

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatitis B virus (HBV) is one of the major causative agents of chronic liver diseases, including asymptomatic carrier (ASC), chronic hepatitis (CH), liver cirrhosis (LC) and hepatocellular carcinoma (HCC) (1). HBV infection is especially prevalent in African and Asian countries such as Korea, Japan, Taiwan and China because most patients with chronic HBV infection have acquired the infection perinatally from carrier mothers (2, 3).
Liver injury associated with HBV infection is mediated predominantly through an immune mechanism (4). This immune response is influenced by age at infection, host genetic factors and the genetic variability of the virus (5).
The serological heterogeneity of the hepatitis B surface antigen (HBsAg) has been well established. HBV isolates have been classified into 9 different subtypes according to the antigenic determinants of their HBsAg (6, 7). However, the classification of HBV by serologic subtype is not rational because a single point mutation at the S gene may result in a change in subtype (8). Therefore, according to the molecular evolutionary analysis of the genomic DNA sequence, HBV strains isolated in various countries are classified into 8 genotypes: genotypes A to H (9-11). It is a distinct trend that the distribution of HBV genotypes throughout the world is specific to location. For example, genotype A is prevalent in the United States, Europe, and Central Africa (10, 12, 13). The incidence of genotype B and C varies markedly among Asian countries (14, 15).
Recently, the influences of HBV genotypes in manifestation of clinical liver disease have been reported (16-21). However, results concerning the distribution of HBV genotypes and the association between the distinct genotypes and the severity of liver disease in Korea remained unreported. A previous comparative study of HBV-associated liver diseases between the southern part of Korea and western part of Japan has shown a difference in severity of liver disease. The HBsAg positive rate of patients with LC and HCC was higher in Korea than in Japan (22). Moreover, mortality rates of HCC among Koreans were higher than those among Japanese (23).
In the present study, we used a monoclonal antibody of the epitopes specific for each HBV genotype and classified the epitopes into five serotypes: bsu, bm, bks, bksu, and bk, which are equivalent to genotypes A, B, C, D, E, and F respectively. By using this enzyme-linked immunosorbent assay (ELISA), we investigated the prevalence of HBV genotypes and the association between distinct genotypes and the severity of liver disease in Korea.
MATERIALS AND METHODS
Patients
A total of 120 serum samples with positive for HBsAg were obtained from chronic HBV carriers (65 from Seoul and 55 from the other city in Korea) who underwent long-term follow-up at Kangnam St. Mary's Hospital, the Catholic University of Korea, Seoul, Korea. They included 30 asymptomatic HBsAg carriers (ASC, persistently normal serum alanine aminotransferase levels for at least 2 yr in periodic biochemical examinations every 3 or 6 months), 30 CH, 30 LC, and 30 HCC. Chronic hepatitis was diagnosed from liver biopsy samples by sono-guided needle aspiration. Liver cirrhosis was diagnosed by liver function and sonogram. The diagnosis of HCC was established in liver-biopsied specimens, and typical features were noted on angiography. Serum samples from each subject were taken and stored at -80℃ until virological tests were performed. For patients with histologically verified chronic liver disease, serum samples were collected when liver biopsies were performed.
Serological markers and detection of HBV DNA
HBsAg and hepatitis B e antigen (HBeAg) were determined by a commercially available kit (Abbott Laboratories, Abbott Park, IL, U.S.A.). Detectable HBV DNA in serum was quantified by Quantiplex branched DNA assay (Bayer Diagnostics, Berkeley, CA, U.S.A.; sensitivity 2.5 pg/mL)
Serological determination of the six HBV genotypes
The six major genotypes of HBV, i.e. A, B, C, D, E and F were determined by ELISA with commercial kits (HBV Genotype EIA, Institute of Immunology, Tokyo, Japan) according to the method described by Usuda et al. (24). First, HBsAg particles in test sera were captured by immobilized antibody to the common determinant of HBsAg. Then, they were subjected to binding with monoclonal antibodies against five distinct preS2 epitopes, designated b, k, m, s, and u, which were labeled with horseradish peroxidase (HRP). Since the expression of these five epitopes is influenced by HBV genotypes, the combination thereof enables us to determine the genotypes serologically. The epitope b is shared by HBsAg of all genotypes. Genotypes A, B, C, D, and F were distinguished by five serotypes recognized by respective mAbs, i.e. bsu, bm, bks, bksu, and bk. Thus, the serotype bsu is specific for genotype A, bm for B, bks for C, bksu for D, E and bk for F. The validity of this ELISA for serological determination of the five HBV genotypes has been verified previously (24).
