

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lung cancer is the leading cause of cancer mortality worldwide for both men and women (1). Pulmonary resection remains the mainstay of curative treatment option for patients with lung cancer. However, the patients undergoing lung cancer surgery are high risk group for pulmonary complications because they have comorbidities such as chronic obstructive pulmonary disease (COPD), histories of heavy smoking, and other coexisting medical conditions (2), and possibility to develop further hypoventilation induced by pulmonary amputation.
Although the operative mortality after lung resection have decreased over the past decades (3), the mortality rate from postoperative pneumonia (POP) following lung cancer surgery remain significant. The incidence of POP after lung surgery has been reported to range from 2.1% to 40% and the associated mortality rate has ranged from 30% to 46% (4). These wide variations among studies may be explained by the heterogeneity of the studied populations in the type of resection or use of prophylactic antibiotics, as well as the differences in the definition of POP.
Age, extent of resection, low FEV1%, advanced pathologic stage, induction therapy, or COPD have been shown to be associated with POP (4-6). In addition, a previous study attempted to produce a validated risk index that predicts risk for pneumonia (7). However, these studies either included patients operated for pulmonary diseases other than lung cancer (4, 7) or included pulmonary complications other than POP as their outcome variable (2, 3). Some recent studies focused on the impact of bronchial colonization of community-acquired pathogens such as Haemophilus influenzae and Streptococcus pneumoniae (4, 5) on POP rather than the identification of the risk factors of POP after lung cancer surgery through detailed review of clinical information. Therefore, it remains difficult to predict who will develop POP after lung cancer surgery.
The purpose of this study was to investigate the risk factors of POP after lung cancer surgery. In this study, we tried to review detailed clinical information.
MATERIALS AND METHODS
Study subjects and design
We screened 454 consecutive patients undergoing lung cancer surgery from September 2007 to February 2009 at a tertiary referral hospital (Seoul National University Hospital, Seoul, Republic of Korea). Among those patients, 417 with pathologically confirmed primary lung cancer were included. Patients who had alternative diagnosis other than primary lung cancer were excluded.
We performed a retrospective cohort study to identify the risk factors of the POP following the surgical resection for lung cancer. Clinical, radiological and laboratory data were reviewed. We compared the variables between patients who did or did not have POP.
Variables and definitions
POP was defined by the presence of a new or progressive infiltrate on chest radiography or computed tomography during the patient's hospitalization, together with any of the following: new onset purulent sputum, change in character of chronic sputum, fever ≥ 38℃, a new rise in C-reactive protein value or WBC count, positive blood cultures, or isolation of pathogen from sputum, transtracheal aspirate or bronchial washing. Empyema was defined as purulent effusion in the postoperative thoracic cavity (4, 8).
We classified combined resections with the chest wall, pericardium, great vessels, left atrium, vertebral bodies, or diaphragm as extended resection. Pathological stage was assessed by the AJCC TNM staging system for lung cancer (6th edition, 2002).
Postoperative complications other than pneumonia included atelectasis, bronchopleural fistula (BPF), chylothorax, prolonged air leakage, subcutaneous emphysema, wound infection and vocal cord palsy. Prolonged air leakage was defined as air leak requiring > 7 days of postoperative chest tube drainage (9).
Preoperative, intraoperative, and postoperative variables were reviewed including demographic data, type of anesthesia, induction therapy, history of previous operations, comorbidities, and postoperative complications other than pneumonia. Eversmoker included current and former smokers. The comorbid conditions were also estimated on the basis of the Charlson's comorbidity index and were divided into two groups, score 0 and score 1 or more (10).
Statistical analysis
In univariate analyses, continuous variables were analyzed using nonparametric test (Mann-Whitney U test) and categorical variables were compared by the Pearson's chi-squared or Fisher's exact test, as appropriate. Multivariate analyses using binary logistic regression was performed to evaluate the risk factors of POP. We created a multivariate analysis model using significant variables as determined by the univariate analysis and suggested risk factors of POP. The SPSS software version 17.0 (SPSS Institute, Inc., Chicago, IL, USA) was employed for statistical analysis. A P value less than 0.05 was considered to be significant.
