

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Behcet's disease (BD) is a chronic, systemic vasculitis of unknown etiology, characterized by orogenital ulcers, uveitis, and arthritis, and is most prevalent in Korea, China, Japan and Turkey (1). Although the pathogenesis of BD remains unknown, several lines of evidence have suggested that host genetic factors play a pivotal role in determining susceptibility to BD (2-4).
Copy number variation (CNV) is defined as deletions or duplications of DNA segments larger than 1 kilobase and up to several megabases in size that are present in variable copy numbers compared to a reference genome (5). Such duplications or deletions of genes or regions that control specific gene expression would be likely to influence protein expression. Consequently, CNV may influence the susceptibility to diseases or the response to environmental factors. CNV has been associated with complex disease traits, such as susceptibility to systemic lupus erythematosus (SLE), and rheumatoid arthritis (RA) (6-8).
Previous studies reported that trisomy 8 is associated with severe and full-blown manifestations, such as intestinal ulceration and high fever, in BD patients with bone marrow failure (BMF) (2, 9). It was suggested that one of the candidate genes of chromosome 8 may be implicated in the pathogenesis of BD.
Neutrophils play a central role in the innate immunity and are known to be hyperactive in BD (1, 10). They possess a set of granules that contain many antimicrobial peptides, including defensins. Genes of defensins are located in a cluster on chromosome 8 and encode antimicrobial peptides that play a role in innate immunity (11). Defensins consist of three main subfamilies, α-, β and θ-defensins and α-defensins are released into the extracellular milieu from neutrophils during inflammation, resulting in induction and aggravation of inflammatory reactions (11).
From these findings, it was inferred that the copy number (CN) of the DEFA1 gene may influence the development or aggravation of clinical manifestations in BD patients. To test this hypothesis, we investigated the CN of the DEFA1 gene in samples from Korean individuals with BD.
The experimental protocols used in this study were approved by the institutional review board of the Kangbuk Samsung Hospital (#KBC10108). Informed consent was obtained from all BD patients and healthy volunteers. For CNV analysis, 55 samples (34 men, 21 women) from Korean BD patients and 35 ethnically- matched control samples (10 men, 25 women) were recruited. Patients fulfilled the diagnostic criteria of the international BD study group (12). Healthy control subjects were medically healthy by history and examination. Of those, we also excluded the subjects with BD related symptoms such as oral or genital ulceration. The demographic and clinical data were obtained from the medical records of patients.
Gene CN was determined by a duplex Taqman® real-time PCR assay (Applied Biosystems, Foster City, CA, USA) following the manufacturer's instructions. The gene CN assay was run as a duplex Taqman® real-time PCR reaction with the RNase P gene as a reference gene. The 10 µL reaction mixture consisted of 5 µL (2 ×) Taqman® universal PCR mastermix, 0.1 mL Amplitaq Gold, 2.5 µL dH2O, 0.7 µL RNase P primer/probe mastermix (22.5 µM primers and 5 µM probe), 0.7 µL DEFA1 primer/probe mastermix (5.63 µM primers and 1.25 µM probe; Forward: 5'-GGATGTCCGCTGCAATCTG-3', Reverse: 5'-GCCATCCTTGCTGCCATTC-3'; FAM Reporter: 5'-CAGCAACCTCATCAGCTCTT-3') and 15 ng DNA (1 µL). Using a standard curve for each gene, the number of DEFA1 copies was calculated as the relative relationship between the signals from DEFA1 and the reference gene. The number of copies of the DEFA1 gene sequence in each test sample was determined by relative quantitation using the comparative CT (ΔΔCT) method. This method measured the CT difference (ΔCT) between target and reference sequences and then compared the ΔCT values of test samples to a calibrator sample known to have two copies of the target sequence. All samples were analyzed in triplicate. Relative quantitation analysis was performed using CopyCaller™ Software (Applied Biosystems).
Statistical comparison between the groups was performed using Student's t-test, and chi-squared-test. Logistic regression analyses were performed to estimate the odds ratio (OR) adjusted for age and sex. P values less than 0.05 were considered statistically significant. The PASW statistics software package (version 17.0, SPSS Institute, Chicago, IL, USA) was used for all analyses.
The mean ages ( ± standard deviation) of BD patients and healthy controls were 44.2 ( ± 9.3) and 45.2 ( ± 12.9) yr, respectively. Among BD patients, erythema nodosum was the second most common clinical finding (63.6% of patients), followed by genital ulcers (61.8%), arthritis (40.0%), vascular involvement (36.3%), ocular involvement (23.6%), and intestinal involvement (10.9%).
