender, and total number of injections; and model 4, adjusted for the treatment group, age, gender, total number of injections, diabetes mellitus, hypertension, dyslipidemia, cerebrovascular accident, and lung disease. Ranibizumab treatment was set as a reference category in the variable "treatment group." The absence of the risk factor was set as a reference category in the other covariates, e.g., no diabetes mellitus or no hypertension. The reference category for "gender" was male gender. Results are presented as hazard ratio/OR and 95% CI. Statistical significance was defined as P < 0.05.
RESULTS
A total of 916 consecutive patients were reviewed during the observation period from April 2010 to June 2011. Of the 916 patients reviewed, 66 were excluded from the study because they received both bevacizumab and ranibizumab injections. Of the remaining patients, 610 (71.8%) received bevacizumab alone and 240 (28.2%) received ranibizumab alone during the observation period. Patients who were followed-up for less than 6 months were excluded from the analysis, resulting in a total of 702 patients for all further analyses.
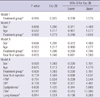
The age of the patients in the bevacizumab group (61.6 ± 12.3 yr) was lower than that in the ranibizumab group (72.2 ± 9.7 yr; P < 0.001). The gender ratio at study entry was comparable between the bevacizumab and ranibizumab groups (P = 0.057). The other baseline characteristics of the bevacizumab and ranibizumab groups are shown in Table 1. A total of 1,041 intravitreal injections (mean ± SD, 2.1 ± 1.5) were administered in the bevacizumab group, whereas 501 injections (mean ± SD, 2.5 ± 1.3) were administered in the ranibizumab group during the observation period (P < 0.001).
Major differences were not found with respect to concomitant diseases in the analysis between the bevacizumab and the ranibizumab groups, with the exception of diabetes mellitus and dyslipidemia (Table 1). Nearly 50% of the patients had hypertension. The presence of cardiovascular diseases such as angina, congestive heart failure, arrhythmia, and cerebrovascular accident were similar between the 2 groups.
The baseline characteristics of the ocular diseases with which the patients were diagnosed and for which treatment was provided are listed in Table 1. Patients received intravitreal bevacizumab injections for various retinal diseases with several causes, including diabetic retinopathy (43.5%), retinal vein occlusions (34.2%), and age-related macular degeneration (10.1%). However, only 2 ocular diseases were observed in the ranibizumab group: age-related macular degeneration (99.5%) and retinal vein occlusion (0.5%).
Systemic adverse events occurred in 10 of the 702 patients (1.4%). Of these, 7 occurred in the bevacizumab group (7/503; 1.4%), and 3 occurred in the ranibizumab group (3/199; 1.5%). This difference was not statistically significant (Fisher's exact test, P = 0.573, OR: 1.085; 95% CI: 0.278-4.237). The characteristics of the patients who experienced systemic adverse events are listed in Table 2. Gastrointestinal disorders (e.g., gastrointestinal hemorrhage, hernia, nausea) were not observed. In the bevacizumab group, most systemic adverse events occurred within 1 month after the last injection (5/7, 71.4%), while systemic adverse events occurred from 1 month up to 6 months after the last injection in fewer patients (2/7, 28.6%). In the ranibizumab group, all systemic adverse events occurred more than 1 month after the last injection, and 1 patient with a systemic adverse event had no concomitant disease.
We examined the association between the treatment group and systemic adverse events using Cox proportional hazards models. This analysis was performed on several variables to elucidate the effect of the treatment group (bevacizumab versus ranibizumab). Of the 4 models tested, none identified a covariate that significantly changed the hazard for systemic adverse events. Furthermore, a significant change in the odds for a new systemic adverse event was not found in any model when the patients in the bevacizumab group were compared with those in the ranibizumab group after controlling for the other covariates. The results of the Cox proportional hazards analysis of all 4 models for prediction of an increased risk of a systemic adverse event are shown in Table 3.