RESULTS
Four-hundred fifty four patients who underwent pulmonary resection under the impression of primary lung cancer were considered for enrollment. Among these patients, 37 were excluded from the analysis because they had alternative diagnosis other than primary lung cancer; 13 with metastatic lung cancer, 7 with tuberculosis, 5 with inflammatory lesion, 3 with aspergillosis, 2 with atypical adenomatous hyperplasia, and 7 with other benign lesions. Finally, a total of 267 men and 150 women (median age 65 yr) was included in the analysis. The demographic and clinical characteristics of the enrolled patients are described in Table 1. Surgical resections were performed by the same surgical team according to standard techniques. Extended resection were needed in 31 patients (7.4%) (Table 1). All patients received pain control with patient-controlled epidural or intravenous analgesia after surgery.
The incidence of POP was 6.2% (26 of 417). POP developed median 4 (1-19) days after surgery. Empyema developed in 3 patients, and among them, 2 had both POP and empyema. Patients with POP frequently required mechanical ventilation (42.3%), and had a higher rate of acute respiratory distress syndrome (ARDS, 34.6%) and in-hospital mortality (27%) (Table 2). One patient without POP died of postoperative ARDS. Among patients without POP, 3 received mechanical ventilation for poor cough strength combined with sputum retention, postoperative cardiac arrhythmia, and ARDS.
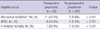
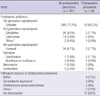
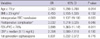
All patients received perioperative antibiotic prophylaxis. Cephalosporin was used in 404 patients (96.9%); 1st generation (cefazolin) in 304 patients, 3rd generation (cefodizime, cefpiramide, cefrtriaxone, cefotaxime, or cepfodoxime) in 55, and 4th generation (flomoxef) in 36. Quinolone (ciprofloxacin, levofloxacin, or moxifloxacin) and vancomycin were used in 12 (2.9%) and 1 (0.2%) patients respectively for the following reasons: previous history of obstructive pneumonitis and known allergy to cephalosporin. The results of microbiological tests in enrolled patients are summarized in Table 3. The pathogens were isolated from sputum (n = 5, 19%), endotracheal aspirate (n = 4, 15%), blood culture (n = 1, 4%), bronchial washing (n = 3, 12%), or pleural effusion (n = 3, 12%). There were no significant differences in development of POP between the prophylactic use of 1st generation cephalosporin and that of other antibiotics (P = 0.642). In univariate analysis, age ≥ 70 yr, male sex, ever-smoker, anesthesia time ≥ 4.2 hr (median value), intraoperative red blood cells (RBC) transfusion, presence of postoperative complications other than pneumonia, forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) < 70%, diffusing capacity of the lung for carbon monoxide (DLCO) < 80% predicted and preoperative levels of serum C-reactive protein ≥ 0.15 mg/dL (median value) were related with risk of POP (Tables 4, 5). Multivariate analysis showed that age ≥ 70 yr, intraoperative RBC transfusion, the presence of postoperative complications other than pneumonia, and FEV1/FVC < 70% were independent risk factors of POP after lung cancer surgery (Table 6).
DISCUSSION
In our study, POP occurred in 26 (6.2%) of 417 patients who underwent lung cancer surgery. Patients with POP frequently required mechanical ventilation and had higher rate of postoperative ARDS and in-hospital mortality (26.9%). The present study revealed that intraoperative RBC transfusion was an independent risk factor of POP after lung cancer surgery. In addition, this study confirmed several risk factors suggested in the previous studies; advanced age, male sex, DLCO, active smoking, and anesthesia time (7, 9, 11). However, some other risk factors such as pathologic stage, extent of surgical resection or neoadjuvant chemotherapy had no relevance to POP in our study.
The mortality rate of patients with POP in this study was similar to previously reported mortality rate of 25% (12). In our study, POP was attributable for 7 of 8 postoperative mortality, 11 of 14 mechanical ventilation, and 9 of 10 ARDS among all the 417 enrolled patients. This indicates that POP constitutes a critical issue in patient management after lung cancer surgery.
