

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Maternal chorioamnionitis has been known to result in a lung maturation response. The incidence of respiratory distress syndrome in preterm infants decreased when they were exposed to maternal chorioamnionitis (1). In animal study, maternal chorioamnionitis increased the size of surfactant pool and the volume of potential gas space (2). However, maternal chorioamnionitis has also been associated with abnormal lung development. The exposure to maternal chorioamnionitis increased the incidence of bronchopulmonary dysplasia (BPD) in preterm infants (1, 3), and resulted in alveolar simplification and impaired microvascular development (4, 5), which are histologic hallmarks of new BPD in the post-surfactant era (6).
Transforming growth factor-beta (TGF-β) is an important regulator of cellular proliferation and differentiation. It has been considered to be crucial for the normal lung development and implicated in the development of BPD. During branching morphogenesis in the lung development, the expression of TGF-β was reduced (7, 8). Overexpression of TGF-β inhibited airway branching (8, 9), while inhibition of TGF-β enhanced airway branching in vitro (9-11). Compared to branching morphogenesis, neither the role nor the status of expression of TGF-β during alveolarization is well known. Several researchers reported that overexpression of TGF-β1 inhibited alveolarization in neonatal rat (12, 13), and inhibition of TGF-β resulted in an emphysematous change in adult mouse (14, 15). However, the role of TGF-β in normal lung development, especially during alveolarization in human preterm infants, remains unclear.
TGF-β is also known as an important mediator of fibrosis. Kotecha et al. reported an increased level of TGF-β1 in bronchoalveolar lavage (BAL) fluid of preterm infants who developed BPD later (16). In animal model, enhanced endogenous production or overexpression of TGF-β1 resulted in pulmonary pathologic changes seen in human BPD, which are enlarged alveolar sacs, poor secondary septation, thick and hypercellular septa, and abnormal capillary development (12, 13, 17). However, the role of TGF-β in the injury response of the lungs in preterm infants also remains unclear.
The objective of our study was to examine the effect of maternal chorioamnionitis on the expression of TGF-β1, the isoform most implicated in fibrosis among its three isoforms whose biological properties are nearly identical, and compare the extent of TGF-β1 expression between preterm infants who develop BPD later and who do not.
MATERIALS AND METHODS
Study design
A prospective cohort study was done to examine the effect of maternal chorioamnionitis on the expression of TGF-β1 in BAL cells of preterm infants. The cohort consisted of preterm (gestational age <34 weeks) infants who were admitted to neonatal intensive care unit (NICU) at Seoul National University Children's Hospital and Seoul National University Bundang Hospital (after May 2003) between March 1999 and February 2004 and who met the following criteria: 1) endotracheal intubation at delivery room, and 2) absence of major congenital anomalies. During the study period, a total of 79 preterm infants were enrolled. Among these preterm infants, 7 infants whose parents' consent was not obtained and 9 infants to whom BAL was not done or done after the first 24 hr after birth due to death or clinical instability were excluded from the analysis. Finally 63 preterm infants were analyzed. Of these, 8 preterm infants died before 36 weeks postmenstrual age when the assessment for the development of BPD was made. The institutional review board at Seoul National University Hospital approved the study protocol (H-0603-230-172), and informed consent was obtained from a parent before enrollment.
Bronchoalveolar lavage
Endotracheal intubation in the delivery room was done only when clinically indicated according to the neonatal resuscitation program (18). BAL fluid and cells were obtained by the method described by Kotecha (19) shortly after birth as soon as the preterm infants became stable, but before surfactant replacement therapy when indicated. Briefly, with the baby supine, two aliquots of sterile saline solution, 1 mL/kg (maximum 2 mL), were instilled via endotracheal tube, and then immediately sucked back, and the returned BAL fluid was collected in a suction trap. BAL fluid was centrifuged for 10 min at 1,000 g within 10 min after acquisition. The supernatant and sediment, which is a cell fraction, were contained to separate polypropylene tubes, and stored at -70℃ and -160℃ in liquid nitrogen, respectively. The stored supernatant and sediment were used for the measurement of TGF-β1 concentration and TGF-β1 mRNA reverse transcription polymerase chain reaction (RT-PCR), respectively.
