

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neonatal respiratory distress syndrome (RDS) is a progressive respiratory failure that is caused primarily by a deficiency of pulmonary surfactants (PS). In 1959, Avery and Mead (1) showed that PS deficiency is a major factor in the pathophysiology of RDS. The first successful treatment was reported in 1980, when Fujiwara et al. (2) successfully administered exogenous PS to preterm infants with RDS. PS replacement therapy is now the routine method of treatment for infants with RDS, and since its introduction, morbidity and mortality due to RDS in preterm infants has decreased remarkably.
In Korea, Surfacten® (Mitsubishi Tanabe Pharma Corporation, Tokyo, Japan), the first artificial PS, was available in 1991. Thereafter, Exosurf® (Burroughs Wellcome Co., Research Triangle Park, NC, U.S.A.) was available from 1991 to 1997, Newfactan® (Yuhan Pharm Corporation, Seoul, Korea) from 1996, and Curosurf® (Chiesi Farmaceutici, Parma, Italy) from 2003 (Table 1).
In Korea, PS was first used to treat 8 RDS cases in 1990 by Namgung et al. (3), and this was followed by a report on 6 cases by Park et al. (4) in 1991. Subsequently, Bae et al. (5) reported PS therapy outcomes in neonatal RDS on a national basis for 1990 and 1991. Bae et al. published again a report on the clinical outcomes of PS therapy in Korea in 1996 and 2002, respectively (6, 7).
In the present study, we investigated improvements of clinical outcome achieved by PS therapy for the treatment of RDS on national data basis for the year of 2007 and compared these findings with those of the three previous reports.
MATERIALS AND METHODS
Subjects
In March 2008, we sent 57 hospitals in Korea questionnaires that addressed the clinical outcomes of PS replacement therapy in 2007. Details of the 57 participating hospitals and the individuals that participated in this study are included in the list of contributors.
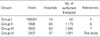
Patients treated in the individual report periods are referred to as groups for convenience, as follows. 1) Group I-patients enrolled in a 1990 to 1991 (24 months) national survey conducted by Bae et al. (5); 2) Group II-patients enrolled in a national survey performed in 1996 (12 months) by Bae et al. (6); 3) Group III-patients enrolled in a national survey performed in 2002 (12 months) by Bae and Kim (7); and 4) Group IV-patients enrolled in a national survey performed in 2007 (12 months). Approval to use previous data (5-7) was obtained from each publisher of the journals.
Details of the four study groups, numbers of cases, and the hospitals that participated in this survey are shown in Table 2. In Group I, there were 60 patients at 16 hospitals for the year of 1990 and 1991. For Group II, 1,179 cases were recruited nationally at 64 hospitals for 1996, and for Group III, 1,595 cases were recruited nationally at 62 hospitals for 2002. Finally, for Group IV, 1,921 cases were recruited from 57 hospitals for 2007.
In terms of all RDS births, the proportions of patients who received PS therapy are shown in Table 3 subdivided into in-hospital-born and out-hospital-born patients. For all RDS patients, the percentages that underwent PS replacement therapy increased from 47.3% and 66.2%, in Groups II and III to 77.7%, in Group IV.
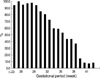
Fig. 1 summarizes the proportions of RDS patients in Group IV that underwent PS replacement therapy by birth weight and gestational period.
Exogenous PS preparations used for therapy
In Group I, Surfacten® (Japan) was the only available agent in Korea, and was used in all cases. Subsequently, several PS preparations were used, as follows; Surfacten® (70.5%) or Exosurf® (26.3%) in Group II; Surfacten® (35.4%), Newfactan® (64.1%), or a mixture (0.5%) in Group III; and Surfacten® (51.3%), Newfactan® (39.3%), Curosurf® (8.3%), or a mixture (1.1%) in Group IV (Fig. 2).
