

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Non-cardiac chest pain (NCCP) is defined as a pain similar to angina that is not accompanied by any symptoms indicative of coronary heart disease [1,2]. It is the second most prevalent trigger for seeking emergency medical services and for hospital visits [3]. This type of pain appears with a variety of symptoms. It may for instance be concentrated in the chest area, or may directly encompass the anterior chest wall. The patient may also feel that the pain is stemming from the chest cavity. NCCP can appear in patterns similar to coronary chest pain, which may last anywhere from a few minutes to a few hours [4]. The lifetime prevalence of NCCP is 33% [5,6], and 43% of the patients undergoing an angiography procedure are not diagnosed with coronary heart disease [7].
Various factors can cause chest pain of non-cardiac origin: the most common include pulmonary disorders, gastrointestinal disorders, musculoskeletal disorders, and arthritis [5,8]. Additionally, NCCP also involves a significant psychological component: in previous studies conducted by experts, 6 to 8% of patients were believed to suffer from a psychological factor, which was presumed to have been left undiagnosed in 83% of cases [4]. There has also been evidence to suggest the existence of a relationship between patients suffering from psychological disorders and patients suffering from NCCP [9,10]. Patients suffering from NCCP face difficulties that may have adverse effects on their professional life, social activities, and personal relationships, causing them fear, anxiety, and stress [11]. Although in these circumstances, the patient's confidence must be boosted in order to prevent intense anxiety and negative protests of his/her illness [12], it has been determined that in most cases, doctors' assurances of a negative result from the heart examination do not cause any relaxation in the patient [13]. Hence, it is necessary to further intervene in the support and completion of doctors' preliminary assurances [14].
A previous study showed that patients suffering from NCCP employed problem-focused strategies, but that their coping style was dry and grid-like in comparison to that of healthy subjects [15]. The majority of these patients believe that their pain has been caused by a heart attack and fear a serious illness, or even death. Therefore, it is clear that despite the diagnosis of NCCP, these patients attribute their pain to the wrong causes [11]. In this regard, Van Peski-Oosterbaan et al. [16] showed that fear springing from bodily sensations was highly linked to excessive obsession with disease, negative automatic thoughts, and tendencies towards disastrous interpretations of bodily sensations in patients suffering from NCCP, and that psychological treatments could help to reduce these problems. In an evaluation of the effect of diaphragmatic breathing on NCCP patients in a three-year follow-up study, DeGuire et al. [17] showed that this treatment was effective in improving the patients' respiratory rate and carbon dioxide levels, and in reducing their pain levels. Achem [18] also mentioned that cognitive therapy could help correct the dysfunctional attitude towards certain traumatic and dangerous physical symptoms (i.e., chest pain) of these patients. However, for the purposes of evaluating the effectiveness of cognitive behavioral therapy, the current study was conducted to compare the relaxation and therapeutic metaphor methods for reducing irrational beliefs and pain severity in patients suffering from non-cardiac chest pain.
MATERIALS AND METHODS
This study was designed as a randomized controlled trial (RCT). The participants were selected among patients who had re-visited the Heart Emergency Section of the Imam Ali Hospital in the city of Kermanshah, Iran, during the summer of 2014 for complaints of pain in the chest area, despite having received a normal coronary angiography procedure. The subjects were randomly assigned to one of the three treatment groups: control, relaxation, and metaphor therapy. The protocol of the study was approved by the Ethics Committee of Kermanshah University of Medical Sciences.