Determination of TGF-β1 and TGF-β1 mRNA in BAL fluid and cells
The TGF-β1 concentration in BAL fluid was measured using a commercially available ELISA kit (Quantikine® human TGF-β1 immunoassay, R&D Systems Inc., Minneapolis, MN, U.S.A.). The sensitivity of the test was <7 pg/mL. Interassay and intra-assay coefficients of variation were 7.3% and 11.7%, respectively. The frozen BAL fluid sediment in liquid nitrogen was pulverized and homogenized using Qiashredder® (Quiagen Inc., Valencia, CA, U.S.A.). The extraction of mRNA from the homogenates was done using Oligotex® direct mRNA kit (Quiagen Inc.). Reverse transcription of TGF-β1 mRNA was done using MuLV reverse transcriptase (PerkinElmer Inc., Waltham, MA, U.S.A.) and RNA PCR kit® (PerkinElmer Inc.). The sense and antisence primers for human TGF-β1 cDNA were designed by PrimerSelect® version 3.11 (DNAStar Inc., Madison, WI, U.S.A.). The primer for forward reaction was 5'GCCCTGGATACCAACTATTGCT3', and the primer for reverse reaction was 5'AGGCTCCAAATATAGGGGCAGG3'. PCR was done using automatic PCR cycler (Gene Cycler®, Bio-Rad Laboratories, Hercules, CA, U.S.A.). The size of the PCR product was 161 bp. For internal standard, PCR was also done for β-actin. PCR products were loaded and analyzed on 1% agarose gel with a 10-fold diluted 100 bp DNA ladder (Promega Corp. Madison, WI, U.S.A.) as a DNA marker. Image analysis was performed using 'Band leader' software version 2.01. The signal intensity of TGF-β1 mRNA was expressed relative to that of β-actin.
Definition of maternal chorioamnionitis and bronchopulmonary dysplasia
Maternal chorioamnionitis was defined histologically as ≥grade 2 inflammation of the amnion or choriodecidua or ≥grade 1 necrotizing funisitis according to the grading system suggested by Salafia et al. (20). BPD was defined as a state of chronic oxygen requirement at 36 weeks postmenstrual age plus a total oxygen duration of ≥28 day with a consistent chest radiographic finding, which is persistent hazy opacification or a cyst-like pattern of density and lucency.
Statistical analysis
Statistical analysis was done using SPSS version 11.5 (SPSS Inc., Chicago, IL, U.S.A.). Comparison of means between groups was performed using one-way analysis of variance (ANOVA) test or Mann-Whitney U-test. Comparison of frequencies between groups was done using χ2 or Fisher's exact test. To investigate the relationship between TGF-β1 or TGF-β1 mRNA in BAL fluid and cells and maternal chorioamnionitis or BPD, while eliminating the effects of potential confounding variables, multivariate logistic regression analysis was performed. A p value of <0.05 was considered statistically
significant.
RESULTS
Clinical profiles of preterm infants with and without maternal chorioamnionitis
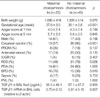
Gestational age and the rate of Cesarean section delivery were significantly lower in preterm infants with maternal chorioamnionitis. There were no significant differences in birth weight, Apgar scores at 1 and 5 min, sex ratio, premature rupture of membrane, antenatal steroid therapy, and intrauterine growth restriction. Respiratory distress syndrome (RDS) was significantly less prevalent, while BPD was more prevalent in preterm infants with maternal chorioamnionitis. There were no significant differences in echocardiography-documented patent ductus arteriosus, culture-proven sepsis, and periventricular leukomalacia (Table 1).
TGF-β1 and TGF-β1 mRNA in BAL fluid and cells in preterm infants with and without maternal chorioamnionitis
The concentrations of TGF-β1 in BAL fluid were lower in preterm infants with maternal chorioamnionitis, although statistically insignificant. Signal intensities of TGF-β1 mRNA expressed relative to that of β-actin were significantly lower in preterm infants with maternal chorioamnionitis (0.70±0.12 vs. 0.81±0.15, p=0.007) (Table 1).
Multivariate logistic regression analysis including confounders such as birth weight, gestational age and Cesarean section delivery in the logistic model revealed an independent relationship between TGF-β1 mRNA in BAL cells and maternal chorioamnionitis (adjusted odds ratio 1.8 per 0.1 decrease of signal intensity of TGF-β1 mRNA expressed relative to that of β-actin, 95% confidence interval 1.0-3.3) (Table 2).
