

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Postoperative pain is a common upsetting symptom following arthroscopic knee surgery. For effective, safe and long lasting post-arthroscopy analgesia, several analgesic strategies such as systemic medication, central or peripheral blocks, and intra-articular drug administration have been used to control postoperative pain [1].
Dexmedetomidine a highly selective α2 adrenergic agonist with sedative, anxiolytic, analgesic, sympatholytic and antihypertensive effects. It enhances the analgesic property of local anesthetics in various routes, such as the neuraxial, intra-articular and intravenous (I.V.) routes [2]. Studies have shown that intrathecal dexmedetomidine produced a better postoperative analgesic effect when added to hyperbaric bupivacaine in spinal anesthesia with minimal adverse events [345]. Alternatively, intra-articular dexmedetomidine was effective for prolonging postoperative pain relief [678].
C-reactive protein (CRP), an acute phase protein, is elevated in case of inflammation and stress response to surgical trauma [9]. Dexmedetomidine may have a role in the attenuation of inflammatory mediators and surgical stress response [10].
We hypothesized that the addition of intrathecal or intra-articular dexmedetomidine to spinal bupivacaine would lengthen postoperative analgesia following knee arthroscopy. The study was designed to find the best route for dexmedetomidine administration in prolonging postoperative analgesia in patients undergoing knee arthroscopy. So, the study aimed to compare the effect of intrathecal versus intra-articular dexmedetomidine on postoperative pain following arthroscopy.
The primary outcome of our study was postoperative pain as assessed by the visual analogue scale of pain (VAS). Secondary outcomes included the effect of dexmedetomidine on total postoperative analgesic use and time to the first analgesic request, hemodynamics, sedation, postoperative nausea and vomiting, patient satisfaction, and postoperative serum CRP levels.
MATERIALS AND METHODS
Our current randomized double-blind controlled study got an approval from the Assiut University (Assiut, Egypt) ethical committee, and was registered in ClinicalTrials.gov (ID: NCT02581566). For enrollment, an informed consent was signed by all study participants in the orthopedic department of Assiut University hospital. Between November 2015 and April 2016, ninety patients between 20 and 50 years old with American Society of Anesthesiologists (ASA) classification I-II who had undergone elective unilateral arthroscopic knee surgery under intrathecal anesthesia were enrolled in this study.
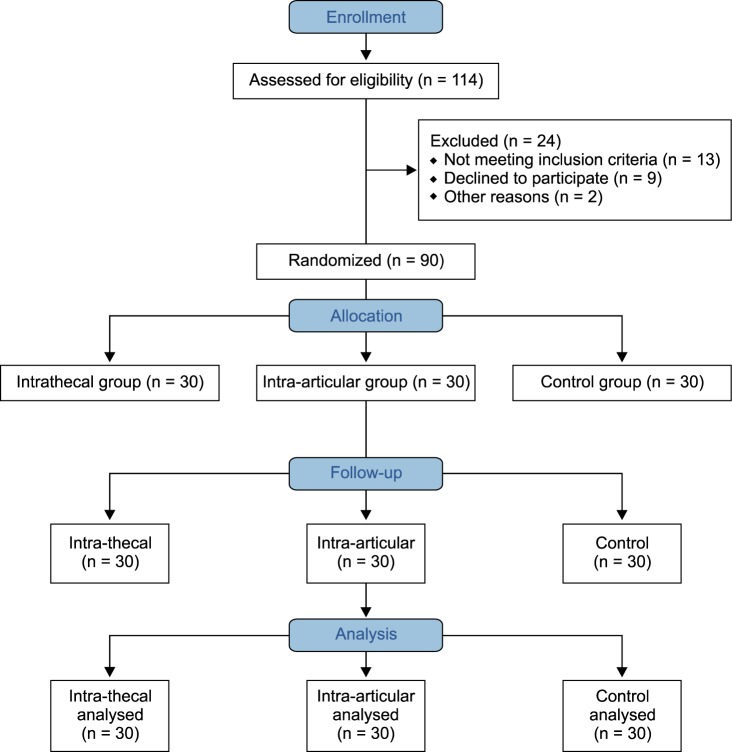
Exclusion criteria included the presence of any absolute or relative contraindications for intrathecal anesthesia, drug allergy, chronic use of pain medications, and refusal to participate. The Fig. 1 shows the CONSORT Flow Diagram. Out of 114 eligible patients, 90 patients were enrolled and completed the study.
