

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Neuropathic pain can be defined as pain caused or initiated by a primary lesion of the peripheral or central nervous system, manifesting with sensory symptoms and signs [1]. It is associated with allodynia, hyperalgesia and spontaneous pain with varying intensity, in which pain could be so severe that daily activities like wearing clothes might be difficult. Neuropathic pain can also decrease quality of life, cause patients to withdraw socially and emotionally, and cause problems with mood and sleep. Moreover, unrelieved pain inhibits respiration, decreases mobility, and decreases patient functional status, which may lead to iatrogenic events, including pneumonia, constipation, and deep vein thrombosis [2].
Medications primarily used for neuropathic pain generally fall into the categories of anticonvulsants, antidepressants, opioids, and topical agents. The current treatment options, however, are not effective enough to make the pain endurable and the response rate has been estimated at a 30% to 50% reduction in pain in up to 50% of patients [3].
Recently, accumulating evidence has demonstrated that both microglia and astrocytes release a variety of proinflammatory cytokines including interleukin (IL)-1β, IL-6, and tumor necrosis factor (TNF-α), which play a major role in mediating and/or maintaining hyperalgesia and allodynia in inflammatory, as well as neuropathic pain [4-6].
Thalidomide, a derivative of glutamic acid, was developed initially as a sedative and used for morning sickness until 1961 when its use was banned due to its association with major birth defects. It reappeared in clinical practice because of its immunomodulatory properties. Furthermore, investigations into the mechanisms underlying thalidomide's pharmacotherapeutic action have increased [7,8], with its effects on the production and release of TNF-α being of notable importance. Thalidomide has been used in several cutaneous inflammatory disorders (erythema nodosum leprosum in lepromatous leprosy, cutaneous lupus erythematosus, severe aphtosis), cancers (relapsed/refractory multiple myeloma) and inflammatory conditions [9]. Previous studies have shown that thalidomide inhibits the inflammatory hyperalgesia in rats and the writhing nociceptive response in mice [10,11]. Thalidomide was found to be effective in animal models of neuropathic pain, such as chronic sciatic nerve injury (CCI) and Lumbar (L) 5 ventral root transection (VRT) neuropathy [12,13]; however, several human case reports and series have demonstrated mixed results, with some patients having dramatic responses, especially in chronic intractable conditions such as complex regional pain syndrome [14,15].
Opioids are among the most powerful analgesics in clinical use for the treatment of nociceptive pain, but data concerning their effectiveness in neuropathic pain has been controversial [16,17]. However, evidence now suggests that opioids are effective in relieving some pain symptoms in patients with neuropathic pain of primarily peripheral origin [18,19].
In the present study, we investigated the antiallodynic effects of morphine and thalidomide in a spinal nerve ligation rat model.
MATERIALS AND METHODS
1. Animal preparation
All experiments followed the Guidelines on Ethical Standards for Investigation of Experimental Pain in Animals [20]. Male Sprague-Dawley rats weighing 100-120 g were used in all experiments. Animals were acclimated to the laboratory environment for 5-7 days before being used in the study. While in the home cage environment, animals were fed a standard rat diet and tap water. Room temperature was maintained at 20-23℃ with a 12:12 h light/dark cycle.
2. Animal model of neuropathic pain
Neuropathic pain was evoked by spinal nerve ligation of experimental rats, as previously described [21]. Briefly, the left L5 and L6 spinal nerves of rats were isolated adjacent to the vertebral column during sevoflurane anesthesia and tightly ligated with a 6-0 silk suture distal to the dorsal root ganglia. Care was taken to avoid injury of the L4 spinal nerve. Animals were considered to be in neuropathic pain when they exhibited mechanical allodynia i.e., paw flinching behavior response to the application of a bending force of less than 4 g. Sham rats underwent identical surgical procedures at the same level, but the spinal nerves were not ligated. Rats showing motor impairment after surgery were killed immediately using overdose of sevoflurane.
