

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Knee pain is a common musculoskeletal problem in elderly, and its prevalence increases with age (1). Knee pain leads to physical disability and decreased quality of life (QOL) (2). Osteoarthritis (OA) is a leading cause of knee pain and physical disability in the elderly, and knee pain derived from OA is a key symptom influencing the decision to seek medical attention (3). On the other hand, it has been consistently reported that radiographic OA changes are poorly correlated with pain and physical function (3-5). Recent studies suggest that knee pain is a better predictor of disability than radiographic change (5). Moreover, risk factors for radiographic knee OA may not be the same as those for knee pain (6). Nevertheless, previous studies have focused mostly on the relationship between knee OA and physical function rather than between knee pain and the latter (5, 7).
In this cross-sectional study, we investigated the prevalence of knee pain and its influence on the QOL and physical performance in community-dwelling older adults in Chuncheon, Korea. Gender differences in the influence of knee pain on QOL and physical function were also examined.
MATERIALS AND METHODS
Subjects
Data were obtained from the Hallym Aging study (HAS). HAS is a prospective cohort study of health among elderly community-dwelling residents of Chuncheon, a city about 120 km east of Seoul. This ongoing study began in 2004, with follow-up examinations planned every 3 yr. The methods have been described elsewhere in detail (8). Briefly, eligibility criteria include age of 50 yr or older and residence within the borders of the survey area for at least 6 months before the survey. Using Korean National Census data for the year 2000, 200 of 1,408 census tracts were randomly sampled according to residential area (9). Study subjects were selected so that those over 65 yr old represented about 70% of the study cohort. This study involved subjects from the second triennial examination. Of the 702 eligible participants, 129 subjects declined knee radiographs and 69 subjects were excluded due to poor knee radiograph quality (n = 4), total knee replacement surgery (n = 3), or missing films due to clerical error (n = 62). Those who declined to take radiographs were significantly older than the subjects who participated. The remaining 504 subjects were analyzed for this study.
Data collection
Demographic information was collected using a standard questionnaire, which included educational attainment, marital status, household income, occupation, and comorbidities. Work demanding physical exertion (e.g., sometimes carrying heavy objects, using instrumentation) or heavy physical exertion (e.g., construction worker, laborer, farmer) were defined as a manual occupation. Comorbidity health information was self-reported according to a closed questionnaire listing 29 pre-defined illnesses. Height (cm) and body weight (kg) were measured to the nearest 0.1 cm and 0.1 kg, respectively, with the subject wearing light clothing and barefooted for calculation of the body mass index (BMI).
Knee pain was assessed by asking, "Have you had pain, aching, or stiffness lasting at least a month in your knee?" All subjects also completed the Korean version of Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), a cross-culturally adapted and validated instrument that measures knee pain and physical function in persons with knee OA (10), and the Short Form 12-item (SF-12) questionnaire for the evaluation of self-reported functional status and QOL.
Physical performance test
Physical performance of lower extremity was tested using the Health-ABC battery, as reported previously, with modifications (11). Briefly, standing balance, a 6-m usual walk, and five repeated chair stands were tested. To test standing balance, the subjects were asked to attempt to keep their feet in side-by-side, semitandem, and tandem positions for 10 sec each. The subjects were given a score of 0 if they could hold a side-by-side standing position for 10 sec but were unable to hold a semi-tandem position for 10 sec, a score of 1 if they could hold a semi-tandem position for 10 sec but were unable to hold a full tandem position for more than 2 sec, a score of 2 if they could stand in the full tandem position for 3 to 9 sec, and a score of 3 if they could stand in the full tandem position for 10 sec. For the 6-m usual walk test, a 6-m walk at the subject's normal pace was timed twice, and the time of the faster of the two walks was used for scoring. For repeated chair stands, the subjects were asked to fold their arms across their chests and to stand up and sit down five times as quickly as possible, and the length of time required was measured. For repeated chair stands and 6-m usual walks, we created quartiles based on the performance of the study subjects, with quartile 0 representing the worst and quartile 3 representing the best performance. Research nurses trained in lower extremity performance test carried out the assessments. To avoid inter-assessor variability, one nurse took charge of one item of the test of all participants. Previously, test-retest correlations of more than 0.89 for walking speed (12), 0.73 for chair stand (13) and 0.97 for standing balance (14) have been reported for these measures.