1. Inclusion and exclusion criteria
The inclusion criteria for this study were as follows;
1) Ages between 35 and 75 years old
2) Minimum background of 3 months of prior chest pain
3) Natural and healthy angiography
4) Existence of extreme pain, at a level higher than 2 out of 10 degrees on the pain scale
5) Continued persistent pain for at least one month after the angiography
6) Lack of physical origin for the pain
The exclusion criteria were as follows;
2. Sample and method
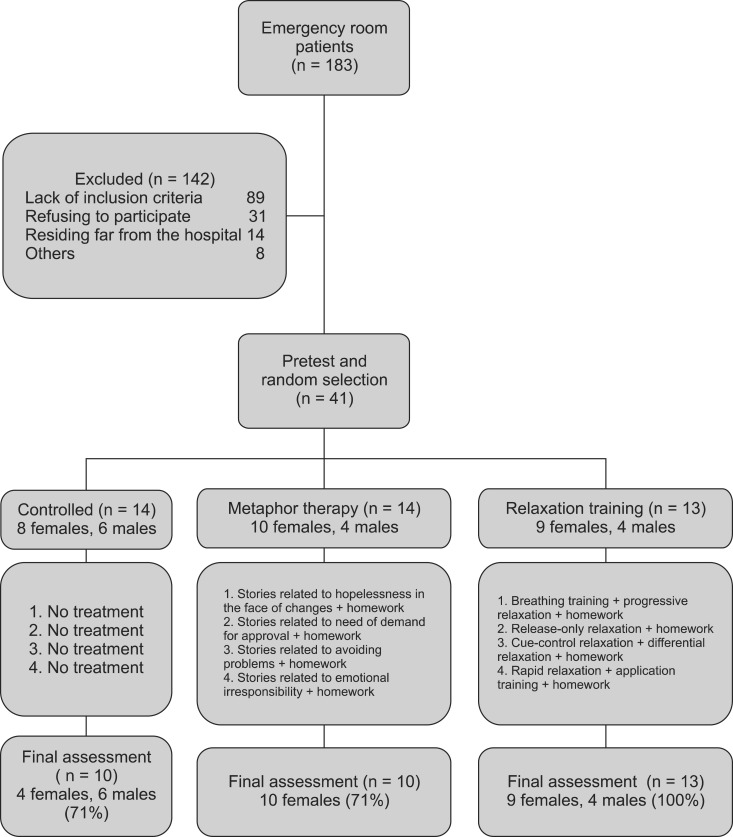
The population of this study consisted in 183 patients who had visited the heart emergency section of the Imam Ali Hospital in the city of Kermanshah, Iran during the summer of 2014 on account of chest pain. Amongst these patients, 142 were deemed ineligible as they did not meet the study's criteria or did not wish to participate in the study. Therefore, 41 patients were retained to participate in the study. After completion of a preliminary interview with a heart surgeon and a clinical psychologist and following the establishment of a medical relationship with the patient, a pretest was conducted in a group format by an impartial psychologist who was not aware of the content of the research. The patients were then placed in one of the three treatment groups: control (14 patients), relaxation training (13 patients), and metaphor therapy (14 patients). The patients in each group participated in weekly intervention sessions conducted over four sessions of two hours each. The clinical psychologists in charge of the program informed the patients of the interventions and relevant training. At the end of each session, forms related to the homework for the session were handed out to the patients, who were asked to complete the forms according to the instructions provided. In the control sessions, only discussions about the physical conditions of the patients and their assessments of future problems were conducted, without any training or medical therapy trends. Finally, one week after the final intervention session, following completion of the test, the data were collected for analysis. During the interventions, 4 patients from the control group and 4 patients from the metaphor therapy group withdrew from the research program (Fig. 1). It should be noted that as a result of concerns for all ethical aspects of the study, after completion of the research and collection of the data from the relaxation therapy group, the results were forwarded to the patients in the control group so that they could benefit from them.
3. Measures
The two tools used in this research were the Brief Pain Inventory (BPI) index for determining the degree of pain and the short version of the Jones Irrational Belief Test. The Brief Pain Inventory categorizes the degree of pain on a 10-point scale, with zero indicating no pain and ten indicating a high degree of pain. This measurement index has been given validity in Iran by Mirzamani et al. [19], and its reliability was reported to be appropriate by the same study. Additionally, the 40 questions included in the irrational belief questionnaire in Iran were composed by Ebadi and Motamedin [20], and were designed and validated based on the original Jones questionnaire. The four subscales included: Hopelessness in the Face of Change (15 items), Need of Demand for Approval (10 items), Problem Avoidance (5 items), and Emotional Irresponsibility (10 items). The scaling of the questions was based on a five-point Likert scale, and the participants rated their degree of agreement or disagreement with each item. In each of the subscales, a higher value showed a higher degree of irrationality. The researchers reported a Cronbach's alpha test of 0.75, and a credibility value by splitting method of 0.76.
4. Treatment protocol
The intervention methods included a relaxation technique based on Öst's treatment, and metaphor therapy. In the relaxation group, the patients were trained in a group format over 4 sessions of 2 hours each, as follows: in the first session, the patients were introduced to the procedures used in Öst's treatment, and were placed in progressive relaxation therapy after receiving diaphragmatic breathing training. At the end of the session, a related homework form was handed out to the patients, and they were asked to complete the exercises on a daily basis, at least twice a day for one week, and to record their relaxation conditions. In the second session, after reviewing the patients' homework, a release-only relaxation technique was taught, and once again the completion and recording of the homework exercises was emphasized. The third session of relaxation therapy training included a cue-control relaxation method and a differential relaxation method, which were taught step by step. In the fourth session, after a review of the homework results from the previous session, a rapid relaxation method was taught with its application to daily real-life situations, while the progression rate of the patients in regard to self-relaxation was simultaneously evaluated.