In the preoperative holding area, the procedure was explained to the patients and they were familiarized with the VAS (graded from 0 = no pain to 10 = maximum pain). An intravenous line was secured and all patients were preloaded with Ringer's lactate solution 10 ml/kg. In the operating room, routine monitors such as electrocardiograph leads II & V5, heart rate, pulse oximetry, and non-invasive blood pressure were connected to the patient; baseline vital parameters like heart rate (HR), mean arterial blood pressure (MAP), and arterial oxygen saturation (SpO2) were recorded.
All patients received an intrathecal block which was performed using the midline approach with a 25-G Whitacre needle (Product # 405138, BD™, Franklin Lakes, NJ). Hyperbaric bupivacaine 0.5% 2.5 ml was injected into the L3-L4 intervertebral space, in a completely aseptic environment, with the patient in sitting position.
Randomization using envelopes to assign participants to a treatment group is a simple strategy that attempts to conceal the allocation sequence. Patients were randomly assigned into three groups using the sealed envelope method [11]; the intrathecal (IT) group (n = 30) received 1 ml of preservative free 0.9% saline containing 5 µg dexmedetomidine (Precedex®, Hospira Inc., Lake Forest, IL) with the intrathecal block.
After skin closure following arthroscopy and 10 m before tourniquet release, 20 ml of preservative free 0.9% saline was injected intra-articularly for every patient in this group. The intra-articular (IA) group (n = 30) received 1 ml of preservative free 0.9% saline with the intrathecal block. Additionally, they received 20 ml of preservative free 0.9% saline containing 1 µg/kg dexmedetomidine intra-articularly after skin closure and 10 m before tourniquet release. The control group (n = 30) received 1 ml of preservative free 0.9% saline with intrathecal block plus 20 ml of preservative free 0.9% saline intra-articularly after arthroscopy and 10 m before tourniquet release. The intra-articular injection was done through arthroscopy at the end of the procedure by the surgeon (without knowing the contents), to ensure drug delivery into the joint. Study medications were prepared by an anesthesia assistant not involved in the study. Surgeons, anesthesiologists, and personnel who helped in patient care or data collection were all unaware of the patients' allocation group.
HR and MAP were recorded intra-operatively at 5, 10, 15, 20, and every 10 m thereafter until 60 m post-intrathecal injection. Then, they were recorded at 90 m and at 2, 4, 6, 8, 12, 18, and 24 h after the intrathecal injection. Bradycardia (HR decrease by 20% from the baseline) was managed by 0.5 mg I.V. atropine. Hypotension (MAP decrease by 20% from the baseline) was treated by fluids and/or 5 to 10 mg I.V. ephedrine.
Postoperative pain on movement was assessed by using the VAS, which was recorded at 2, 4, 6, 8, 12, 18, and 24 h after the intrathecal injection. Meperidine 1 mg/kg was given when the VAS ≥ 4 or the patient requested analgesia. The time of the first postoperative analgesia request and total meperidine consumption during the first 24 h were recorded. All data was collected by an observer who was uninformed of the patients' group assignment.
Patient satisfaction with analgesia was measured using the global patient satisfaction score verbally at 8 h and 24 h after the intrathecal block. The score includes the following scales: (1) very dissatisfied; (2) slightly dissatisfied; (3) neither satisfied nor dissatisfied; (4) satisfied; and (5) highly satisfied [12]. For the purposes of the study, scales 1, 2 and 3 were categorized as non-satisfied while scales 4 and 5 were categorized as satisfied.
The patients' level of sedation was assessed intraoperatively every 15 m and postoperatively hourly for 6 h using the Ramsay sedation scale [13]. The incidence of PONV was recorded during the first 24 h postoperatively.
Two blood samples (5 ml each) were collected for measuring serum C-reactive protein (CRP); the 1st was taken pre-operatively and the 2nd was taken 24 h post-intrathecal block. CRP was measured using high-sensitivity CRP (hsCRP) technique [1415]. The assay was batched and run as per manufacturer's instructions with a sensitivity of 0.1 ng/ml and a detection limit of 0.5-100 ng/ml (Product # ABIN626326, Aachen, Germany). Samples were diluted 1 : 100-1000 to be within the linear detection range, and final patients' results were reported in mg/dl [16].
1. Statistical analysis
The study power effect was calculated for the highest pain score on the VAS scale (β = 1) and for time of rescue analgesia (β = 0.992). For both, the power was above 80%. Power analysis was done using a Power and Sample size calculator [17].
