

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Vitamin B12, commonly known as cobalamin, is a water soluble vitamin primarily obtained from the dietary intake of animal proteins, mainly meat and eggs. Vitamin B12 plays an important role in the production of red blood cells, DNA synthesis, and neurological functions. According to the National Health and Nutrition Survey, a person with serum vitamin B12 concentration ≥ 200–300 pg/mol is defined as vitamin B12 deficient [12]. The prevalence of vitamin B12 deficiency in the general population is unknown. However, the incidence rate appears to increase with age [3].
Vitamin B12 deficiency causes demyelination of nerves in the central and peripheral nervous system and has been associated with peripheral neuropathy, loss of sensation in peripheral nerves, and weakness in the lower extremities [456]. The pathogenesis of this condition may be connected to a disturbance in the transfer of methyl groups to myelin basic protein, probably in the production of the lipids of myelin [7]. The recognition of this condition at an initial stage is necessary, as it is reversible and preventable [89].
Methylcobalamin is an active and effective form of vitamin B12 which treats or prevents the complications associated with vitamin B12 deficiency. It helps in the synthesis of methionine and S-adenosylmethionine. Methylcobalamin is required for the integrity of myelin (it covers and protect the nerve fibers), neuronal function, red blood cell formation, and DNA synthesis [10]. It is the only form of vitamin B12 that can cross the blood brain barrier without biotransformation. Previous studies reported that methylcobalamin has a potential to regenerate nerve cells [1112].
The diagnosis of vitamin B12 deficiency is based on the measurement of serum cobalamin levels, however, about 50% of patients with subclinical disease have normal B12 levels [39]. Methylcobalamin accounts for 90% of the total cobalamin level in the cerebrospinal fluid (CSF), suggesting its correlation with the nervous system and making it more appropriate for use in neuropathy associated with vitamin B12 deficiency rather than other analogues [13]. The major route of administration is oral, although it has been administered by means of an intramuscular injection [14]. Injectable methylcobalamin was registered as a 500 µg unit dose ampule and recommended in a regimen of one injection every other day. This thrice weekly recommendation was in accordance with the prescription information provided by the innovator, Eisai pharmaceuticals, Japan [15]. Lately, there are higher dose ampoules of 1500 mcg available, which claim to replace the 3 weekly injections with just one. The difference in serum levels of cobalamin might affect the effectiveness of therapy. In India, both the regimens are followed by clinicians, however, no study has compared the two regimens to assess the levels of cobalamin after administration in the patients with peripheral neuropathy and healthy volunteers. The present study was conducted to evaluate the serum cobalamin levels after the administration of either regime in patients with peripheral neuropathy and healthy volunteers.
MATERIALS AND METHODS
1. Study design
This was a prospective, randomized, comparative study. The study was approved by the Ethics Committee of the Institute of Neurosciences, Kolkata and registered at Clinical Trials Registry, India with the registration number CTRI/2017/02/007804. All the subjects were recruited for two weeks with due consent prior to the study. The entire study duration was six months.
2. Study characteristics
Consenting patients of either gender diagnosed with peripheral neuropathy, aged 18 years or above, and attending the Neurology out-patients' department (OPD) of the Institute of Neurosciences, Kolkata, were included in the study. Pregnant or lactating women and subjects with history of previous exposure of clinically significant metabolic, hepatic, renal, hematological, pulmonary, cardiovascular, gastrointestinal, urological, neurological or psychiatric disorders were excluded from the study.
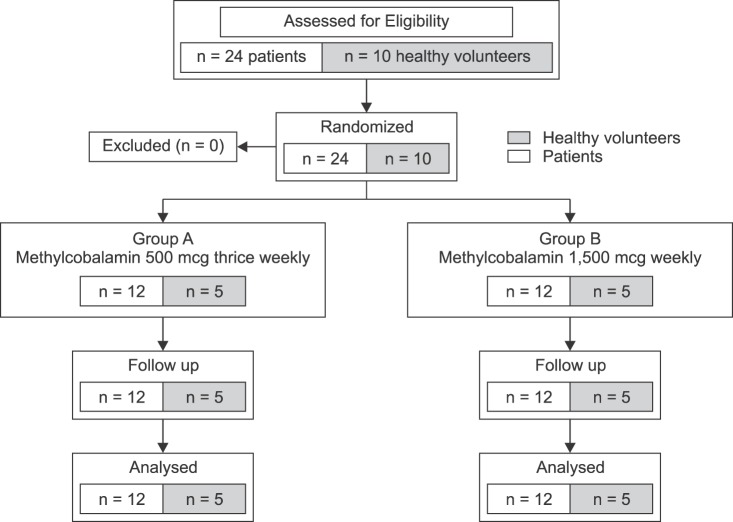
The study population was categorized into two parallel groups, Group A (methylcobalamin 500 mcg injection intramuscularly thrice weekly) and Group B (methylcobalamin 1500 mcg injection intramuscularly once a week). The study medication ampoules were stored in a cool, dark place away from light. A control group of healthy subjects (family members of patients aged > 18 years) was also included. Randomization was done with the help of a computer generated random number table into two parallel groups for 24 patients, and 10 healthy volunteers were randomized by balanced unstratified randomization using the Winpepi software ETCETERA version 2.32 program. Allocation concealment was done by the sequentially numbered opaque sealed envelope (SNOSE) technique. All the patients were followed up for 2 weeks (Fig. 1).