The metaphor therapy was also completed in 4 sessions of 2 hours each. In the first session, after challenging the patients' beliefs about their current physical condition, two metaphoric stories relating to feelings of hopelessness in the face of changes were presented to the patients, and they were then invited to share their impressions and conclusions from the story. Later, they were asked to draw a connection between this metaphor and their own current conditions. At the end of the session, a homework form was presented to them, and they were asked to mentally rehearse the metaphors on a daily basis, and to write them down and indicate what changes had occurred in their beliefs and behaviors. In the second session, after a review of their previous homework and a discussion of their conclusions, stories about the need of demand for approval from others were presented, and feedback was requested from the patients as for the previous session. Likewise, in the third and fourth sessions, after a review of the homework from the previous sessions, metaphors for problem avoidance and emotional irresponsibility were presented in order to challenge the patients' beliefs. At the end of the last session, it was asked of the patients to always remember the cited metaphors and how they had benefited from the results (Fig. 1).
5. Statistical analysis
The data collected from the 33 samples were analyzed using a multivariate analysis of covariance method (MANCOVA) and a Chi-square test, with the aid of the SPSS (ver. 20.0) statistical software. In addition, the Bonferroni procedure of post-hoc analysis was used to determine the differences between the groups.
RESULTS
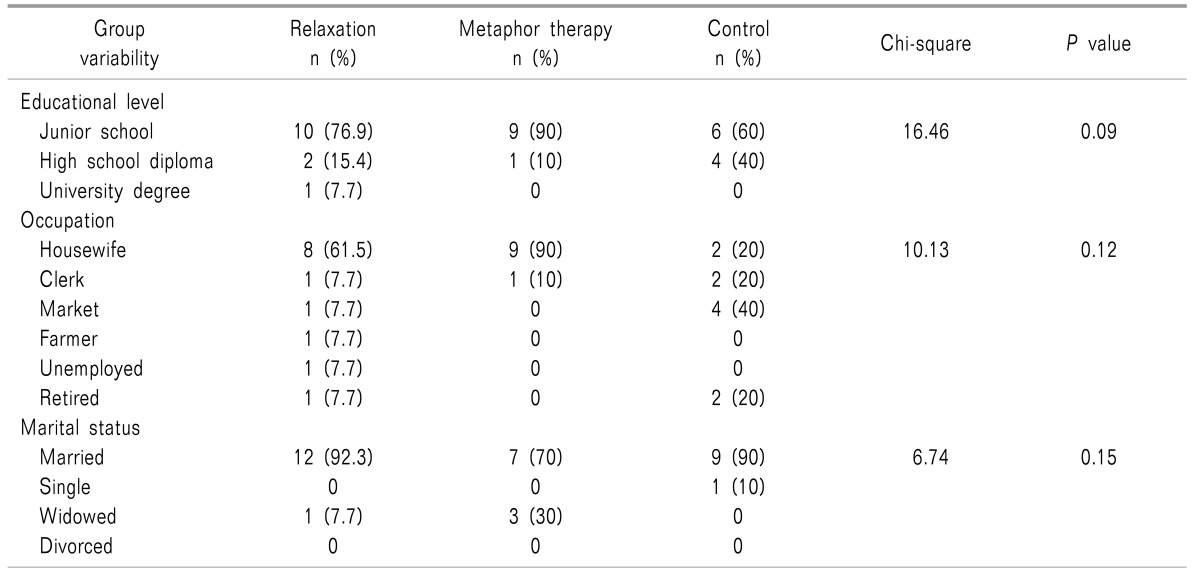
The mean (SD) age of the participants was 52.69 (10.80) in the relaxation group, 48.30 (6.25) in the metaphor therapy group, and 51.80 (10.68) in the control group. In addition, the age range was 41-72 years in the relaxation group, 37-56 in the metaphor therapy group, and 37-74 years in the control group. Table 1 depicts the patients' demographic information.
