

 PDF
PDF Citation
Citation Print
Print


Discal cyst is an intraspinal cyst with a distinct communication with the corresponding intervertebral disc [1]. It is a rare condition and could present with radiculopathy similar to that caused by lumbar disc herniation. Usual treatments for discal cysts include surgical removal of the cyst [1-4] and, percutaneous computed tomography (CT)-guided aspiration of the cyst and steroid injection [5].
We experienced a case of leg pain due to lumbar discal cyst, and we alleviated the radiating pain with selective transforaminal epidural blocks.
CASE REPORTS
A 74-year-old female patient visited our department due to pain in the left lower limbs for 6 months. Her past medical history was unremarkable.
The patient complained of a continuous dull pain along the left 5th lumbar vertebral (L5) and 1st sacral vertebral (S1) dermatomes. The pain level was 9 on the numeric rating scale (NRS) from 0 (no pain) to 10 (worst pain imaginable). The pain was exacerbated by walking and was alleviated by sitting or lying in bed. The patient was unable to walk more than 20 m due to pain.
Physical examination revealed sensory loss of 50% along the left L5 and S1 dermatomes without weakness. On deep tendon reflex (DTR) testing, the knee jerk and ankle jerk were normal. The straight leg raise test showed a positive result at 45° in the left lower limb. The pulsation of the dorsalis pedis artery was normal.
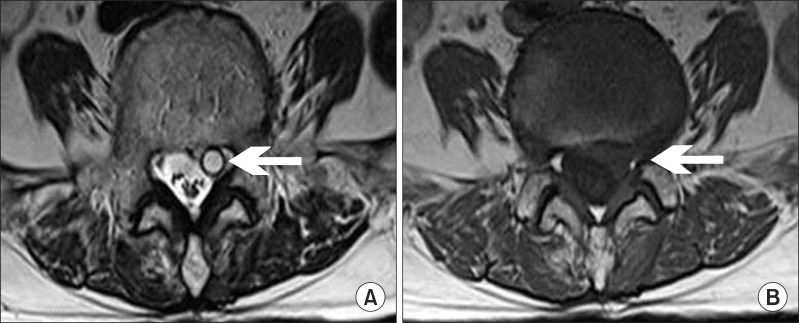
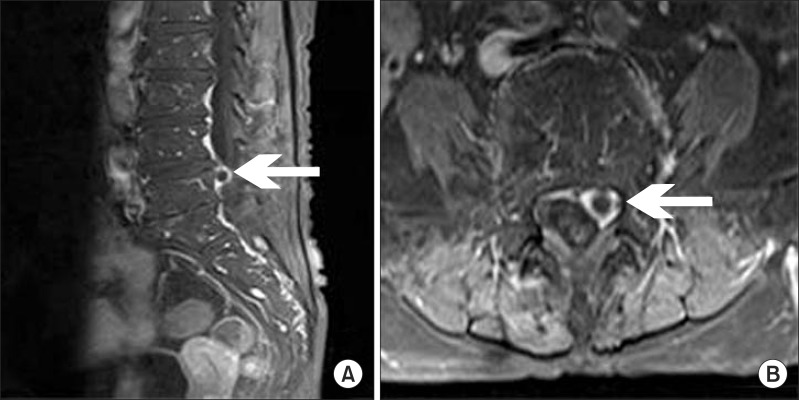
Magnetic resonance imaging (MRI) of the lumbar spine showed a large cyst in the ventrolateral epidural space of the L5 level that communicated with the adjacent 4th lumbar and 5th lumbar intervertebral disc (Fig. 1). The cyst showed high signal intensity on T2-weighted images and low signal intensity on T1-weighted images (Fig. 2). After addition of contrast, the cystic mass had a thick wall with rim enhancement (Fig. 3). The patient was diagnosed with radiculopathy due to a discal cyst. Left L5 and S1 selective transforaminal epidural blocks were performed using 20 mg triamcinolone and 2 ml of 0.3% mepivacaine for the left lower limb radiating pain. Pregabalin 150 mg, tramadol 50 mg, and a muscle relaxant were administered daily for 2 weeks. Two weeks later, the patient's left lower limb radiating pain had been somewhat alleviated, as judged by the decrease in the pain score on the numeric rating scale (NRS) to 6 following the treatment. L5 and S1 transforaminal epidural blocks were then repeated using 40 mg triamcinolone and 2 ml of 0.3% mepivacaine. Pregabalin 300 mg and tramadol 100 mg were administered daily for 4 weeks. One month after the 2nd procedure, the left lower limb radiating pain was rated a 5 by the patient on the NRS. Therefore, we once again repeated the L5 and S1 transforaminal epidural blocks using 40 mg triamcinolone and 2 ml of 0.3% mepivacaine, and the same medications were prescribed. Two months after the 3rd transforaminal epidural blocks, the patient's leg pain was rated a 2 on the NRS, although the hypesthesia persisted.
DISCUSSION
Discal cyst was first reported in 2001 by Chiba et al. [1]. The pathogenesis of discal cyst is currently unknown. However, it has been suggested that discal cyst results from focal degeneration of the intervertebral disc with fluid production [6], and that discal cyst develops through deficits in hematoma resorption [1].
The clinical presentation of discal cyst is unilateral radiculopathy similar to that caused by intervertebral disc herniation. It is difficult to differentiate between discal cyst and intervertebral disc herniation through history taking and physical examination of patients [1].
MRI is the most sensitive imaging modality in the diagnosis of a discal cyst. The typical finding for a discal cyst is a round to oval extradural mass lesion with high signal intensity on T2-weighted images and low signal intensity on T1-weighted images. After addition of gadolinium medium, the surrounding rim of the cyst is enhanced [7]. In the present case, all of these characteristics were observed on MRI. A connection between the cyst and the corresponding disc is the key to differentiate discal cysts from intervertebral disc herniation [8]. In the present case, the cyst was observed to communicate with the adjacent 4th lumbar and 5th lumbar intervertebral disc.
Surgical removal of the cyst [1-4] and CT-guided aspiration of the cyst with steroid injection [5] are believed to be effective treatment options for discal cyst. However, Chou et al. [9] and Prasad et al. [10] report the regression of a discal cyst with epidural blocks without surgery or aspiration. In addition, Demaerel et al. [8] and Takeshima et al. [11] report cases of spontaneous regression of a discal cyst without intervention. At this point, the natural history of discal cysts is still unknown [4], and further evaluation is needed.
I felt that radiculopathy due to discal cyst could be treated similarly to HNP (herniated nucleus pulposus), and conservative treatment such as transforaminal epidural block should be the first choice. If transforaminal epidural block is unsuccessful in reducing radiating pain, surgery or CT-guided aspiration of the cyst with steroid injection should be considered. Therefore, I performed several left L5 and S1 transforaminal epidural blocks to relieve the radiating pain. Following those procedures, the patient's radiating pain was reduced sufficiently.
The patient refused to undergo follow-up MRI due to her symptomatic improvement and the financial burden. Therefore, I were unable to determine whether the discal cyst regressed spontaneously as in previous cases [8-11], or whether the discal cyst persisted but the radiating pain was relieved by the transforaminal epidural blocks.
In conclusion, radiculopathy caused by intervertebral discal cyst is a very rare condition. If patients complain of radiating pain, the possibility of a discal cyst cannot be excluded. For the treatment of discal cyst, various treatment options are available. However, transforaminal epidural blocks can also be a good treatment option.

 XML Download
XML Download