The primary outcome measure (serum cobalamin) was evaluated at baseline (BL), on Day 8, and at the end of treatment (ET), i.e., Day 15. Patients were asked to report at 10 AM, and the blood samples were collected at 11 AM. The injection of methylcobalamin was made at 12 PM. The Leeds Assessment of Neuropathic Symptoms and Signs Pain scale (LANSS: value > 12 indicating neuropathic mechanisms are contributing to patients' pain) which is a scale to assess the source of patients' pain [16] and a diagnostic questionnaire (DN4: value > 4 suggesting neuropathic pain) [17] to diagnose neuropathic pain were evaluated at BL and ET. All the adverse events (AEs) reported by patients or elicited by clinicians were recorded at each visit.
3. Statistical analysis
Continuous data was reported as mean ± standard deviation (SD) and categorical as percentage (%). The normality analysis was performed using the Kolmogorov-Smirnov (K-S) test. The clinico-demographic parameters were analyzed by chi-square/Fishers (for categorical data) or Student's t-test (for numerical data).
The parameters between groups were analyzed using the Mann-Whitney U test. Intra-group changes of cobalamin were done using Friedman's ANOVA, followed by a post hoc Dunn's test. Medcalc version 10.2 (Mariakerke, Belgium: MedCalc Software, 2011) was used for statistical analysis. A P value less than 0.05 (P < 0.05) was considered to be statistically significant. Sample size calculation was done by convenient sampling, as such a comparative study was the first of its kind.
RESULTS
1. Study participants
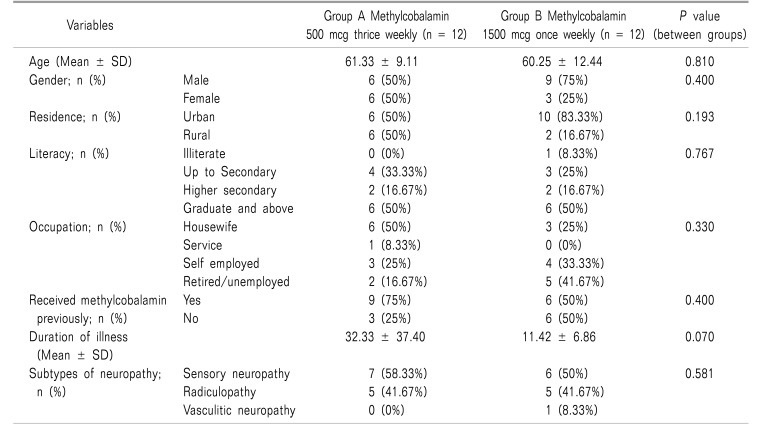
A total of 24 patients with neuropathic pain and 10 healthy volunteers were included in the study (Fig. 1). Both the groups, A and B consisted of 12 patients each having a mean age of 61.31 ± 9.11 years and 60.25 ± 12.44 years, respectively.
Five healthy volunteers in each group were also included as a control. A majority of the patients were men (62.5%). Most of the patients were literate (95.8%) and residents of an urban area (66.7%). All the study participants completed the study and none were lost to follow-up. The clinico-demographic characteristics of all the subjects are represented in Table 1.