Classifications for clinical interpretation
Initial chest radiograph findings before PS replacement therapy were classified as Stage I, II, III, or IV using Bomsel's classification (8). The classification of Fujiwara et al. (9) uses ventilatory index as a respiratory index. Ventilatory index is calculated using FiO2×mean airway pressure (MAP)/arterial oxygen pressure (PaO2). Using ventilatory index values, respiratory distress was classified into 3 groups in the present study, namely, mild respiratory distress <0.047; moderate respiratory distress ≥0.047 and <0.133; and severe respiratory distress ≥0.133.
We classified the early response to PS therapy using the classification of Fujiwara et al. (10), which utilizes fraction of inspired oxygen (FiO2), MAP, and arterial-alveolar oxygen tension ratio (a/A PO2). Patients were classified into good response, relapse, and poor response groups. The good response group was composed of patients that showed clinical improvements in FiO2, MAP, and a/A PO2 after PS administration. The relapse group was composed of patients that experienced a recurrence of respiratory distress after an initial good response, as determined using respiratory markers. Poor response group members showed no respiratory marker improvement and continued respiratory distress.
RESULTS
Epidemiology
The incidences of in-hospital-born RDS by birth weight and gestational period in Group IV are shown in Fig. 3. This data shows that RDS incidence increased with decreasing birth weight and gestational period.
The proportions of patients in Group IV who received PS replacement therapy among all RDS births by gestational period are illustrated in Fig. 4. The data show that the need for PS replacement therapy increased with decreasing gestational period. Interestingly, PS replacement therapy was less used in patients with a birth weight of <500 g, presumably due to the abandonment of rescue therapy due to a perceived low likelihood of survival.
The distributions of birth weights and gestational periods among RDS patients in Group IV who received PS therapy are shown in Fig. 5. PS therapy was performed in 87.9% of low birth weight infants (<2,500 g) with RDS, in 56.7% of very low birth weight infants (<1,500 g), and in 27.5% of extremely low birth weight infants (<1,000 g).
Fig. 5 shows the distribution of RDS patients in Group IV who received PS replacement therapy by gestational period. In the Group III study, PS replacement therapy was conducted in 93.5% of preterm patients with RDS (gestational period <37 weeks), 6.4% of term patients with RDS (gestational period 37-42 weeks), and in no post-term patient with RDS (gestational period ≥42 weeks). When preterm patients were sub-grouped by gestational period, 20.5% of the gestational period 33-36 weeks subgroup underwent PS replacement therapy, 36.4% of the gestational period 29-32 weeks subgroup, and 36.4% of the gestational period <28 weeks subgroup.
Clinical findings
In the surfactant treated RDS patients in Group IV, initial chest radiograph findings (before PS therapy) showed that 11.3%, 25.3%, 36.9%, and 26.0% of patients were of Stages I, II, III, and IV, respectively, according to Bomsel's classification. In Groups III and IV the rates of those with relatively severe RDS (Stage III and IV) were high at 67.7% and 62.9%, respectively (Fig. 6).
Distributions of severity according to ventilatory index in each Group before PS replacement therapy are shown in Fig. 7. In Group IV, 23.0%, 42.0%, and 35.0%, of patients had mild, moderate, or severe respiratory distress, respectively.
In Groups I and II, all cases received a single dose of PS, probably because repeated administrations were limited by medical insurance policies at that time. However, because repeated PS administration was approved in part prior to 2002, in Groups III and IV second and third administrations were reported in some cases. Single and multiple uses were reported in 79.9% and 20.1% of cases in Group III, and these were similar to those reported in Group IV (80.5% and 19.5%, respectively). Summarizing, multiple PS was used in about 20% of all RDS patients in Groups III and IV (Table 4).
In terms of early response to PS therapy, using the Fujiwara et al. classification, i.e., good response, relapse, and poor response, responses in Group IV were 69.2%, 14.4%, and 16.4%, respectively. Response results for Groups I, II, III, and IV are shown in Fig. 8.
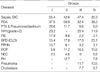
Complications frequently developed during the management of RDS patients and preterm babies (Table 5). The occurrence rates of infections (including disseminated intravascular coagulopathy [DIC]) were high in Groups I, II, and III at 55.4%, 42.6%, and 47.4%, but the rate was appreciably lower in Group IV (25.3%). These changes were accompanied by decreases in pneumothorax and intraventricular hemorrhage. Furthermore, the frequencies of bronchopulmonary dysplasia (BPD) and retinopathy of prematurity (ROP) were found to be higher in Group IV, in parallel with the improved survival of extremely premature infants in 2007.