DISCUSSION
This retrospective and nonrandomized study found that systemic adverse events occurred in 7 of the 503 patients (1.4%) in the bevacizumab group and in 3 of the 199 patients in the ranibizumab group (1.5%); this was not a significant difference. The event rates that we observed are similar to previously reported findings (13-15). Although the 2 groups in our study differed with respect to age and concomitant diseases such as diabetes mellitus and dyslipidemia, they were similar in terms of systemic adverse events even after adjusting for these factors. The potentially controversial time effect issue was addressed by applying the Cox hazard regression approach, which takes into account different follow-up times (time-to-event) (Table 3). The time interval between the last injection and the systemic adverse event appears to be a very important factor, and the relationship between these 2 events can weaken with time. Herein, we observed a wide time interval range (7 days to 6 months) between the last injection and the systemic adverse event; this raises a question regarding the possible mechanism underlying development of systemic adverse events when attempting to elucidate a cause-and-effect relationship. In addition to this, multiple intravitreal injections of bevacizumab or ranibizumab did not increase the risk of systemic adverse events during the 6-month period in our study. Finally, the Cox proportional hazards model did not detect a significant covariate after adjusting for sex, age, total number of injections, and major concomitant diseases such as hypertension, diabetes mellitus, dyslipidemia, cerebrovascular accident, and lung disease through model 1 to model 4.
Concern regarding systemic exposure to anti-VEGF agents is derived from experience with intravenous bevacizumab, in which severe adverse events such as hypertension, thromboembolic events, gastrointestinal perforations, or even death have been reported (16). An analysis of 1,745 patients included in 5 randomized, controlled trials that studied options for colorectal, breast, and lung cancer treatment showed that the addition of intravenous bevacizumab to chemotherapy increased the risk of arterial thromboembolic events (ATEs) from 1.05 to 3.75 (16). In a recent review of 12,617 patients from 20 randomized clinical trials in patients with cancer, Ranpura et al. (17) found that intravenous bevacizumab significantly increased the risk of all grade ATE by 108% when compared to a control group. This risk was increased similarly in patients receiving both low and high doses of bevacizumab. Although low doses are used during intravitreal injection of anti-VEGF, the breakdown of the blood-retina barrier associated with diseases such as exudative AMD and diabetic retinopathy may lead to greater systemic anti-VEGF molecule absorption (9).
The role of bevacizumab or ranibizumab in the development of systemic adverse events remains unclear. However, from a theoretical viewpoint, the risk of development of systemic adverse events may be higher with bevacizumab than with ranibizumab. Ranibizumab has a higher affinity for VEGF than does bevacizumab, and as an antibody-binding fragment, it lacks the domain necessary to activate complement-mediated cytotoxicity or to interact with Fc receptors on immune cells (6). Therefore, bevacizumab is more likely to induce immunologic activation than is ranibizumab. Next, the systemic concentration after intravitreal anti-VEGF injection appeared to be higher for bevacizumab (59.8-86.5 ng/mL) (18) than for ranibizumab (0.3-2.36 ng/mL) (19). Thus, bevacizumab administration may constitute a higher risk of systemic adverse events. Moreover, in contrast to the pharmaceutical industry-sponsored randomized clinical trials evaluating ranibizumab, the results of the randomized clinical trials evaluating bevacizumab are of strongly limited value (8). The main limitations stem from the lack of description of rigorous monitoring of systemic adverse events and inadequate reporting of actual events (20). For example, almost of the randomized clinical trials (20-23) evaluating bevacizumab lack definite reporting methods and have an insufficient follow-up time (< 6 months) or a small number of patients (22).
