

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sudden death (SD) is a serious social problem and much attention and studies have been conducted to prevent SD, especially in the young and active. As the number of patients with coronary artery disease (CAD) is increasing rapidly, safe sex is an important issue for both medical professionals and lay people as well. Routine sexual activity is regarded as an activity of mild to moderate intensity (1). However, it is also expected that routine sexual activity in subjects with organic heart disease such as CAD may trigger SD. The investigation of SD related to sexual activity may be difficult as it may be regarded as shameful or disgraceful to the family members and, especially, to the remaining partner. Thus, we could expect considerable bias in the investigation of SD related to sexual activity. Recently sildenafil or similar medications have become available and many patients and spouses are willing to be more sexually active than before and health care professionals are expected to provide reasonable advice on their sexual activity. However, only a handful of studies of SD related to sexual activity are available and only one study from the East Asia, published more than 40 yr ago, is available (2-4).
The aim of this study was to assess the causes and clinical characteristics of SD related to sexual activity in Korea.
MATERIALS AND METHODS
Daegu-Kyungpook is a 19,908 km2 region of Korea with a population of 4.8 million according to the census from the year 2005. Although Korean law does not mandate postmortem examinations following SD, an autopsy is usually conducted in the case of unwitnessed or sudden unexplained death. Most of the autopsies in the Daegu-Kyungpook region of Korea were performed by pathologists from the Department of Forensic Medicine at Kyungpook National University, Daegu, Korea. We had the opportunity to estimate the clinical characteristics of SD related to sexual activity. Sexual activity was defined as usual heterosexual coitus. From August 2001 to November 2005, all autopsies performed at Kyungpook National University were prospectively examined for SD cases related to sexual activity from the police reports. SD was defined as unexpected death within 1 hr after the symptom onset in witnessed cases, and within an estimated 24 hr under normal condition in unwitnessed cases. A complete medicolegal autopsy, including the brain, was performed in every case. In addition, all autopsies were followed by a toxicological analysis for a panel of illicit drugs. Coronary luminal stenosis of more than 70% was considered significant.
RESULTS
Fourteen cases (1.0%) of SD related to sexual activity were found out of 1,379 autopsy cases (Table 1). They were 46±11 yr old and 9 were male. All victims were heterosexual. The toxicological study showed no evidence of illicit drug use in any of the subjects. No one was taking sildenafil or any similar medications. A history of drinking just before their sexual activity was observed in 5 cases (Nos. 3, 4, 8, 13, and 14). However, the amount of drinking was moderate in most cases and ethanol was detected only in case No. 3 with a blood level of 0.145%. Ten cases were witnessed; during sexual activity in 4 cases, just after sexual activity in another 4 cases, 2 and 5 hr after in 1 each case. In 4 unwitnessed cases the victims were found dead less than 12 hr from the end of their sexual activity. The sexual partners were steady extramarital partners in 8 cases, unknown in 3, prostitutes in 2 and a marital partner in 1 case. The SD took place in the victim's own home only in 1 case. The other places that the SD and sexual activity occurred were hotel in 10 cases, steady extramarital partner's home in 2 and brothel in 1.
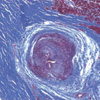
The mean heart weight was 391±93 gram and somewhat heavier in males than in females (410±109 vs. 356±42 gram, p=0.25). The causes of the SD were as follows; CAD in 6 (4 in males), subarachnoid hemorrhage (SAH) with ruptured berry aneurysm in 4 (3 in females), fibromuscular dysplasia of the atrioventricular nodal artery in 2, and unknown in 2. Cases No. 6 and No. 8 had histories of hypertension and old myocardial infarction, respectively. History of chest discomfort or pain was reported in two cases (No. 9 and 11). The histories of the other victims were unremarkable in this regard. Among 6 cases of SD due to CAD, multivessel disease was detected in 4 cases and evidence of old myocardial infarction was observed in 2 cases (Nos. 8 and 13). In 4 cases of SAH the ruptured aneurysms were found in the middle cerebral artery in 3 cases and basilar artery in 1 case. Multiple aneurysms including ruptured and unruptured were observed in 1 case (No. 7) (Figs. 1, 2, 3).
DISCUSSION
The results of this study showed that CAD and SAH are important causes of SD related to sexual activity in this region of Korea. Although the gender differences in the incidence of CAD and SAH were statistically not different, the male dominance of CAD and female dominance of SAH were similar to the other previous reports (2, 5, 6). The Korean statistics of death also showed similar findings of a gender difference with a higher incidence of death due to CAD in men and cerebrovascular accidents in women (Korea National Statistical Office. http://www.nso.go.kr). Our data could be considered similar to the previous reports (2-4) of SD related to sexual activity; in which most victims were male, the most frequent cause was CAD, and most partners were extramarital. Compared to the Japanese and German reports (2-4), the incidence of SAH as a cause of SD related to sexual activity was higher and the incidence of CAD was lower. The frequency of SD related to sexual activity was 1.0% of all autopsies in this study. Compared to the Japanese and German data (2, 4) of 0.61% and 0.18%, respectively, the incidence in our study seems higher. Probably it was influenced by many factors including genetic and cultural differences.