Mortality
As shown in Fig. 9, mortality rates (defined as the percentage of neonates who died within 28 days of birth) dramatically decreased over the study period (40% in Group I, 30% in Group II, 18.7% in Group III, and 14.3% in Group IV).
Mortality rates of surfactant treated patients by birth weight and gestational period in Group IV are illustrated in Fig. 10. In term babies, mortality rates were found to be high, which appears to be due to some co-morbidities other than RDS causing respiratory distress such as, persistent pulmonary hypertension, meconium aspiration, sepsis, and so on, which also influence negatively the function of surfactant. Many of co-morbidities are known to bring their clinical courses severe enough even leading to death.
As shown in Fig. 11, in Groups III and IV, mortality rates of those who underwent PS once were 15.6% and 13.0%, respectively. These rates were lower than mortalities among those who underwent repeated treatment (24.1% in Group III and 16% in Group IV), probably because more severe cases were administered multiple PS.
DISCUSSION
In 1980, Fujiwara et al. (2) first successfully administered exogenous PS to preterm infants with RDS, and subsequently several PS preparations were developed. These preparations have since been shown to reduce mortality and morbidity effectively among RDS patients by several double blind, randomized, controlled studies. Today PS replacement therapy has become a routine method of treating infants with RDS.
The PS preparations used today are either animal-sourced or synthesized. Animal-sourced agents, include; 1) Alveofact® (Bovactant, Germany), BLES® (Canada), Infasurf® (Calfactant, U.S.A.), Survanta® (Beractant, U.S.A.), Surfacten® (Surfactant-TA, Japan), and Newfactan® (Korea), which are all extracted from bovine lungs, and 2) Curosurf® (Poractant alfa, Italy) from porcine lungs. Synthetic agents include; ALEC® (Pulmactant, U.K., no longer manufactured), Exosurf® (Colfosceril palmitate, U.S.A.); phospholipid synthetics, and Surfaxin® (Lucinactant, U.S.A., not FDA licensed), a surfactant protein B synthetic (11). Of these, Surfacten®, Newfactan®, and Curosurf® are currently being used, but Exosurf®, which was used for short time, is no longer available in Korea. The PS agents used in Korea are listed in Table 1.
Surfacten® and Newfactan® contain phospholipids extracted from bovine lung, and surfactant proteins -B and -C, which increase surface physical activity and reduce surface tension on the alveolar surface. Curosurf® is produced from porcine lung by chloroform/methanol extraction and liquid gel electrophoresis for purification, and contains surfactant proteins -B and -C. In Group IV, Surfacten® (51.3%) was administered in more than half cases, and Newfactan® (39.3%), Curosurf® (8.3%), and mixtures of these agents (1.1%) were followed. Several meta-analyses concluded that PS replacement therapy reduces mortality in RDS patients. In 1993, Jobe et al. (12) after integrating results from 1985 to 1992, reported that mortality is decreased by PS therapy when used as a prophylactic or rescue therapy with an odds ratio of 0.6. Furthermore, in 1993 Ptamanik et al. (13) reported that PS agents of synthetic or animal origin administered as prophylactic or rescue therapies effectively reduce mortality among RDS patients (odds ratio 0.5-0.6). In a meta-analysis conducted by the Committee on Fetus and Newborn of the American Academy of Pediatrics (2008) (14), attributed remarkable reductions in the mortalities of RDS patients to these agents (odds ratio of 0.6 for agents of animal origin and of 0.7 for those of synthetic origin when administered with prophylactic intent; and of 0.67 for agents of animal origin PS and 0.73 for those of synthetic origin when administered as rescue therapies).