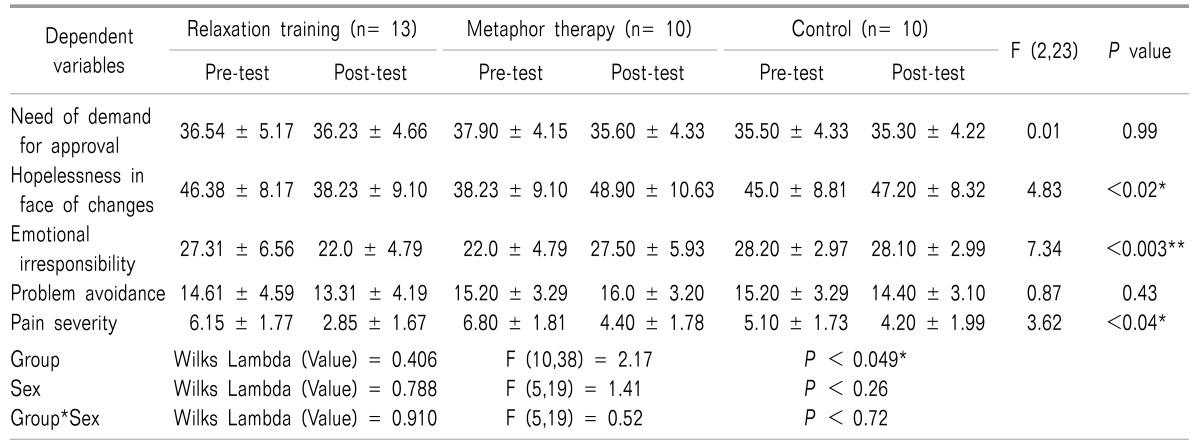
Table 1 shows that there was no significant difference between the groups in terms of educational level, occupation, and marital status. A MANCOVA analysis was used to compare the pre-test and post-test scores for irrational beliefs and pain severity between the three groups. The results are presented in Table 2.
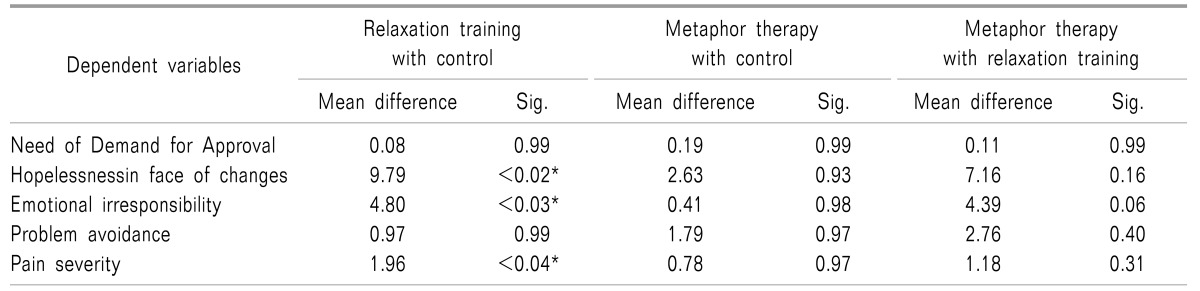
With regard to the calculated F group effect [F (10,38) = 2.17; P < 0.05] it can be stated that there was a significant difference between the groups in at least one of the scores. In order to compare the statuses of the different groups for each item, a Bonferroni post-hoc analysis procedure was used. The results are shown in Table 3. As there was no significant interaction between the gender and the group, it can be inferred that the gender had no effect on the intervention.
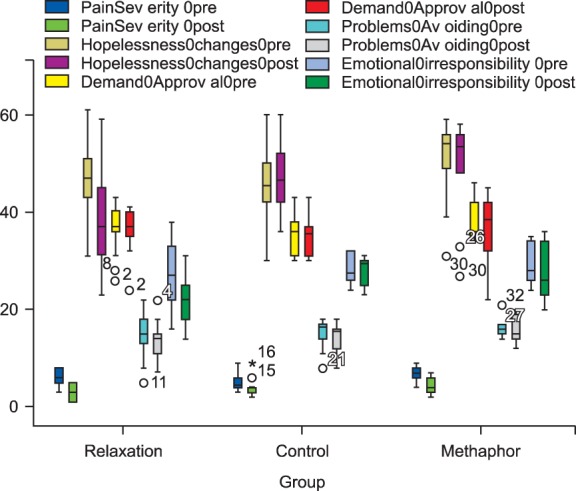
As demonstrated in the table above, there was a significant difference between the relaxation and control groups in the justified means for hopelessness in the face of changes (DM = 9.79, P < 0.05), emotional irresponsibility (DM = 4.80, P < 0.05), and pain severity (DM = 1.96, P < 0.05). In other words, relaxation was effective in decreasing these variables. Conversely, there was no significant difference in the justified means between the metaphor therapy and control groups. In other words, metaphor therapy was not effective for these variables (Fig. 2).