The results of this study may be considered as supporting the common belief that sexual activity with an extramarital partner may increase the risk of SD as compared to that with marital partners. It is natural to assume that sexual activity with an extramarital partner or prostitute, especially in an unfamiliar setting, may lead to significant increase in blood pressure and heart rate, which may result in SD or nonfatal cardiac events. Unfortunately, we do not have enough evidence to support the assumption that sexual activity between marital partners is safer. However, SD develops with sexual activity between marital partners and even manual stimulation was reported to induce SD (2-4). The public prosecutors also may not pay much attention to this kind of SD between marital partners unless there is an evidence of a crime. So the true incidence of SD related to sexual activity, at least, between marital partners may be severely under-reported. In contrast, SD related to sexual activity between extramarital partners may have a significantly higher chance of undergoing a full investigation including an autopsy.
Six cases of SD were due to CAD; 4 in males and 2 in females. Partners were extramarital in all cases. The absolute risk of myocardial infarction caused by sexual activity is known to be extremely low and transient, even in patients with known CAD (7). Myocardial ischemia or ventricular arrhythmias may be the cause of SD related to sexual activity in patients with CAD (8, 9). We also observed similar findings in which four out of six cases of SD due to CAD occurred during or just after sexual activity as in the Japanese and German reports (2-4). Only case No. 8 had had a history of an old inferior myocardial infarction. However, evidence of old myocardial infarction was observed in cases No. 8 and 13. In case No. 11, the victim complained of chest pain a few hours before her death further suggesting the presence of an acute coronary syndrome. Although sexual activity is a potential trigger of a myocardial infarction, the real risk of cardiac events including SD associated with sexual activity may be regarded as not being significant since sexual activity with a familiar partner may be considered as being an infrequent activity in most situations and any increase in the risk of a myocardial infarction is transient lasting only a few hours (1, 7, 10). One study from Israel (11) showed that only less than 1/3 of deaths due to ischemic heart diseases were exercise related, which may further complicate the interpretation of these findings.
SAH due to a ruptured cerebral aneurysm is still an important cause of death in Korea despite steady advances in diagnosis and treatment (Korea National Statistical Office). SAH has been a common cause of SD in women in previous studies (5, 6, 12). The high incidence of SAH and/or intracranial aneurysms in the 5th decade of life in women in the middle cerebral artery was also observed in our study (5, 6, 12). Patient No. 7 had two aneurysms; a ruptured huge aneurysm in the left middle cerebral artery and unruptured aneurysm in the right middle cerebral artery. The size of the aneurysm was less than 5 mm in patient No. 9 and she complained chest discomfort during sexual activity with moderate stenosis in coronary artery. Although transient hemodynamic changes associated with sexual activity seem to play some role in the pathogenesis of SAH, the mechanism of physical activity induced SAH is still not completely understood. Although about 4% of SAHs were reported as related with sexual activity, the correlation of the intensity of the physical activity at the time of the rupture also has shown varying results (6, 11, 12). Better methods for detecting silent and unruptured cerebral aneurysms are needed to prevent SD in these victims.
Fibromuscular dysplasia of the AV nodal artery with severe luminal stenosis was observed in 2 young men. Although mild to moderate, sometimes even severe, luminal stenosis has not been rare in normal controls, severe stenosis has been reported as more prevalent in victims of SD (13-15). At least some SDs in patients with this abnormality was not bradycardia-related as a patient with both this abnormality and permanent pacemaker could not escape from SD (13).
Two victims in this study had no significant abnormalities which can explain the cause of the SD in them. Previous studies on SD in Korea also showed a high incidence of structurally normal hearts and SD during the night or sleep (16, 17). Cardiac arrest with groaning in patient No. 2 occurred 5 hr after the end of his sexual activity and he was sleeping at that time, which was quite similar to the typical history of Brugada syndrome. As we did not have the medical records of the victims including their ECGs, we were not able to rule out SD due to so-called electrical diseases such as Brugada syndrome or long QT syndrome which may have had no direct relation to the sexual activity.
This study has some limitations. Because we were not working within the context of a formal registry of SD, and because Korean law does not require autopsies in all cases of SD, the true incidence of SD related to sexual activity remains unknown. Most information was obtained from police reports in most cases and those reports may not reliable in some cases. Thus, direct comparison between SD related to sexual activity and SD unrelated to sexual activity was not possible. The selection bias between the marital versus extramarital relations is also unknown. Luminal stenosis of the atrioventricular nodal artery due to fibromuscular dysplasia may not the real cause of the SD. Some SD may be due to so-called electrical diseases such as long QT syndrome or Brugada syndrome.



 XML Download
XML Download