

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The incidence of bloodstream infections with fungi (especially Candida species) has increased substantially during recent decades (1). One study revealed that the incidence of candidemia increased from 1.25 episodes per 10,000 patient days per year in 1999 to 3.06 episodes per 10,000 patient days per year in 2003 (2). In the United States, Candida species are the fourth highest cause of nosocomial bloodstream infection (3). Moreover, the overall mortality of patients with a blood culture positive for Candida species ranges from 31% to 81% (4-11).
Although antifungal agents have recently been developed and are widely used, the incidence of candidemia and its associated mortality are increasing, especially in patients with severe underlying diseases (12). This trend is associated with an increase in the number of patients who receive immunosuppressive agents after antineoplastic or antirejection chemotherapy (13, 14). The known risk factors for candidemia are immunosuppression, neutropenia, hemodialysis, long-term use of a central venous catheter, previous broad-spectrum antibiotic use, and Candida colonization (1, 13). As these risk factors are common among intensive-care unit (ICU) patients, ICUs are high-risk environments for candidemia.
There are few recent studies on the epidemiology of candidemia in medical ICUs (MICUs). Therefore, we undertook a case-control study of MICU patients to evaluate their clinical characteristics, including the incidence of candidemia, the predominant infectious organisms present, mortality, and risk factors for candidemia in an MICU.
MATERIALS AND METHODS
Study design and patients
We performed a retrospective 1:3 matched case-control study. The study was conducted at the Seoul National University Hospital, a tertiary care center in Korea. Seoul National University Hospital has 5 ICUs: a medical ICU, a surgical ICU (for patients who underwent abdominal and orthopedic surgery), an emergency ICU (for patients who presented at the emergency room), a pediatric ICU (for patients <15 yr old), and a cardio-pulmonary ICU (for patients who underwent thoracic surgery). We studied patients who were admitted to the MICU. The MICU has 22 beds and admits medical and neurological patients. All patients in the MICU were ≥15 yr old. The duration of the study was 6 yr and 7 months (1 January 2000 to 31 July 2006).
Definitions
Nosocomial candidemia was defined as one or more blood cultures positive for Candida species at least 48 hr after admission. Blood cultures were tested routinely if a patient's temperature was greater than 38℃. The onset of candidemia was defined as the date on which the first positive blood culture was detected. In-hospital mortality was defined as death during the same period of hospitalization.
Hemodynamic instability was defined as systolic blood pressure (BP) <90 mmHg, diastolic BP <60 mmHg, mean arterial BP <70 mmHg, or administration of a vasopressor on admission to the ICU. Patients were considered as having neutropenia if their absolute neutrophil count was <500 cells/mm3 on admission to the ICU. Acute renal failure was defined as a 0.5 mg/dL increase in serum creatinine level on admission to the ICU. Hepatic failure was defined as aspartate aminotransferase (AST) level >200 IU/L, alanine aminotransferase (ALT) level >200 IU/L, albumin level <3.0 g/dL, and prothrombin INR >2.0 on admission to the ICU. Central venous catheters (including internal jugular venous catheters, Hickman catheters, Swan-Ganz catheters, or femoral catheters), nasogastric tubes, and Foley catheters were considered risk factors for candidemia if they were used for more than 3 days before the onset of candidemia. Previous total parenteral nutrition (TPN), transfusion with any blood product, including red blood cells, platelets and fresh, frozen plasma, gastrointestinal (GI) bleeding, and steroid therapy were regarded as risk factors for candidemia when they occurred within 2 weeks of the onset of candidemia (15). Steroid therapy was defined as administration of ≥10 mg/day of prednisolone (or the equivalent dose of an alternative corticosteroid) or administration of <10 mg/day of prednisolone or its equivalent for more than 7 days. The use of immunosuppressive agents was defined as the administration of chemotherapeutic or antirheumatic agents within 2 weeks of the onset of candidemia (15). An immunocompromised state was defined as the presence of a malignancy or the use of immunosuppressive agents during the same admission. Candida colonization was defined as a Candida species-positive culture of a sputum, urine, or fecal sample collected at any time before the onset of candidemia.
Matching procedure
Control patients were selected from patients who did not have candidemia and were admitted to the MICU at about the same time as the candidemia patients. Control patients had no evidence of bacterial or fungal growth in blood cultures at any time during their hospitalization in the MICU. Control patients were selected according to the following matching criteria: sex, age (±5 yr), and an Acute Physiology and Chronic Health Evaluation (APACHE) II score (16) of at least 5 on the day of admission to the MICU.