Radiographic assessment
Radiographic evaluations consisted of weight-bearing anteroposterior, 14 × 17-inch, semi-flexed knee radiographs. Each knee was graded using the Kellgren and Lawrence (K-L) grade (15). Radiographic knee OA was defined as being present if the subject had a radiographic grade in the tibiofemoral joint of ≥ K-L grade 2. Radiographs were read twice by one reader, an academically based rheumatologist. Films allocated different K-L grades at the two readings were adjudicated by consensus between the original reader and a second reader, another academically based rheumatologist. The reproducibility of intra-reader assessments was high (for OA vs no OA, κ = 0.89).
Statistical analysis
Subjects were divided into four age groups: 50-59 (n = 56), 60-69 (n = 126), 70-79 (n = 274), and ≥ 80 yr (n = 48). The age-specific prevalence of knee pain was calculated for men and women. Student's t test and chi-square tests were used to compare the subjects with or without knee pain. Logistic regression models with generalized estimating equations (GEE) were used to calculate the odds ratios (ORs) for the presence of knee pain. GEE were used to minimize the lack of independence between measures originating from the same individual. In multivariate GEE analysis, an adjusted OR was calculated after adjusting for age and factors found to be significant in univariate analysis. Because a sizable majority of subjects marked 0 for WOMAC subscales, the subscales were categorized into quartiles 0-3 with quartile 3 representing the worst scores. The ORs and 95% confidence interval (CI) for belonging to the worst quartile of WOMAC were calculated by logistic regression analysis in subjects with knee pain compared to subjects without knee pain after adjusting for age, BMI, sex, and the presence of knee OA. In addition, sex-specific quartiles were created and analyzed to separately compare male and female subjects, respectively. Scores for SF-12 items were analyzed and compared using general linear models after adjustment for age, sex, BMI, and the presence of knee OA between subjects with and without knee pain. The proportion of subjects belonging to each category of physical performance test was compared between subjects with and without knee pain using chi-square test. Data were analyzed using SAS software version 9.1 (SAS Institute, Cary, NC, USA). P values < 0.05 (2-tailed) were considered statistically significant.
Ethics statement
This study was approved by the institutional review board of the Hallym University School of Medicine (IRB approval number: HIRB-2007-001). All participants agreed to the use of their health check-up results including blood sample, physical performance test and knee radiographs. Written informed consent was obtained from each participant.
RESULTS
Characteristics of the study subjects
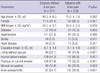
Of the 504 participants, 54% were women and the mean age was 70.2 yr. The demographic and clinical characteristics of the study population are shown in Table 1.
Those with knee pain were more likely to be female. The subjects with knee pain had a significantly lower level of education, lower income, higher BMI, and higher frequency of manual occupation and living without a spouse. Of the subjects with knee pain, 55.8% had radiographic knee OA.
Prevalence and risk factors of knee pain
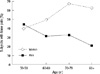
The overall prevalence of knee pain was 46.2% (32.2% in men and 58.0% in women, P < 0.001). In 10.3%, 9.1% and 26.8% of subjects, pain was present in right, left or both knees, respectively. The prevalence of unilateral knee pain in dominant leg was 10.4% and 16.1% in right and left knees, respectively. Fig. 1 shows the age-specific prevalence of knee pain in men and women. Except for subjects under the age of 60 yr, the prevalence of knee pain was significantly higher in women than in men. The prevalence increased with age in women until 70 yr then leveled off (P < 0.001 for trend). The prevalence of knee pain did not increase with age in men, and the mean age of subjects with knee pain was not significantly different from that of subjects without knee pain (Table 1).