The correlations between TGF-β1 mRNA in BAL cells and gestational age and birth weight
Signal intensity of TGF-β1 mRNA expressed relative to β-actin demonstrated a moderate positive correlation with gestational age (r=0.414, p=0.002) and birth weight (r=0.372, p=0.005). However, in preterm infants with maternal chorioamnionitis, there were no correlations between them. In preterm infants without maternal chorioamnionitis, there were also moderate correlations between signal intensity of TGF-β1 mRNA and birth weight and gestational age (Fig. 1).
There were no correlations between the concentration of TGF-β1 in BAL fluid and birth weight or gestational age (data not shown).
Clinical profiles of preterm infants who developed BPD and who did not
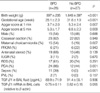
Birth weight, gestational age, and Apgar scores at 1 and 5 min were significantly lower in preterm infants who developed BPD later. Maternal chorioamnionitis, echocardiography-documented patent ductus arteriosus (PDA) and culture-proven sepsis were more prevalent in preterm infants who developed BPD later. The higher prevalence of sepsis in preterm infants who developed BPD later was thought to be consequential rather than causative of BPD considering the temporal relationship between them. There were no significant differences in sex ratio, the rate of Cesarean section delivery, premature rupture of membrane, antenatal steroid therapy, intrauterine growth restriction, RDS and periventricular leukomalacia (Table 3).
TGF-β1 and TGF-β1 mRNA in BAL fluid and cells and later development of BPD
The concentrations of TGF-β1 in BAL fluid did not differ significantly between preterm infants who developed BPD later and who did not (Table 3). Signal intensities of TGF-β1 mRNA expressed relative to β-actin in BAL cells were marginally significantly lower in preterm infants who developed BPD later (0.75±0.11 vs. 0.82±0.15, p=0.055) (Table 3).
Subsequent subgroup analyses by the presence of maternal chorioamnionitis and the development of BPD demonstrated no significant differences in the concentration of TGF-β1 in BAL fluid and signal intensities of TGF-β1 mRNA expressed relative to β-actin in BAL cells, except for preterm infants who did not develop BPD (Table 4). Multivariate logistic regression analysis including confounders such as gestational age, chorioamnionitis and PDA which were significant variables in the univariate analysis in the logistic model failed to reveal an independent relationship between TGF-β1 mRNA in BAL cells and the later development of BPD (Table 5).
DISCUSSION
Pulmonary fibrosis was a prominent feature in preterm infants who died of BPD (21, 22). Moreover, markers of fibrosis such as hydroxyproline, fibronectin, and desmosine were increased in lung tissue, tracheal fluid, and urine of preterm infants who developed BPD (23-25). TGF-β has been known to be an important mediator of fibrosis. Accordingly, TGF-β has been implicated in the pathogenesis of BPD. Kotecha et al. (16) demonstrated increased levels of TGF-β1 in BAL fluid in preterm infants who developed BPD later. However, as with the introduction of antenatal steroid, surfactant replacement therapy, and gentle ventilatory strategies, the incidence of classic BPD in which fibrosis is a predominant feature has decreased (26). Instead, a milder new type of BPD has been increasing in preterm infants who were not exposed to significant hyperoxia and baro/volutrauma (27). This type of BPD in the post-surfactant era has different pathologic characteristics from that of classic BPD. It lacks fibrosis, airway injury, and emphysema which are predominant features of classic BPD. Instead, an arrest in alveolar and microvascular development is the pathologic hallmark of this type of BPD in the post-surfactant era (6).