DISCUSSION
The current study was conducted with the aim to compare the effectiveness of relaxation training and metaphor therapy in reducing irrational beliefs and pain severity in patients suffering from non-cardiac chest pain. The results show that relaxation therapy is more effective than metaphor therapy in reducing factors including hopelessness in the face of changes, emotional irresponsibility, and pain severity. Even though these two intervention mechanisms were never directly compared with one another in previous studies, the effectiveness results of relaxation therapy correlate with those of prior studies [21,22,23,24,25]. Using relaxation techniques, patients can have recourse to relaxation as an effective method to create their own feelings of cue control [24]. The emergence of a sense of control over the present situation can challenge the patients' beliefs. Despite the fact that many cases of dysfunctional beliefs in patients suffering from non-cardiac chest pain are reinforced by the emergence of pain, and despite the medical reassurance that their recovery process can be affected by such thinking, relaxation therapy can counter the physiological effects of anxiety, including acting on bradycardia and increasing the peripheral blood flow and neuromuscular stability [24]. Through the practice of relaxation exercises, patients' disappointment and frustration with their sense of control over their physical and mental symptoms will be reduced, allowing them to eventually develop a sense of responsibility for their own recovery. It is therefore expected that relaxation therapy can help reduce not only the signs of pain, but also the irrational beliefs of the patients. In particular, it can affect their hopelessness in the face of changes and their sense of emotional responsibility.
On the other hand, in accordance with the research conducted by Esler and Bock [26], the results of the current study show that metaphor therapy has had a significant impact as a recognized therapy for reducing the irrational beliefs and perceived pain of patients who do not suffer from non-cardiac chest pain. It is apparent that the goal of therapy for patients with non-cardiac chest pain is to correct their dysfunctional attitudes, particularly towards traumatic and dangerous physical symptoms, (i.e., chest pain), and to reduce their concerns [18]. This study attempted to accomplish this task by providing metaphors and local stories related to the patients' irrational beliefs. With knowledge that the use of metaphor rather than direct suggestions of treatment can weaken defense mechanisms against any functional changes and cause an increase in the effectiveness of therapeutic interventions [27,28,29], patients without a certain defensive mechanism usually pay more attention to the more obvious symptoms of chest pain and find it difficult to separate the true or false nature of it, being of the belief that it is necessary to control the matter either with medication or by acquiring an objective method of application. Considering these circumstances and following the lack of response to prior conventional drug therapies, the problems can become chronic and, in the event of a lack of response to their unanswerable questions regarding the reasons for their pain by the treating physicians, it is expected that the patients will seek more obvious and quicker remedies to significantly reduce their pain. Metaphor therapy apparently does not comply with these expectations, and the patients feel that nothing has changed in comparison with past states. Meanwhile, the patients in the relaxation group acknowledged that they had learned a technique, and that they could reduce their pain symptoms by utilizing this technique on a daily basis.
Another explanation for the lack of effectiveness of metaphor treatment may lie in the patients themselves, as the extension of metaphors is largely due to the willingness and ability of the patients to use their own power of imagination and visualization [30]. Therefore, the question arises of how the patients can visualize the messages in the stories despite their current level of pain and according to the non-cardiac justifications for their physical, cognitive, and behavioral irrational beliefs, so that they and challenge their catastrophic interpretations of their symptoms and recognize them as being dependent on themselves.
It is noteworthy to mention that given the limitations of the statistical population and research samples in this study, as well as the fact that the patients were aged between 35 and 75 years old, creating heterogeneity in the course of the sessions became problematic. It is recommended that larger samples with more limited age ranges be used in follow-up research.
Finally, the results of this research show that relaxation training was significantly more effective than metaphor therapy and the lack of treatment in reducing irrational beliefs about "Hopelessness in the Face of Changes", "Emotional Irresponsibility", and the "Severity of Pain" in patients suffering from non-cardiac chest pain. However, none of the treatment therapies were effective in reducing the beliefs related to the "Need of Demand for Approval" and "Problem Avoidance." Given that the relaxation method can help transfer the feelings of control over symptoms to the patients by inducing relaxation, it is suggested that this method of treatment be set as a priority for this type of patients. Additionally, given the ineffectiveness of the metaphor therapy method in reducing the symptoms of these patients, further related studies should be conducted in this area.
 XML Download
XML Download