Statistical analysis
Continuous variables are expressed as the mean±standard deviation or as the median and interquartile range. Patient characteristics were compared between groups using the Mann-Whitney test for continuous variables and the chi-square test for categorical variables. To identify risk factors independently associated with candidemia, variables that were significant according to a univariate analysis were subjected to binary logistic regression analysis. A P value <0.05 was considered significant. Kaplan-Meier survival curves were compared using the log-rank test. All statistical analyses were performed using SPSS software, version 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Analysis of patients with candidemia
During the study period, 52 of 5,383 MICU admissions were identified as having fungemia. Three patients were infected with species other than Candida (1 patient was positive for Aspergillus species and 2 patients were positive for Trichosporon beigelli). Therefore, we analyzed data from 49 patients.
The incidence of candidemia in the MICU was 9.1 per 1,000 admissions. The mean age of the patients was 57.6±14.1 yr. There were more men than women in the sample (28:21). Among the candidemia patients, there was no significant difference in APACHE II score between the day of admission to the ICU and the day of onset of candidemia (23.8±7.7 vs. 23.3±6.4, respectively; P=0.473).
Albicans was the predominant Candida species (32 cases, 65%); non-albicans Candida species accounted for 35% of infections (13 patients [27%] were infected with C. tropicalis, 3 patients [6%] were infected with C. parapsilosis, and 1 patient [2%] was infected with C. glabrata). Thirty-five patients (71%) were treated with an antifungal agent: amphotericin B was administered to 25 patients and fluconazole was administered to 10 patients. Eight of the 35 patients were treated with an antifungal agent before candidemia was diagnosed. The median duration of antifungal treatment was 11 days (range, 1-45 days). Bacteremia was present before diagnosis of candidemia in 20 patients (41%). Various causative organisms of bacteremia were detected: Clostridium perfringens, Escherichia coli, Enterobacter cloacae, Enterococcus faecium, Klebsiella pneumoniae, Staphylococcus aureus, Pseudomonas aeruginosa, and Staphylococcus epidermidis. The median duration of antibiotic use before the onset of candidemia was 16 days (range, 1-92 days). All patients were treated with antibiotics before the onset of candidemia.
Comparison of candidemia patients with matched control patients
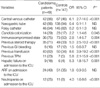
There were no significant differences in demographic characteristics or underlying diseases between the candidemia patients and the controls, except for the presence of malignancy (Table 1). Malignancy was more prevalent in patients with candidemia than in the control patients (P=0.048). This difference was not associated with solid malignancies (12 candidemia patients [25%] vs. 35 control patients [24%]; P=0.923) but with hematological malignancies (18 candidemia patients [37%] vs. 31 control patients [21%]; P=0.028). The dialysis method used for patients with chronic renal failure did not differ between the 2 groups. Patients with candidemia had longer stays in hospital and in the MICU compared with the control group, but there was no difference in their pre-ICU hospital stays (Table 1). Patients with candidemia were mechanically ventilated for a longer period during their total MICU stay than the controls (P=0.001) and had a longer MICU stay than the controls (P=0.001). At the time of MICU admission, patients with candidemia were more hemodynamically unstable than the controls (P<0.001).
Univariate analysis identified 8 variables that differed significantly between the candidemia patients and the controls (Table 2). These were central venous catheterization, candida colonization, an immunocompromised state, previous steroid therapy, transfusion, TPN, hepatic failure, and neutropenia on MICU admission. Multivariate analysis of these 8 variables using logistic regression revealed that central venous catheterization, previous steroid therapy, transfusion during the same admission, and hepatic failure on MICU admission were independent risk factors for candidemia (Table 3).
In-hospital mortality was 96% (47 of 49 patients) for patients with candidemia and 52% (77 of 147 patients) for control patients with odds ratio (OR) 21.4 (95% confidence interval [CI] 5.0-91.2). The significance of this difference in mortality rate was confirmed using Kaplan-Meier survival curves (P=0.024; Fig. 1).
DISCUSSION
We performed a 1:3 matched case-control study to determine the incidence of candidemia in MICU patients and the mortality rate among these patients and to identify factors associated with candidemia. We matched cases and controls on admission using variables known to be strongly correlated with nosocomial infections and the risk of death (e.g., severe illness and age). There were no differences between cases and controls in underlying illnesses, except for malignancy. The duration of the pre-ICU hospital stay did not differ significantly between groups.