3. Drugs
The following drugs were used in this study: thalidomide (Sigma Chemical Co., St. Louis, MO, USA) and morphine sulfate (Sigma Aldrich Co., St. Louis, MO, USA). Thalidomide was dissolved in dimethyl sulfoxide (DMSO), and the solution was then diluted with saline to reduce the concentration of DMSO to 10%. Morphine was dissolved in normal saline. Both agents were intraperitoneally administered. The dose of thalidomide and morphine were decided based on previous studies using neuropathic pain models.
4. Assessment of mechanical allodynia
Paw withdrawal threshold (PWT) in response to mechanical stimulation was measured using the up and down method [22] by applying calibrated von Frey filaments (Stoelting, Wood Dale, IL, USA) from underneath the cage through openings in the mesh floor to the hindpaw. Rats were placed in a separate transparent plexus-glass chamber with a wire mesh floor underneath and acclimated to the test chambers for 30 min. A series of eight von Frey filaments (0.4, 0.7, 1.2, 2.0, 3.6, 5.5, 8.5 and 15 g) were applied vertically to the plantar surface of the hindpaw for 5 s while the hair was bent. Brisk withdrawal or paw flinching was considered as positive responses. If rat showed the positive response the less stiff filament was used for the next trial, or the stiffer one for the case with no withdrawal or licking. The cut-off value was determined as 15 g, where the PWT was 15 g if the rat did not show any withdrawal or licking response to the application of a 15 g von Frey filament. Rats which did not show allodynia (less than 4 g) were excluded from this study.
5. Experimental paradigm
On the day of testing (day 10 after spinal nerve ligation), rats were allowed to acclimate to the testing chamber for 30 min then allocated into experimental and control groups for the tested drugs. Control studies were performed using intraperitoneal saline or DMSO according to the solvent used for the tested drug. Animals were tested only once in this study, and the investigator was blind to the drug given. The effects of thalidomide (6.25, 12.5, 25, and 50 mg/kg) and morphine (3 and 10 mg/kg) were investigated in the neuropathic pain state, and withdrawal threshold was determined at 30 minutes after intraperitoneal administration of experimental drugs.
6. General behavior
For the purpose of examining motor impairment by thalidomide and morphine, the highest dose of each drug used was given intraperitoneally to 10 additional rats. Motor function was assessed by the righting reflex and placing-stepping reflex. The former was evaluated by placing the rat horizontally with its back on the table, which normally gives rise to an immediate coordinated twisting of the body to an upright position. The latter was evoked by drawing the dorsum of either hind paw across the edge of the table. Normally rats try to put the paw ahead into a position to walk. Pinna reflex and corneal reflex were also evaluated and judged as present or absent.
7. Statistical analysis
Data are expressed as mean ± SEM. Time response data are presented as paw withdrawal threshold to mechanical stimulation, while dose-response data are presented as the percent of maximum possible effect (%MPE). Withdrawal threshold data from von Frey filament testing were converted to %MPE, according to the formula: %MPE = [(postdrug threshold - post-injured baseline threshold) / (cutoff threshold - post-injured baseline threshold)] × 100. To analyze the 50% probability PWT data and dose-responsiveness, one-way analysis of variance (ANOVA) with Scheffe multiple comparison test was used. P values of < 0.05 were considered statistically significant.
RESULTS
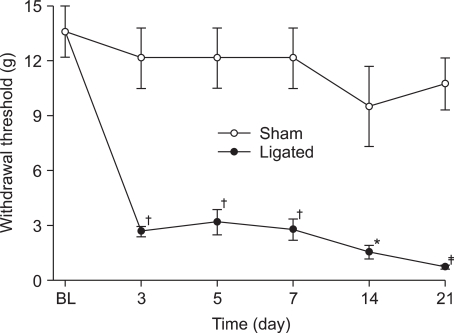
1. Time course for development of mechanical allodynia in spinal nerve-ligated rats
Before spinal nerve ligation, PWTs ranged from 12 g to 14 g. After L5, 6 spinal nerve ligation, withdrawal threshold of the nerve-ligated group was significantly reduced in comparison with that of the sham-ligated group, and this reduced threshold persisted for 21 days. Withdrawal threshold of the sham group did not change during the observation period (Fig. 1).