Determination of genotypes by HBV DNA sequences
HBV genotype in six samples was determined by phylogenetic analysis using the method described previously (25). Nucleic acids were extracted from 100 µL of serum, using a DNA extractor kit (Genome Science Laboratory, Fukushima, Japan). The entire small S gene (681 bp) was amplified by two overlapping fragments. The PCR primers for the first round consisted of sense: 5'-AAG CTC TGC TAG ATC CCA GAG T-3' (SS1: 18-39) and anti-sense: 5'-CAT ACT TTC CAA TCA ATA GG-3' (SS2: 989-970); the primers for the second round were sense primer SS1, antisense: 5'-GAA ACA TAG AGG TGC CTT GAG CAG-3' (SS3: 557-634) and sense: 5'-TGC TGC TAT GCC TCA TCT T-3' (SS4: 414-433), antisense primer SS2 (25). Amplified HBV DNA fragments were sequenced directly by the dideoxy method using a Taq Dye-Deoxy Terminator cycle sequencing kit and a fluorescent 3100 DNA sequencer (Applied Biosystems, Foster City, CA, U.S. A.). The primers used for the sequencing were the second set of primers described above for PCR.
Statistical analysis
Differences between groups were examined by Student's t-test, Fisher's exact probability test or the Mann-Whitney rank test. A two-tailed p value of less than 0.05 was considered to be significant. Data analysis was performed using SPSS software (version 10.0, Chicago, IL, U.S.A).
RESULTS
Clinical features of patients with chronic hepatitis B
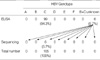
The demographic, virological, and clinical characteristics of the carriers with chronic hepatitis were summarized in Table 1. A family history of positive for HBsAg, as determined through an interview during the first visit, was noted in 76 patients (63%). Incidence of alcohol consumption, operation and transfusion history was present in 48 (40%), 34 (28%), and 10 (8%) carriers, respectively. HBeAg and HBV DNA were detected in 47 (39%) and 58 (48%) carriers, respectively. Clinical backgrounds in carriers with different stages of liver disease are shown in Table 1. In each group, no statistically significant differences were observed between family history of HBV infection and history of transfusion, operation and drinking. The level of albumin and γ-glutamyl transpeptidase was significantly lower in the group of LC and HCC than in other groups (p=0.045 and p=0.039). The alanine aminotransferase (ALT) levels had tendency to increase in carriers with CH, LC and HCC than that of ASC. The HBeAg positive rate was significantly higher in the carriers with CH and LC than in those with ASC and HCC (p=0.001), and the HBV DNA positive rate was significantly higher in the carriers with ASC, CH and LC than in those with of HCC (p=0.032).
Distribution of HBV genotypes in 120 patients with chronic hepatitis B
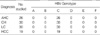
HBV genotypes were determined by ELISA with monoclonal antibodies against pre S2 determinants. Of the 120 serum samples, 21 (17.5%) were negative for ELISA. Among them, HBV DNA was amplified in 6 samples, and HBV genotypes were determined by direct sequencing of the small S gene (Table 2). Finally, the 105 patients (26 ASC, 30 CH, 30 LC and 19 HCC) were analyzed the genotypes of HBV (Table 3). HBV genotype C was identified all of the carriers with ASC, CH, LC and HCC. Genotypes A, B, D, E and F were not detected in any of them. All HBV carriers in Seoul and the other cities had genotype C.
DISCUSSION
HBV strains isolated in various countries are classified into 8 genotypes: genotypes A to H (9-11). These genotypes are recognized as distinct if differences of more than 8% exist in the entire nucleotide sequence of approximately 3,200 nt. The preS2-region has less constraint on the sequence and would be more variable than the S gene, making it a better candidate than the S gene as the basis of genotypic divergence. With such a rationale, epitopes on the preS2-region product which would reflect genotypes were selected. Monoclonal antibodies which recognized epitopes borne by the preS2-region product were obtained. The present study used an ELISA method to classify HBV genotypes (24). ELISA is a rather simple method and takes only a short time (about 6 hr), although genotypes are currently determined by restriction fragment length polymorphism (13, 26). With the methods in this study, it was possible to classify HBV into five types: HBV genotypes A, B, C, D, E and F based on a combination of epitopes detected with monoclonal antibodies, for example, a common epitope observed on all HBV genotypes, and a specific epitope on the respective HBV genotype.