In univariate analysis, knee pain was associated with female gender, higher BMI, lower educational level, non-smoking, manual occupation, living without a spouse, lower income, and the presence of radiographic knee OA (Table 2). None of these variables had significant correlations with each other (Pearson correlation < 0.5, data not shown), thus, multivariate analysis was performed after adjusting for age and all of those significant factors. After multivariate GEE analysis, female gender (OR = 2.82, 95% CI = 1.47-5.40) and the presence of knee OA (OR = 2.81, 95% CI = 2.02-3.89) were significantly associated with knee pain. Knee OA was significantly associated with knee pain in both genders with adjusted ORs of 2.44 (95% CI = 1.31-4.53) and 2.92 (95% CI = 1.96-4.36) in men and women, respectively. Among subjects with knee OA, 47.2% of men and 70.2% of women had knee pain, while among those without knee OA, 29.4% of men and 40.7% of women had knee pain. Women had significantly higher ORs for knee pain compared to men in both radiographic OA and non-OA groups (adjusted ORs, 3.22 [95% CI = 1.66-6.24] and 1.94 [95% CI = 1.28-2.96], respectively).
Physical function and QOL as measured with WOMAC and SF-12 in subjects with knee pain
To compare the pain, stiffness, and function as measured with WOMAC between subjects with and without knee pain, we performed logistic regression analysis to estimate ORs for belonging to the worst quartile (Table 3). After adjusting for age, sex, BMI and the presence of knee OA, subjects with knee pain had significantly increased risk of belonging to the worst pain, stiffness, and function quartile compared to subjects without knee pain. In both men and women, knee pain was correlated with worse WOMAC scores compared to those without knee pain. Among subjects with knee pain, women had significantly higher risk for belonging to the worst quartile for all WOMAC subscales compared to men after adjustment of age, BMI, and the presence of knee OA.
The mean scores for the SF-12 items are shown in Table 4. Similar to the WOMAC results, subjects with knee pain had significantly worse (lower) scores on all SF-12 subscales than did subjects without knee pain after adjusting for age, sex, BMI, and the presence of knee OA in both genders. Among those with knee pain, women had worse SF-12 scores in all categories except for general health perception and social functioning in comparison to men.
Physical performance test in subjects with knee pain
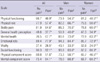
We compared the proportion of subjects belonging to each category of Health-ABC battery according to the status of knee pain (Table 5). The subjects with knee pain had worse scores on all tests than subjects without knee pain, and knee pain was significantly associated with poorer physical performance. While female subjects with knee pain had significantly worse functional categories compared to those without knee pain in all tests, male subjects with knee pain did worse in usual walk test only. Although standing balance was not influenced by gender, men performed significantly better on usual walk (mean 6.0 vs 6.9 sec in men vs women), and repeated chair stands (mean 11.91 vs 13.40 sec in men vs women). Regarding this as inherent gender difference, we did not compare the lower extremity function between men with OA and women with OA.
DISCUSSION
The present study found that the overall occurrence of knee pain in an elderly Korean community was 46.2%, with a higher percentage reported in women than in men. ORs for knee pain were significantly higher in females and in subjects with knee OA after adjustment of confounding factors. Knee pain was correlated with substantial reduction of physical function and QOL and lower-extremity physical performance, as measured with the WOMAC, SF-12 and Health-ABC tests. Women had worse WOMAC and SF-12 scores compared to men.
The occurrence of knee pain has been reported previously in diverse Caucasian populations. In older adults in the UK, 25%-47% had knee pain (2, 16), while in Australia, 52% of women aged 70 and older reported knee pain and in US adults aged 45-74, 10% of women and 12.7% of men had knee pain (6). However, there are relatively few data on the prevalence of knee pain among elderly populations in Asia. Among Chinese residents aged ≥ 70 yr of age, 27% of men and 48% of women experienced knee pain (17), while 41% of Japanese women between the ages of 60-79 had knee pain (18). Despite the fact that a strict comparison of prevalence is not possible due to the differences in age or definition of knee pain, the subjects in our cohort generally had a higher rate of knee pain than the Caucasian populations discussed in previous studies. Possible reasons for the difference include genetic, environmental, and cultural factors including lifestyle behaviors such as squatting and kneeling.