In our study, the incidence of candidemia (9.1 patients per 1,000 admissions) and the crude mortality rate (96%) of candidemia patients were greater than those of previous studies, in which the incidence of candidemia was 0.3-2.5 episodes per 1,000 admissions (4, 7, 12, 17) and the crude mortality rate was 31-61% (4-9). Lee et al. (18) reported that the incidence of candidemia in a Korean ICU was 0.3-1.5 episodes per 1,000 patient days and that the crude mortality was 48.3%. This discrepancy may have arisen because we included patients with severe disease and only enrolled MICU patients with a preexisting risk factor for candidemia. Our study involved more patients with malignancy (61%) than previous studies (10-41%) (4, 5, 9, 18), which may also have contributed to the relatively high incidence of candidemia in our study.
Attributable mortality in our study was 44% (96% minus 52%), which is similar to the results of previous studies (34-49%). However, crude mortality was higher in our study than in previous studies (96% vs. 40-61%, respectively) (5, 9, 12, 18, 19). Of 8 patients who received preemptive antifungal therapy, only 1 survived. There are several potential explanations for the difference in crude mortality between our study and previous studies. First, criteria for enrollment in our study were stricter than those of other studies, which enrolled general ward patients whose mortality rate was lower than that of our patients (5, 9, 19). According to previous studies, an APACHE II score >20 during candidemia is associated with an elevated mortality rate (12) irrespective of intensive antifungal therapy (15). For this reason, we conducted an APACHE II score-matched case-control study. This matching procedure ensures that the control group is valid for comparison of mortality rate. Second, our study included more patients with malignancy (61%) than previous studies (10-41%) (4, 5, 9, 18). These factors may have been responsible for the high mortality rate in our study.
The Kaplan-Meier survival analysis showed that the difference in mortality between the two groups was sustained (P=0.024). In terms of underlying illness, the candidemia patients had more malignancies than the control patients (P=0.048). Therefore, it could be inferred that the difference in the prevalence of malignancy contributed to the difference in mortality. However, survival analysis that excluded patients with a hematological malignancy showed a consistent result (P=0.037 according to the log-rank test).
Many studies have been undertaken to evaluate risk factors for the development of candidemia. However, most studies were undertaken using specific patient populations or did not use case-control methodology (4, 10). Using a case-control design, we identified several independent risk factors for candidemia in the MICU: central venous catheterization, previous steroid therapy, and previous transfusion. This result is consistent with risk factors identified by other authors (5, 13, 20, 21).
We identified a new risk factor, viz., the presence of hepatic failure on admission to the MICU. A previous study reported that fungal infection (predominantly candidiasis) is a common complication (32%) in patients with acute liver failure (22). However, there are few reports on hepatic failure as an independent risk factor for candidemia. In our study, 9 patients in the candidemia group had hepatic failure on admission to the MICU. Using multivariate analysis, we identified hepatic failure on admission to the MICU as an independent risk factor for candidemia (OR, 7.6 ; 95% CI, 1.5-39.0). Hepatic failure may be a risk factor because patients with hepatic failure have increased susceptibility to infection because of abnormal immune function (23), increased colonization of the small bowel (24, 25), impaired phagocytic function (26, 27), or reduced complement levels (28).
Our study has several limitations. First, the incidence of candidemia in the MICU might have been underestimated. Because this was a retrospective study, no special fungal blood cultures were performed. In our hospital, blood is cultured for 5 days using a Bact/Alert 3D instrument (BioMerieux, Inc., Durham, NC, USA) when a routine blood culture is requested. If no growth is identified after 5 days, the blood culture is terminated. However, if a fungal blood culture is requested, the blood is cultured for 3 weeks to identify any slow-growing Candida species. Several authors have reported that they cultured blood for more than 5 days to identify specific slowgrowing organisms. Therefore, it has been suggested that the appropriate duration for blood culture should be determined on an individual basis according to the clinical relevance of the culture (29, 30). A prospective study would have avoided this methodological weakness.
Second, the control patients had no evidence of bacterial or fungal growth in their blood cultures. However, systemic bacterial or fungal infections may be present even if blood cultures are negative. In this study, 67 patients (46%) in the control group used empirical antibiotics. Therefore, the control group may have included infected patients. However, circumvention of this situation is clinically very difficult. Therefore, we performed a multivariate analysis that included antibiotic use as a variable.
In conclusion, bloodstream Candida infections in MICUs are associated with much higher crude mortality rates than would be expected for uninfected patients with the same disease severity. We identify an additional independent risk factor for candidemia, the presence of hepatic failure on MICU admission. Therefore, increased awareness of risk factors, including hepatic failure, is necessary for the management of candidemia.



 XML Download
XML Download