We used the VAS as the primary variable, and assumed that dexmedetomidine would detect a difference of 1 cm on the VAS at an alpha threshold of 5%. The calculations were based upon preliminary data that showed dexmedetomidine can improve VAS by at least 0.75 standard deviations (SD). That is, Δ = 0.75 SD in our notation. To have 80% power to detect an effect size, it would be sufficient to have a total sample size of n = (5.6/0.75), 2 = 55.75, or n/2 = 28 in each group. We enrolled 30 patients in each group for possible dropout.
We examined the data collected for pain and record review for normal distribution using the Kolmogorov-Smirnov test. The Kruskal-Wallist test was used for non-parametric data. Two-way repeated measure analysis of variance (ANOVA) was used for continuous variables, followed by post hoc testing, using the Dunnett test, to examine significant differences between the experimental and placebo control groups. Results were presented as mean ± SD or a percentage according to their category. P < 0.05 was considered significant. Statistical analysis was done by using GraphPad Prism version 5.03 for windows (GraphPad Software Inc, CA, www.graphpad.com).
RESULTS
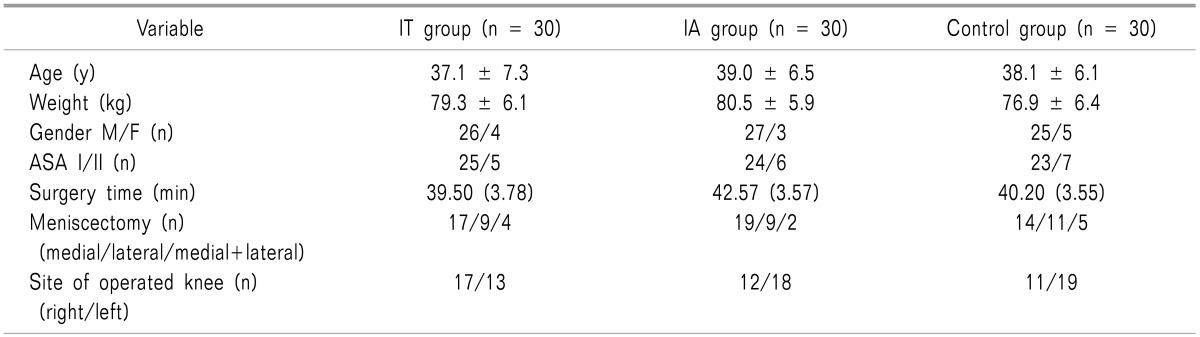
The study recruited 90 adult patients (30 patients in each group) who underwent unilateral knee arthroscopy under spinal anesthesia. The three groups showed no significant differences regarding age, weight, gender, ASA status, duration of surgery, localization of the partial meniscectomy (medial, lateral, or both), or site of the operated knee (right or left) (Table 1).
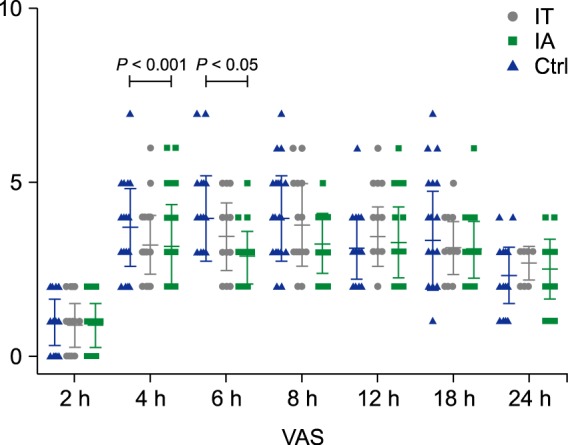
On movement, the mean VAS score at 2 h post-intrathecal block was not significant among the three groups. However, at 4 h post-intrathecal block, the control group showed a significantly higher value compared to the other 2 groups, with no significant differences between the IT group and the IA group. At 6 h post-intrathecal block, the IA group had significantly lower VAS scores compared to the other 2 groups. However, after 8h, the intensity of pain was comparable among all the patient groups (Fig. 2).
The difference in the mean time of the first rescue analgesic request (m) was significant among the three groups (359 ± 30, 413 ± 34 and 224 ± 36 for the IT, IA, and control groups, respectively) with the longest being in the IA group. Postoperatively, the mean total consumption of meperidine rescue analgesia (mg) during the first 24 h was significantly reduced in the IT and IA groups (110 ± 31 and 104 ± 26, respectively) compared to the control group (128 ± 32), with no significant difference between the IT and IA groups.