Age as a risk factor for symptomatic knee OA has been recognized (19, 20). In this study, the prevalence of knee pain increased with age in women but not in men. In the elderly females, knee pain may more often be the consequence of factors associated with aging, such as reduced physical activity, or muscle weakness compared to men.
The strong relationship between knee pain and female gender is consistent with previous reports (2, 8, 20-22). In our study, women had significantly higher ORs for knee pain compared to men among subjects both with and without knee OA. However, the presence of knee OA posed comparable risk for knee pain in both genders (adjusted OR 2.44 vs 2.92 in men and women, respectively). On the other hand, in a study investigating knee OA and pain among elderly Japanese subjects, the association between knee pain and advanced radiographic OA (≥ 3 K-L grade) was stronger among men compared to women, implying that knee pain may arise from locations other than joint cartilage in women (23). Although the presence of radiographic knee OA increased the OR for knee pain, only 66% of our subjects with knee OA reported knee pain. This finding correlates with a previous finding that in adults with radiographic knee OA, the prevalence of pain ranged from 15%-81% (4). Pain perception is complex and knee pain may be the result of non-OA problems, such as psychosocial factors, education, marital, or economic status rather than local pathology (6, 20, 24).
Our results showed that subjects with knee pain scored worse on all WOMAC and SF-12 subscales compared to subjects without knee pain, even after adjusting for age, sex, and the presence of OA. This is in line with previous results, which showed that knee pain was associated with poor QOL and physical function (25). Therefore knee pain, independent of knee OA, may be associated with disability. We also found that women with knee pain had significantly worse scores on all WOMAC subscales and on almost all physical and mental domains of SF-12 compared to men. Mechanical, environmental, and psychosocial factors including economic or education level, physical activity, muscle strength, pain coping skills, and social support may account for gender difference in functional status and QOL measures(3, 7, 26-29).
A few tests including a 6-min walk, a stair climb, a lifting and carrying task, and ambulatory-based performance tasks have been validated and used to evaluate physical activity in patients with knee OA or knee pain (29, 30). We used the physical performance test including standing balance, usual walk and chair stands. We found that knee pain had a greater impact on physical performance in women compared to men. This implies that knee pain affects lower extremity function more adversely in women. With the chi-square test that we used, it was not possible to adjust age or knee OA. We compared the proportion of subjects belonging to each category of Health-ABC battery according to the status of knee OA (data not shown). The subjects with knee OA had worse scores on all tests than subjects without knee pain. Thus, the possibility that lower extremity function measured by this battery is influenced more by factors other than knee pain, such as aging or knee OA cannot be ruled out.
This is the first population-based study on the influence of knee pain on physical performance in an Asian elderly population, using knee-based analysis to estimate risk factors for knee pain. Knee-based analysis can eliminate potential confounding bias by presuming that because each subject had two knees, all person-level confounders would be equally distributed between both knees. In addition, physical performance test as well as questionnaires was used to evaluate the functional aspect of knee pain. On the other hand, our study is limited by the small sample size and a cross-sectional study design. In addition, only anteroposterior knee radiographs were performed-therefore, patellofemoral OA could not be evaluated. About the WOMAC, we checked pain and stiffness separately. Although only 5 subjects (1%) had knee stiffness without pain, it may be problematic for subjects to differentiate knee pain and knee stiffness.
In conclusion, the prevalence of knee pain is high (32.2% in men and 58.0% in women) in this elderly community-dwelling population in Korea, and it tends to be higher compared to that reported previously in Caucasian populations. Independent of knee OA and other confounding factors, subjects with knee pain have more than 5-fold increase in the risk of belonging to the worst lower extremity function compared to subjects without knee pain. In addition, subjects with knee pain have SF-12 scores 10%-30% lower than subjects without knee pain after adjusting confounders, reflecting lower QOL. Women are more adversely affected than men. Prevention and early intervention of knee pain in older adults should be a high public health priority.



 XML Download
XML Download