Thus far, several systematic reviews have compared the effects of ranibizumab and bevacizumab. However, the previous reviews mainly focused on the beneficial effects of anti-VEGF agents without adequately addressing systemic adverse events since conclusions on systemic safety are more intricate and require a very thorough evaluation because of a methodological argument regarding the assessment of systemic adverse events (8). Recently, Curtis and colleagues (14) conducted a retrospective cohort study of 146,942 Medicare beneficiaries aged 65 yr or older treated for AMD with photodynamic therapy, intravitreal pegaptanib, bevacizumab, or ranibizumab. After adjusting for patient characteristics, they showed significantly lower hazards of all-cause mortality, incident myocardial infarction, and stroke with ranibizumab injection compared with bevacizumab injection. However, significant differences in study outcomes were not observed between the bevacizumab and ranibizumab groups after they further limited the subjects to newly treated patients in order to alleviate potential selection bias. Although the "Comparison of Age-related macular degeneration Treatment Trials" (CATT) (24, 25) and the "alternative treatments to Inhibit VEGF in Age-related choroidal Neovascularization" (IVAN) (26) trial are head-to-head bevacizumab and ranibizumab trials that are attempting to address the question of efficacy, these study were not powered sufficiently to detect drug-specific differences in rates of rare adverse events. In CATT trial (24, 25), although multiple systemic serious adverse events were observed in more patients receiving bevacizumab injections than in those receiving ranibizumab injections, these events were not associated with the system organ class identified with anti-VEGF therapy (24, 25, 27). More recently, the IVAN trial (26) showed no difference between bevacizumab and ranibizumab in the proportion experiencing a serious systemic adverse event. Additionally, these trials may not reflect the current status in actual practice because the inclusion criteria were so stringent.
We are aware that our study has several limitations, which are mainly due to its retrospective nature. Because our intravitreal injection treatment was not assigned randomly, this study had a limited statistical power to detect significant adverse events. Furthermore, the decision to use bevacizumab or ranibizumab as the anti-VEGF agent may have been related to an unmeasured confounding factor. The health insurance system in Korea was a factor of consideration in the decision to use bevacizumab or ranibizumab. Patients newly diagnosed with exudative AMD usually received ranibizumab injections because the first 5 instances of intravitreal injection of ranibizumab have health insurance benefits in exudative AMD cases. However, patients with other retinal diseases received intravitreal injection of bevacizumab because ranibizumab is much more expensive than bevacizumab. In our study, patients who received intravitreal bevacizumab injection had several different retinal diseases with various causes, including diabetic retinopathy (43.5%), retinal vein occlusion (34.2%), and AMD (10.1%). However, most patients in the ranibizumab group (99.5%) received intravitreal injection for exudative AMD. Second, systemic adverse event outcomes were not standardized prospectively. This is important to note since 6 of the 10 patients with systemic adverse events had a stroke, and 3 of the remaining patients had a cardiac disease such as angina. On the basis of the current data, it is not possible to conclude whether stroke is the most likely systemic adverse event to occur in anti-VEGF treatment or whether angina predominantly occurs during the treatment with a specific drug. Furthermore, the detection of systemic adverse events such as stroke and angina was based solely on a thorough chart review. Therefore, the rate of adverse events in our study may be lower than the actual rate of adverse events because subclinical events were undetected. For example, gastrointestinal disorders, which were reported in CATT or IVAN trial, were not detected in our study although we reviewed the chart thoroughly. Third, the 2 groups had different baseline characteristics with respect to concomitant diseases and underlying ocular diseases, although the results associated with systemic adverse events were analyzed after adjusting for these different factors. Therefore, our results should be interpreted with caution because several ocular diseases were included in the bevacizumab group, and the composition of diseases was quite different from that of the ranibizumab group. Another limitation of our study is the relatively short follow-up, which precludes estimation of the long-term safety of intravitreal anti-VEGF injection. Finally, our predictors were mostly classified in a binary fashion (e.g., diabetes mellitus: yes or no or hypertension: yes or no) rather than in more detail (e.g. type of diabetes, duration of diabetes, use of insulin, or HbA1c level).
In conclusion, although the risk for development of systemic adverse events may be higher with bevacizumab than with ranibizumab from a theoretical viewpoint, the present study demonstrates that there is no difference between bevacizumab and ranibizumab in terms of the risk of systemic adverse events among patients who receive intravitreal ranibizumab or bevacizumab.

 XML Download
XML Download