It is a distinct feature that the distribution of HBV genotype throughout the world is specific to geographical location. Genotype A is prevalent in the United States, Europe, and Central Africa (10, 12, 13). Genotype B and C are frequent in Asia, especially Southeast Asia and Far East Asia (21), and D is prevalent worldwide, with particular presence in the Mediterranean area, Central Asia, and South America. Genotype E is restricted to West Africa, and genotype F prevails in Central and South America (27). Genotype G was determined very recently in France and Georgia of the U.S.A., and its distribution is yet to be investigated (10).
The incidence of genotype C varies markedly among Asian countries (16, 18, 21). In our study, we found that all 105 (100%) patients were HBV genotype C regardless of disease severity in Korean and the outcome of this study is comparable with the results of previous studies in Korea (28, 29). As in the results from Shanghai, China and Japan, genotype C was found in most patients with chronic HBV infection in Korea. As a note of comparison, genotype B was predominant in Taiwan. Genotype C was especially predominant in the central regions of Japan, reaching a distribution of over 95% comparable to that in Korea, suggesting the migration from other Asian countries to the Japanese archipelago. It was reported that people from Northeast Asia migrated to Japan via the Korean peninsula about 2,300 yr ago, displacing the people to the south and north (30). Besides epidemiological distributions, HBV genotypes would also be able to trace the population movement; the route of infection is mainly found from mother-to-infant perinatally in Asian countries (31), suggesting that the HBV genotype may be highly conserved in the same population by vertical transmission from mother to baby, especially in Southeast Asia, including Korea. There were significant differences reported regarding geographic distribution; genotypes C and B were predominant in Japan, while Korea expressed no difference in geographic distribution between in and around Seoul and Jeju island, which is located far away from the Seoul, but close to Japan (28) and genotype C prevailed. This study also shows the same result (Table 2, 3). The differences between the two close countries can be associated with the route of migration; people from Northeast Asia and Southern Asia migrated to Japan, but the migration to Korea occurred only from Northeast Asia, with some subsequent migration to Japan (18).
It has been reported that HBV genotypes exert their influence through a point mutation in the precore region for an HBeAg-minus phenotype, from G to A nucleotide 1896, which is associated with the loss of HBeAg. Li et al. was the first to note that the HBV genome of genotype A had C 1858 and implicate it in a rare HBeAg seroconversion. Patients with genotype A were significantly more likely to be HBeAg-positive at first examination compared with results in patients with genotypes B and C (32). In contrast, genotype C strains are heterogenous with respect to T or C as nucleotide 1858 mutations in the HBV genome were associated with HBeAg as well as viral replication (33). The G1896A mutation changes a wobble G-T for a Watson-Crick A-T pair in genomes with T1585, although it is precluded in those with C1858 because it results in a forbidden C-A pair. In addition, core mutants were more frequent in genotype C strains and were associated with more inflammation and fibrosis of the liver than those in genotype B (34). These findings suggest that pathogenic differences between genotypes may exist and the core mutation may be useful as a marker for progressive liver damage. Patients with genotype C appeared to be correlated with lower seroconversion rates, severe liver damage, higher replicative activity and more-severe liver inflammation than those with genotype B (16, 34).
Cirrhosis was ascribed to HBV (58%), alcohol (26%), hepatitis C virus (11%) or both (2%), or was cryptogenic (3%) in Korea (35). HCC is a major public health problem in Korea, where it is the sixth most common cause of death, reported by Korean National Statistical Office in 2002, and is probably linked to the high prevalence of HBV infection (58%) and to the culture which encourages high alcohol consumption. The HBsAg positive rate of patients with liver cirrhosis and HCC was higher in Korea than in Japan (22, 36). Mortality rates of HCC among Koreans are also higher than those among Japanese (23). These may be related to a higher rate of HBsAg carriers, heavy drinking, and the predominance of genotype C in Korea (23, 28, 37). Furthermore, low clearance of interferon-induced HBeAg loss in genotype C might be an additional factor of poor prognosis in patients with chronic HBV infection (38).
In conclusion, genotype C HBV prevails predominantly among Korean chronic carriers of the virus, irrespective of their clinical stages of liver disease and geographic origin, indicating that it may associate with more advanced liver disease than any other country.

 XML Download
XML Download