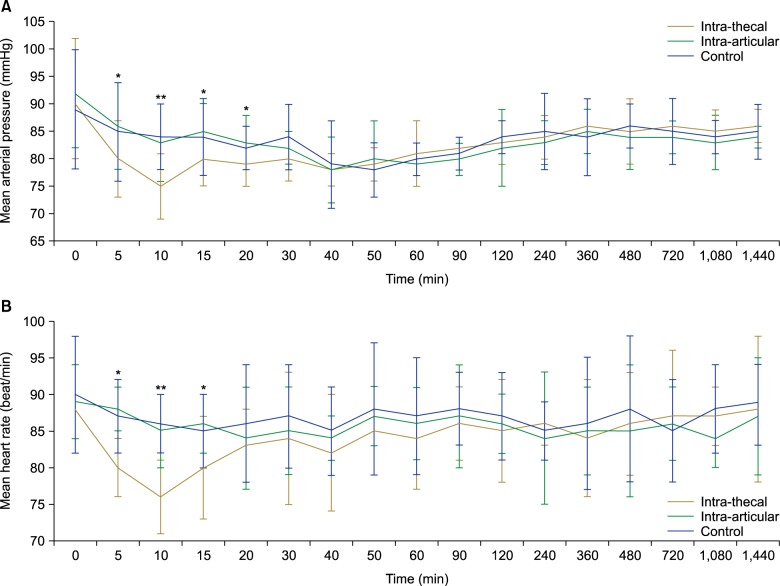
Regarding hemodynamic variables measured during the intraoperative period, the mean arterial blood pressure showed a significant reduction from 5 to 30 m post-intrathecal in the IT group compared to the IA and control groups (Fig. 3A). Also, the heart rate showed significant reduction in the IT group from 5 to 15 min post-intrathecal compared to the IA and control groups (Fig. 3B). After that and during the postoperative period, there were no significant differences among the three groups in mean heart rate or mean arterial blood pressure. In the IT group, two patients received one dose of ephedrine. None of the patients required atropine.
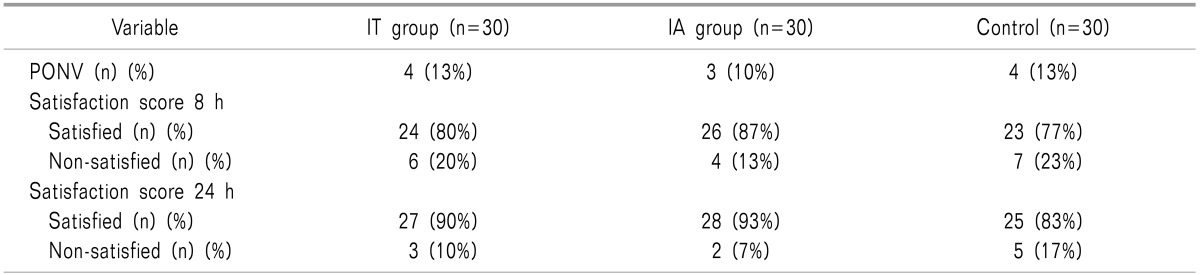
There were no significant differences in the incidence of postoperative nausea and vomiting or patient satisfaction among the three groups (Table 2). Also, the mean sedation score was non-significant among the three groups; all patients were arousable and responsive to commands.
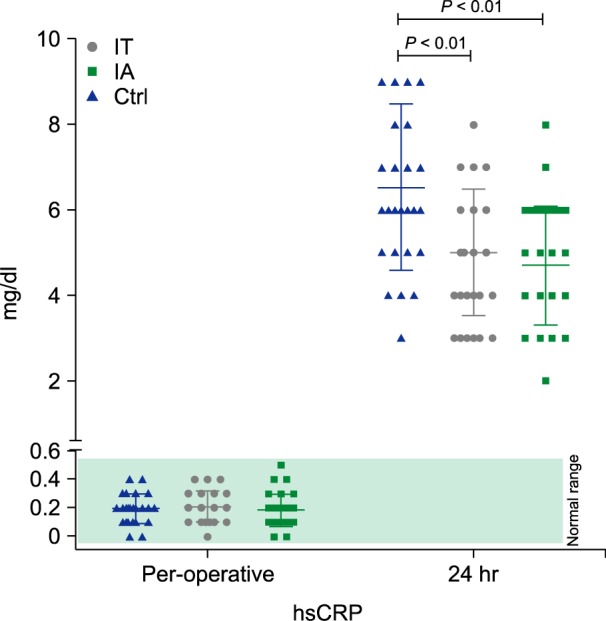
Preoperative CRP level (mg/dl) was non-significant among the patient groups (P > 0.05). At 24 h postoperative, CRP levels significantly increased in the control group compared to the IT and IA groups, with no significant differences between the IT and IA groups (Fig. 4).