The use of PS therapy obviously decreased mortality among Korean RDS patients over the 17-yr study period, i.e., from 40.0%, 30.0%, 18.7%, and 14.3% for the periods 1990/91, 1996, 2002, and 2007, respectively. Furthermore, PS therapy reduced mortalities not only among RDS patients, but also among prematurities and neonates in Korea. In the pre-PS era (before 1990), mortality due to RDS was much higher. In addition, several advances in neonatal supportive care, such as, improvements in artificial ventilator strategies, and the prevention and early management of infections and complications, have also undoubtedly contributed to these reductions in mortality (15-17).
A double blind, randomized, controlled study on Surfacten® conducted in Japan found lower mortality among RDS patients (8%, birth weight<1,750 g) than we found in the present study (9). On the other hand, other double blind, randomized, controlled study performed on Survanta®, which has the same composition as Surfacten®, reported a RDS mortality of 18.4% (birth weight <1,750 g) (18).
In the present study, we investigated the frequency of RDS among in-hospital-born patients in 2007 treated at 57 hospitals and found that the frequency of RDS decreases as birth weight is light or gestational period is short.
Furthermore, in the present study, PS was administered to a greater proportion of RDS patients with time, i.e., 47.3%, 66.2%, and 77.7% in Groups II, III, and IV, respectively. This appears to be due to changed attitude of the Korean Medical Insurance Association in terms of PS administration. In terms of our 2007 data, rates of PS use were found to be greater in patients with a smaller gestational period, which implies that RDS is more severe among these patients. Furthermore, PS replacement therapy was used in 87.9% of low birth weight infants (<2,500 g) and in 56.7% of very low birth weight infants (<1,500 g) in terms of birth weight, and in 93.5% of preterm infants in terms of gestational period (especially 73% had a gestational period of <32 weeks). In brief, infants with a gestational period of <32 weeks and a birth weight of <1,500 g were major members.
In terms of the classification of initial chest radiographic findings in RDS patients, stage distributions were similar for Groups III and IV. The proportions of patients with stage III or IV (severely affected) composed about 2/3 of Groups III and IV, which confirms that patients with more severe initial chest findings by radiography require more PS therapy.
Initial respiratory distress classifications using ventilatory index showed that patients who received PS therapy in Groups I and II had milder conditions than those in Groups III and IV, which appears to be due to the extended indication for PS referred to above. Groups III and IV had similar initial respiratory distress distributions. In Group IV, 23.0% had mild respiratory distress, 42.0% had moderate, and 35.0% had severe respiratory distress. Furthermore, those with moderate or severe respiratory distress constituted as much as 77% of Group IV RDS patients, and thus, more aggressive management is required in these patients.
Korean medical insurance policies did not permit multiple administration of PS in 1990/91 (Group I) or in 1996 (Group II), when only a single dose was administered in all cases. However, the policy was changed to a direction permitting multiple dose in 2001. In Groups III and IV multiple administrations were performed in roughly 1/4 of cases. In Groups III and IV 14.4% and 16.0% of patients relapsed and these patients were treated with multiple doses of PS.
The classification of early response to the PS treatment showed better results in Groups III and IV than in Groups I and II. In Group IV, 69.2% responded well, 14.4% relapsed, and 16.4% responded poorly, which means that about 1/5th of RDS patients relapsed after initial PS treatment. In a Japanese report (10), 79% responded well, 16% relapsed, and 5% responded poorly, which is a substantially better response rate that observed in our 2007 study.
To improve the prognosis of RDS patients early detection and adequate management of co-morbidities, including associated diseases and complications, are as important as general supportive care. We examined data for the past 17 yr in terms of complications and associated diseases that developed during the management of RDS patients and preterm babies (Table 5).
Mortalities of RDS neonates in Korea were found to dramatically improve over the 17-yr study period, i.e., from 40.0%, 30.0%, 18.7%, to 14.3% for 1990/91, 1996, 2002, and 2007, respectively. Furthermore, our study of birth weights and gestational periods showed that both are inversely related to mortality, which means that these high-risk patients require more attention.