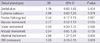
Overall, most samples (31.1%) had a CN of 5 with a mean CN of 5.4 ± 0.2. There was no significant difference in the DEFA1 CN between BD patients and healthy control subjects (mean CN 5.3 ± 0.2 vs 5.5 ± 0.3 copies, P = 0.883, Fig. 1). There was no significant difference in DEFA1 CN between male BD patients and healthy male controls (P = 0.956) or between female BD patients and healthy female controls (P = 0.505). There was no significant association between the DEFA1 gene CN and clinical features (Table 1). However, we found that a high DEFA1 CN was significantly associated with intestinal involvement in BD patients (OR = 2.86, 95% confidence interval 1.37-5.94, P = 0.005). Intestinal involvement was found in six patients with BD, who had 5, 6, 7, 8, 9, and 10 copies of the DEFA1 gene, respectively. In our experiment, three BD patients had complications of BMF, trisomy 8 in their bone marrow and intestinal involvement, and their copy number was 6, 7, and 9 copies, respectively.
Host genetic factors are thought to influence susceptibility to BD. Behcet's disease, also known as the Silk Road disease, is strongly associated with HLA-B51 (4). It was reported that the higher concordance rate of monozygotic twins compared to dizygotic twins suggests significant genetic influences on the development of BD (3). We previously reported that intestinal involvement and full-blown features of BD were common in patients with BMF who had trisomy 8 in their bone marrow (2), suggesting that candidate genes associated with the development of BD may be located on chromosome 8. Defensin genes form a cluster at 8p23 and CNs of DEFA1 gene and seven β-defensin genes on chromosome 8 are known to vary in normal subjects (8, 13, 14). α-defensin-1 is the most abundant isoform of α-defensins in neutrophil granules. Since the DEFA1 gene encoding α-defensin-1 on chromosome 8 was a possible candidate contributing to the risk of BD, we examined the CNV of the DEFA1 gene in BD patients compared with healthy controls, and sought to determine the association between the CN of the DEFA1 gene and clinical BD phenotypes.
As shown in Fig. 1, we found that the DEFA1 gene showed common CNV between 2 and 9 copies per diploid cell in BD patients and healthy controls, with occasionally CNs as high as 10 in BD patients. Our results showed that the DEFA1 gene CN was not significantly different between BD patients and healthy controls. A similar report found that the mean copy number for α-defensins gene among 14 BD patients (mean CN of 5.1 copies) was not significantly different compared to the 121 unaffected controls (mean CN of 6.8 copies) in the UK (9). In accordance with previous studies (9, 13), the DEFA1 gene in our samples appeared to be present in high CNs in both Korean patients with BD and healthy controls, and no significant difference in the DEFA1 CN was observed between the two groups. Our study demonstrated that a higher DEFA1 gene CN was significantly associated with BD patients with intestinal involvement compared to those without intestinal involvement, suggesting that a high DEFA1 CN may contribute to intestinal involvement in BD patients. High CNs of DEFA1 gene were closely related to the level of α-defensin-1 expression (14). α-defensins confer not only antimicrobial effects such as microbicidal or antiviral activity, but also have an immune-enhancing or cytokines-inducing effect similar to that of tumor necrosis factor-α and interleukin-1 (15, 16). Also, α- and β-defensins are important in immune activation in the epithelial surface (11). From these findings, it is conceivable that the high CN of the DEFA1 gene and the subsequent increase in α-defensin-1 expression might initiate or amplify the inflammatory reaction in the intestine of BD patients. Accordingly, high DEFA1 gene CN may be associated with susceptibility to intestinal involvement in patients with BD. Similar to the present results, it was recently reported that high α-defensins CN is significantly linked to the inflammation of colonic Crohn's disease (17). Some authors have reported that inflammatory bowel disease (IBD) and BD may be part of a spectrum of disease rather than distinct disease entities (18). Considering these findings, α-defensins CNV may be one of the pathogenic mechanisms common to development of IBD and intestinal BD.
BD patients with positive pathergy tests had lower DEFA1 CNs than those with negative tests, although this difference was not statistically significant. Considering the fact that neutrophil infiltration and activation are increased in pathergy reactions, or pustules (19), our result was unexpected. We note that our finding may be partly due to the small number of patients in each of our study groups.
In conclusion, variable CNs of the DEFA1 gene have been observed in both BD patients and healthy controls and high DEFA1 CNs may be associated with susceptibility to intestinal involvement in BD. Further studies will be required to determine the reproducibility of our findings in larger patient groups and different study populations.

 XML Download
XML Download