2. Treatment outcomes
1) Changes in serum cobalamin level
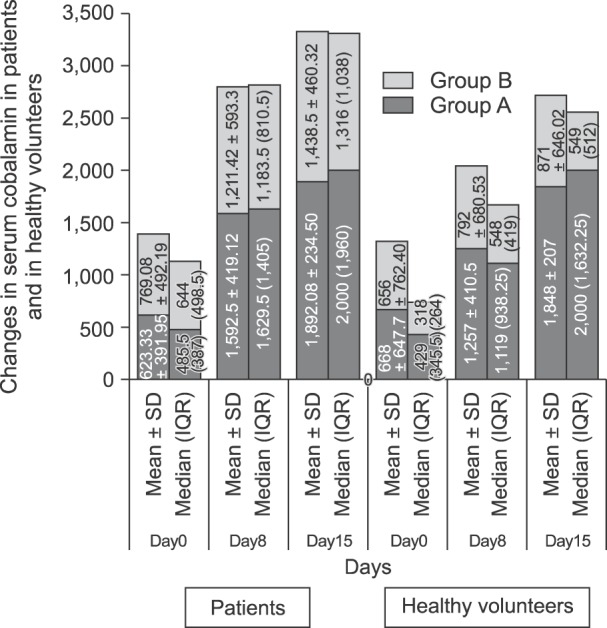
The change in serum cobalamin levels is presented in Fig. 2. At ET, both the groups showed a significant increase (P < 0.001) in serum cobalamin levels from BL. However, Group A showed a significant increase from Day 8, whereas Group B showed a significant increase from Day 15 when compared to BL. It was found that serum cobalamin level was significantly higher in Group A (1892.08 ± 234.50 IU) as compared with Group B (1438.5 ± 460.32 IU) at the ET (P = 0.028). In Group A, the increase in cobalamin levels from BL was 3 fold as compared with a 1.87-fold increase in Group B. The healthy volunteers in both the groups showed a significant increase (P = 0.093 in Group A, P = 0.009 in Group B) in serum cobalamin level at ET from BL. The increase in serum cobalamin levels was 2.76 and 1.33 times the mean BL value in Group A and Group B, respectively. When both the groups were compared, it was observed that the serum cobalamin levels in Group A volunteers was two times that of Group B and it was nearly significant (P = 0.056) (Fig. 2).
2) Changes in the LANSS scale and DN4 questionnaire after treatment
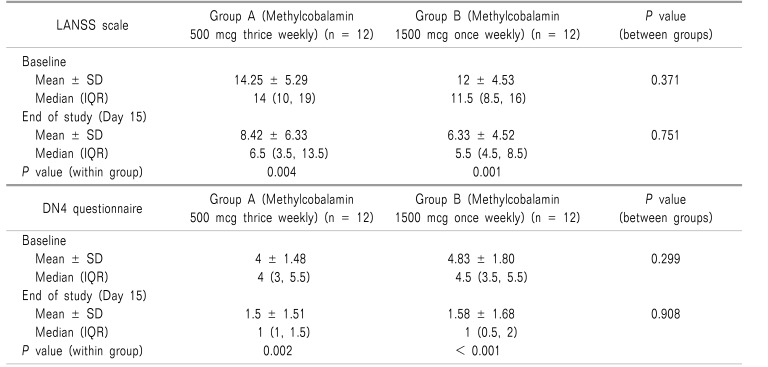
Both the LANSS scale and DN4 questionnaire showed similar results at ET. The data for changes in the LANSS scale and DN4 questionnaire is presented in Table 2. At BL, the LANSS pain scale was comparable in both the patient groups and value was > 12 suggesting neuropathic mechanisms are likely to contribute to the patients' pain. At ET, a significant decrease in the LANSS pain scale was observed in both the Group A (P = 0.004) and the Group B (P = 0.001). However, intergroup comparison at ET showed comparable changes (P = 0.751).
At BL, value of the DN4 questionnaire was > 4 in both groups indicating neuropathic pain. At ET, both the groups showed a significant decrease (Group A, P = 0.002 and Group B, P < 0.001) from BL value. The intergroup comparison between both groups showed comparable results at ET (P = 0.908).
3) Adverse drug reactions after the treatment
Four patients (33.3%) in Group A and one patient (8.3%) in Group B complained about pain during injection. Only one patient in each group complained about pain at the injection site and headache. It was observed that AEs were not statistically significant between the groups. Among the healthy volunteers, one person in each group complained about pain during injection (Table 3).
DISCUSSION
Vitamin B12 is a micronutrient that plays a substantial role in various biological processes. It is compulsory for the metabolism of folate and biosynthesis of nucleotides [18]. Prolonged vitamin B12 deficiency can lead to nerve degeneration and irreversible neurological damage [19]. The neuropathy associated with vitamin B12 deficiency is well-known in humans [20]. The United State Food and Drug administration (US-FDA) recommends a daily intake of 6.0 µg of vitamin B12. Food providing 20% or more of the daily requirement are considered a rich source of vitamin B12 [20]. The Institute of Medicine (IOM) reported that no AE has been associated with an excessive intake of vitamin B12 either from food or supplements [21].