In this longitudinal study, we analyzed clinical findings, disease severity, dose schedule of PS administration, response to treatment, associated diseases, complications, and mortalities, with respect to RDS and PS treatment in neonates over a 17-yr period in Korea. We conclude that surfactant treatments in neonates with RDS have had a marked impact on clinical course and outcome, together with substantial reduction of mortality rates among RDS patients over the last 17 yr in Korea.
LIST OF CONTRIBUTORS
We list the following 57 hospitals and individuals who participated in this research by providing information in this nationwide study; Byeong Il Kim (Seoul National University Bundang Hospital), Chang Ryul Kim (Hanyang University Guri Hospital), Chan Hoo Park (Gyeongsang National University Hospital), Chong Woo Bae (Kyunghee University East-West Neo Medical Center), Chung Sik Chun (The Catholic University of Korea Kangnam St. Mary's Hospital), Eun Ae Park (Ewha Womans University Mokdong Hospital), Eun Sil Lee (Yeungnam University Medical Center), Han Suk Kim (Seoul National University Children's Hospital), Heng Mi Kim (Kyungpook National University Hospital), Hye Sun Yoon (Eulji General Hospital), Hyun Kyung Park (Hanyang University Medical Center), Hyun Seung Jin (Gangneung Asan Hospital), Hyun Seung Lee (The Catholic University of Korea Uijeongbu St. Mary's Hospital), Il Sung Park (Soonchunhyang University Gumi Hospital), Il Tae Hwang (Hallym University Kangdong Sacred Heart Hospital), In Kyung Sung (The Catholic University of Korea St. Mary's Hospital), Jang Hoon Lee (Korea University Anam Hospital), Jang Hoon Lee (Korea University Ansan Hospital), Jong Hee Hwang (Inje University Ilsan Paik Hospital), Jung Are Kim (Hanil General Hospital), Jung Hyun Lee (The Catholic University of Korea St. Vincent's Hospital), Jung Ju Lee (Chung-Ang University Medical Center), Ki Soo Kim (University of Ulsan Asan Medical Center), Kyu Hyung Lee (Pochon Jungmun University Cha Hospital), Kyung Hee Lee (Gumi CHA General Hospital), Kyung Og Ko (Konyang University Hospital), Kyun Woo Lee (Dae Dong Hospital), Mea Young Chang (Chungnam National University Hospital), Mi Jung Kim (Chungbuk University Hospital), Mi Lim Koo (Sowha Children's Hospital), Min Soo Park (Yonsei University Yongdong Severance Hospital), Moon Sung Park (Ajou University Hospital), Myoung Jae Chey (Inje University Sanggye Paik Hospital), Myung Ho Oh (Soonchunhyang University Cheonan Hospital), Ran Namgung (Yonsei University Severance Children's Hospital), Sang Geel Lee (Daegu Fatima Hospital), Sang Kee Park (Chosun University Hospital), Sang Lak Lee (Keimyung University Dongsan Medical Center), Sang Young Bae (Halla General Hospital), Son Moon Shin (Cheil General Hospital & Women's Health Care Center), Soo Chul Cho (Chonbuk National University Hospital), So Young Kim (The Catholic University of Korea Holy Family Hospital), Su Eun Park (Pusan National University Hospital), Sung Mi Kim (Busan St. Mary's Medical Center), Sung Min Choi (Dongguk University Gyongju Hospital), Sung Shin Kim (Soonchunhyang University Bucheon Hospital), Sun Ju Lee (Dongguk University Pohang Hospital), Tae Jung Sung (Hallym University Kangnam Sacred Heart Hospital), Won Ho Hahn (Kyunghee University Kyunghee Medical Center), Woo Taek Kim (Daegu Catholic University Medical Center), Yeun Kyun Oh (Wonkwang University Hospital), Yong Hoon Jun (Inha University Hospital), Yong Won Park (College of Medicine Inje University Seoul Paik Hospital), Young Hee Kim (Bundang Jaesang General Hospital), Young Sook Hong (Korea University Guro Hospital), Young Youn Choi (Chonnam National University Hospital), and Youn Woo Kim (Cheju National University Hospital).













 XML Download
XML Download