To the best of our knowledge, this was the first report that intraoperative RBC transfusion was an independent risk factor of POP after lung cancer surgery. It has been shown that perioperative blood transfusion could result in postoperative immunosuppression, which may contribute to the development of infectious complications (7, 13-17). The transfusions were associated with preoperative anergy and, with depressed lymphocyte responses to phytohemagglutinin, pokeweed mitogen, and concanavalin A for up to 4 weeks postoperatively, which increases risk of postoperative infections (15, 18). In addition, long-term transfusion is known to be associated with inverted helper-to-suppressor T-cell ratios and, with reduced natural-killer cell cytoyoxicity (19).
In the multivariate analysis of this study, age ≥ 70 yr was an independent significant risk factor of POP. Shiono et al. (6) showed that age ≥ 75 yr was an independent significant risk factor for postoperative pneumonia and empyema. Similarly, Iwamoto et al. revealed that elderly patients ≥ 65 yr who underwent thoracic surgery showed the highest incidence of pneumonia (20).
We found an additional significant risk factor of POP as the presence of postoperative complications other than pneumonia. Shiono et al. (6) reported that BPF occurred in 1% of the patients undergoing lung cancer surgery, and most of them were associated with empyema. In our study, 2 patients who underwent pneumonectomy developed BPF, and all of them died of POP. In addition, 2 patients with prolonged air leakage developed POPs on the 8th and 19th day after surgery, respectively, and the latter received pleurodesis on the 30th day. Postoperative atelectasis was associated with poor sputum expectoration, resulting in POP.
Another result of the present study corresponded with the earlier studies which reported that patients with COPD have an increased risk of postoperative pulmonary complications (21, 22). A reduced FEV1/FVC ratio is an indicator of airway obstruction. For these patients with impaired respiratory pulmonary function, combinations of bronchodilators, physical therapy, smoking cessation, and corticosteroids might be needed to reduce the risk of postoperative respiratory complications (22).
Antimicrobial prophylaxis is given routinely in thoracic surgery (23). However, there are no specific guidelines regarding antibiotic prophylaxis for pulmonary surgery, and the agents applied are the same antibiotic prophylactic regimen as for cardiac surgery; e.g., 1st- and 2nd-generation cephalosporins (24, 25). In previous randomized trial of patients undergoing thoracic surgery, cefazolin therapy was associated with a significant reduction in wound infection but not in empyema or pneumonia (26). Recently, it has been proposed that prior airway colonization could be a potential risk factor for postoperative infections, and in this context, new strategies of antibiotic prophylaxis for these potential pathogens has been offered (4, 5, 27). However, the correlation between the germs responsible for preoperative colonization and subsequent POP was not clear. In recent retrospective study of 626 patients undergoing lung cancer surgery, it was suggested that Staphylococcus aureus and Gram-negative bacilli should be included in targets for postoperative prophylactic antibiotic selection (11).
For this reason, we devided prophylactic antibiotics into 2 groups; 1st-generation cephalosporin and others. The latter included 3rd- and 4th-generation cephalosporins and quinolones which could cover a broad spectrum of Gram-negative as well as Gram-positive pathogens. However, there were no significant differences in POP incidence between both groups in our study. Microbial pathogens were identified in 9 of 26 (35%) patients with POP. Most of these were resistant strains such as methicillin-resistant Staphylococcus aureus (MRSA). These results were in accordance with those of recent study, in which the majority of POP was sustained by bacterial species more frequently associated with truly hospital-acquired pneumonia (11).
This study has potential limitations. First, it was a retrospective study with a small sample size. Second, microbiological diagnosis could not be confirmed in most patients, although there were attempts to identify the microbial pathogens in all the POP patients. Finally, variable prophylactic antibiotics were used, so there was a lack of consistency in antibiotic prophylaxis.
In conclusion, we identified risk factors of POP in lung cancer surgery. Postoperative pneumonia after lung cancer surgery is associated with higher mortality rate. Therefore, careful attention should be paid to those patients with advanced age, intraoperative RBC transfusion, postoperative complications other than pneumonia and a decreased FEV1/FVC ratio.



 XML Download
XML Download