DISCUSSION
The present study showed that both intra-thecal and intra-articular administration of dexmedetomidine decreased postoperative pain following arthroscopic knee surgery. Also, they prolonged the time to first analgesic request, and decreased the total dose of analgesic consumption. Our results showed that the VAS scores were lower in both the intrathecal and intra-articular dexmedetomidine groups at 4 h post-intrathecal block compared to control group. Furthermore, the VAS scores were lower in the intra-articular dexmedetomidine group at 6 h post-intrathecal block compared to both the intrathecal dexmedetomidine and control groups.
However, intra-articular dexmedetomidine was superior to the intrathecal route because it caused more prolonged analgesia with less analgesic consumption during the first 24 h.
Dexmedetomidine produces its effect through activation of receptors in the brain, spinal cord, and peripheral nerves. Through inhibition of neuronal firing, it causes analgesia, hypotension, bradycardia, and sedation [618]. It was proved that dexmedetomidine prolonged the duration of the sensory and motor block and the time to the first analgesic request after intrathecal injection without any neurological complications [351920].
The affinity of dexmedetomidine to the α2 adreno-receptors has been reported to be 10 times higher than in clonidine [5]. The action of intrathecal dexmedetomidine is probably similar to intrathecal clonidine: it increases the duration of sensory and motor spinal blocks when added to local anesthetics [321].
In agreement with our finding, intrathecal dexmedetomidine, in a dose of 3-10 µg, prolonged the duration of a bupivacaine block compared to bupivacaine alone without significant side effects [34]. The analgesic action of intrathecal dexmedetomidine may be related to the depression of the release of C-fiber transmitters and hyperpolarization of post-synaptic dorsal horn neurons [22].
The intra-articular route of dexmedetomidine has been found to improve the quality and duration of postoperative analgesia and reduce postoperative analgesic consumption [67]. The mechanism by which intra-articular dexmedetomidine prolongs the duration of postoperative analgesia is not fully understood. It could be attributed to its direct local action on the joint through the poorly vascular intra-articular surface [27]. Others believe that dexmedetomidine may stimulate the release of enkephalin-like substances at peripheral sites [23].
In agreement with earlier reports [524], our findings demonstrated that intra-thecal Dexmedetomidine, in addition to bupivacaine, is associated with a decrease in heart rate and blood pressure compared to the intra-articular and control groups. In contrast, Gupta et al. [25] found that the addition of 5 µg of intrathecal dexmedetomidine to bupivacaine produced intraoperative hemodynamic stability.
The present study showed insignificant differences between the three groups in sedation and satisfaction scores, as well as PONV. In agreement with this finding, Liang et al. [26], in their meta-analysis, found that dexmedetomidine significantly reduced the incidence of PONV after general anesthesia but not regional anesthesia. However, Safari et al. [27] found that IT dexmedetomidine decreased PONV compared to IT fentanyl or bupivacaine.
In this study, there was a significant decrease in CRP in both the intrathecal and intra-articular dexmedetomidine groups compared to the control group at 24 h post-intrathecal block. However, there was no significant difference between the intrathecal and intra-articular dexmedetomidine groups at the same time. CRP was considered a predictor of postoperative complications following knee arthroscopy [28]. No previous reports have studied the effect of intra-articular or intrathecal dexmedetomidine on CRP. However, I.V. dexmedetomidine reduces some of the intraoperative stress response, like plasma cortisone, without affecting the increased postoperative CRP levels [10].
General limitations may apply to our study, such as external validity, multiple centers, and large patient scale. In addition, different intra-thecal and intra-articular dexmedetomidine doses are recommended to find out a minimum safe and effective dose, as well as the determination of the optimal time postoperatively.
While both IT and IA dexmedetomidine provided analgesia for patients undergoing arthroscopic knee surgery, IA was superior to IT based on this study.
 XML Download
XML Download