Methylcobalamin, an active form of vitamin B12, plays an important role in transmethylation and acts as a coenzyme of methionine synthetase. It is required for the synthesis of methionine from homocysteine that involves the methylation of DNA or proteins [22]. It is well transported into nerve cell organelles and promotes nucleic acid and protein synthesis [23]. The efficacy of methylcobalamin has been documented in various experimental and clinical studies with respect to the regeneration of peripheral nerves in acrylamid neuropathy [24], uremic neuropathy [25], peripheral neuropathy associated with diabetic polyneuropathy [14] and leprous neuralgia [2627]. All these effects come together in the effectiveness of methylcobalamin in peripheral neuropathies.
Previous studies have demonstrated the protective role of methylcobalamin in patients with peripheral neuropathies. Yagihashi et al. observed that continuous treatment with methylcobalamin had a protective effect on the peripheral nerve lesions in experimental diabetic neuropathy [28]. Yamazaki et al. observed that methylcobalamin stimulates the regeneration of motor nerve terminals that were degenerating in the anterior gracile muscle of the gracile axonal dystrophy mutant mouse [29]. Naik et al. reported that methylcobalamin is necessary for the proper functioning of critical peripheral nerves impaired in different types of neuropathies and acts as an important tool in therapeutics [30]. Okada et al. reported that vitamin B12 may provide a basis for more beneficial treatment of nervous disorders through effective systemic or local administration of high doses of methylcobalamin to target organs [22].
However, the mode of the administration of vitamin B12 affects the serum cobalamin levels that, in turn, have an effect on the efficacy of active cobalamin. Methylcobalamin can be administered via intranasal, oral, and parenteral routes. The parenteral administration of methylcobalamin, usually intramuscular injection, is mainly used in the treatment of vitamin B12 deficiency caused by conditions which leads to malabsorption and severe vitamin B12 deficiency [20].
After absorption, vitamin B12 is highly bound to transcobalamin II, a specific carrier protein (which helps in the quick transport of the cobalamins to tissues) and is distributed and stored mainly in the liver as coenzyme B12. A significant amount of the absorbed vitamin B12 is also stored in the bone marrow. The half-life of methylcobalamin is about 6 days and elimination takes place through the bile; however, methylcobalamin in excess amounts is excreted unchanged in the urine. Absorption of methylcobalamin is optimal with an intramuscular injection as compared to oral administration, and therefore few injections are needed once the serum cobalamin levels reach an acceptable level. Intramuscular injection of methylcobalamin attains peak plasma concentration within one hour as compared to the oral dose (3 h). Thus, it is better to use intramuscular injections rather than oral doses for a faster effect [20313233]. In the present study, we observed that the rise in serum cobalamin levels was significantly higher in the patients receiving 500 µg thrice weekly than the group receiving 1500 mcg weekly. The rise in serum cobalamin levels was also confirmed in healthy volunteers where the thrice weekly regime of methylcobalamin produced a more significant rise than the weekly regime. It was observed that the 500 µg, thrice weekly regime produced a significantly rapid rise in serum cobalamin levels after the first week itself as compared to the weekly 1500 µg regime in both the patients and healthy volunteers. The same results were observed with the DN4 questionnaire and LANSS scale. The mechanism by which methylcobalamin produces positive effects on nerve damage is yet to be understood. We speculate that exogenous methylcobalamin accumulation stimulates nerve regeneration or remyelination. Biochemical findings suggest that in DNA metabolism, methylcobalamin directly acts as a methyl donor which may increase the synthesis of proteins for nerve regeneration [27]. Only a few patients reported AEs during the study, such as pain at the injection site and headache, which did not affect the efficacy of the drug. Since, the AEs were comparable and distributed in both the groups, the thrice weekly regime offers a higher serum cobalamin level. Maintaining a uniformly high dose is the first step in achieving a better clinical response. Our study was limited by the fact that each patient was studied for a two-week duration due to logistic reasons, which was insufficient to comment on their clinical improvement. The ease of once weekly higher dose injection of methylcobalamin is counteracted by a lower level of serum cobalamin value. Physicians thus must be aware of ease versus effectiveness in maintaining the serum cobalamin values of both the regimes of methylcobalamin while administering them to their patients. However, clinical studies with large population sizes and longer duration are needed for conclusive results.

 XML Download
XML Download