Recently, there has been growing evidence that antenatal inflammatory process may inhibit normal alveolarization (4, 5, 28). In epidemiologic and clinical studies, antenatal inflammation or maternal chorioamnionitis was related to the development of BPD (1, 29-31). However, there have been few studies as to the status of TGF-β expression in the lungs when the fetus is exposed to maternal chorioamnionitis. The exact role of TGF-β in normal alveolarization phase in human lung development is not known clearly, although its role in branching morphogenesis is well known in in-vitro studies (7-11). Considering that an increased TGF-β level has been associated with the development of BPD, it could be reasonably postulated that TGF-β would be increased in preterm infants with maternal chorioamnionitis which has also been related to the development of BPD. Recently, Kunzmann et al. (32), demonstrated elevated TGF-β1 mRNA and protein expression in the lungs by experimental maternal chorioamnionitis in preterm neonatal sheep model. In contrast, the expression of connective tissue growth factor, a down-stream mediator of some of the pro-fibrotic effects of TGF-β1, decreased. In our study, however, the expression of TGF-β1 mRNA and protein decreased in BAL cells and fluid obtained shortly after birth from the preterm infants who were exposed to maternal chorioamnionitis, although the latter lacked statistical significance. These results are opposing to those of Kunzmann et al. and also to common expectation. Some speculations may be done as to our unexpected results. Firstly, in our study, the profile of BAL cells was not analyzed. Therefore, decreased expression of TGF-β1 mRNA could be simply a reflection of different cell profiles. If the proportion of cell types in BAL fluid obtained from each preterm infant differed by the presence of airway inflammation or maturity, the interpretation of the measured value of a specific mRNA which is expressed differently by airway cell type would be problematic. In our study, there is a possibility that the proportion of three major cell types of BAL cell which are alveolar macrophages, neutrophils, and epithelial cells may be affected by maternal chorioamnionitis and gestational age. However, TGF-β1 is known to be markedly expressed in alveolar macrophages, and to a lesser degree, in neutrophils and epithelial cells (16). If it is the case, the validity of TGF-β1 mRNA value in BAL cells by RT-PCR method would be unaffected. Secondly, the method of BAL can matter. We used non-bronchoscopic BAL due to infeasibility of bronchoscopy for study preterm infants because of their small body size. Therefore, there may be a concern that the cells from distal airway and alveoli were not obtained sufficiently. However, Kotecha (33) reported that the cell profiles of non-bronchoscopic BAL cells from each lung were very similar, thus very representative of lung environment. Grigg et al. (34) also demonstrated that a sufficient amount of distal airway cells was obtained by non-bronchoscopic BAL. Therefore, decreased expression of TGF-β1 mRNA in non-bronchoscopic BAL cells in our study may be thought to be representative of actual alveolar environment. However, further studies that will analyze the cell profiles of BAL cells are required to eradicate the controversy on the representativeness of true alveolar environment of our data. Moreover, the lack of statistical significance of TGF-β1 in BAL fluid in comparison to that of its m-RNA expression in BAL cell was observed in our study. This disparity between TGF-β1 m-RNA and its protein was not observed in other recent study that dealt with the same molecule and might have originated from the small sample size and/or post-transcriptional modifications (32). However, its elucidation requires further studies.
In this study, the expression of TGF-β1 in BAL cells showed a significant positive correlation with gestational age and birth weight. It increased as gestational age and birth weight increased. When maternal chorioamnionitis was present, the expression of TGF-β1 in BAL cells significantly decreased independently of gestational age and birth weight. If our data are acceptable as a reflection of actual alveolar environment, it could be suggested that the expression of TGF-β1 in the lungs increases as a function of maturity, and that maternal chorioamnionitis exerts a negative influence on this normal increase of TGF-β1 expression at the later phase of human lung development. These findings may be thought to be an indirect evidence showing the possibility that maternal chorioamnionitis might inhibit normal lung development of fetus, although the exact role and the expression status of TGF-β1 in saccular phase are not known clearly. Be that as it may be, however, this assumption is not supported by our results in that there was no significant relationship between the expression of TGF-β1 in BAL cells and the development of BPD.
There should be another caution in interpreting our results. The study subjects in our study were preterm infants who needed tracheal intubation in delivery room. However, they were relatively larger preterm infants with a mean birth weight of 1,243±491 g and a gestational age of 29.5±3.1 weeks who can usually be managed successfully without intubation in delivery room nowadays. Therefore, there is a possibility that the preterm infants enrolled to our study might have suffered some antenatal insults such as maternal chorioamnionitis and perinatal asphyxia. Actually, the incidence of maternal chorioamnionitis is as high as 37% and the 5-min Apgar score was as low as 5±2, each of which is higher and lower than 27% and 7±2, respectively, of our previous epidemiologic study enrolled preterm infants who have similar birth weight and gestational age irrespective of whether tracheal intubation was done or not in delivery room (3). This difference supports the likelihood of a higher proportion of antenatally adversely affected preterm infants in our present study. Therefore, hasty generalization of our results should not be made.
In conclusion, positive correlation of TGF-β1 mRNA expression in BAL cells obtained from preterm infants shortly after birth with maturity and decreased expression of TGF-β1 mRNA in the presence of maternal chorioamnionitis suggest a possibility that maternal chorioamnionitis might inhibit the normal lung development of fetus. However, further studies will be necessary to delineate the representativeness of non-bronchoscopic BAL cells of alveolar environment and search for better easily obtainable pulmonary specimens that have a good reflection of alveolar environment in human preterm infants.




 XML Download
XML Download