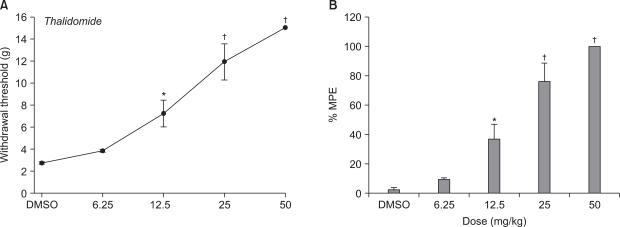
2. Effect of intraperitoneal thalidomide on mechanical withdrawal thresholds
Thalidomide significantly increased PWT compared to controls (Fig. 2A), and produced dose-responsiveness (Fig. 2B). The lower dose of thalidomide (6.25 mg/kg) produced no significant reversal of the tactile allodynia, however the higher dose of thalidomide (12.5, 25 and 50 mg/kg, respectively) effectively increased mechanical withdrawal threshold compared to vehicle.
DISCUSSION
Neuropathic pain encompasses a myriad of painful disease states that are often hard to treat, especially with one single medication. There is no "gold standard" in regard to one medication for neuropathic pain. Some new medications have emerged during the past few years that help to augment the armamentarium of medications used in neuropathic pain [3]. Recently, increasing evidence indicates that glial cells, one of non-neuronal cells, also play an important role in the pathogenesis of neuropathic pain and the mechanism of neuropathic pain by nerve injury. Neuropathic pain is newly regarded as complex and integral in the interaction of neuronal and non-neuronal cells [4-6]. Not only neurotransmitters from neurons at the synapses, but also many cytokines released from glial cells are involved in the development of hyperalgesia and allodynia in inflammatory as well as neuropathic pain. In addition, much research indicates that proinflammatory cytokines such as TNF-α, IL-1β and IL-6 are major elements contributing to development and maintenance of the pathological state of pain [6,23]; consequently, they have been proposed as therapeutic targets [24].
Thalidomide has profound immunomodulatory actions in addition to its originally intended pharmacological actions. Thalidomide is currently approved by the US Food and Drug Administration in conjunction with dexamethasone in newly diagnosed multiple myeloma, and in the acute treatment of cutaneous manifestations of erythema nodosum leprosum, as well as in maintenance therapy for its prevention and suppression.
In the present study, intraperitoneal thalidomide significantly increased PWT compared to control and produced dose-responsiveness. The lower dose of thalidomide (6.25 mg/kg) produced no significant reversal of tactile allodynia, but the higher dose of thalidomide (12.5, 25 and 50 mg/kg, respectively) effectively increased mechanical withdrawal threshold compared to vehicle.
Although thalidomide and its analogues have broad-spectrum properties, their major mode of action is the inhibition of TNF-α synthesis. Thalidomide reduces synthesis of TNF-α in cultures of lipopolysaccharide-stimulated human microglial cells [25], and also modulates TNF-α production by several mechanisms, for example, by enhancing TNF-α mRNA degradation [26] or by binding to a1-acid glycoprotein [27]. Thalidomide was also found to be effective in animal models by inhibiting TNF-alpha production [10-13]. Previous studies have shown that thalidomide inhibits inflammatory hyperalgesia in rats and the writhing nociceptive response in mice as a possible consequence of inhibition of TNF-α production [10,11]. It has also been reported that thalidomide reversed and prevented the hyperalgesia by inhibiting TNF-α production in chronic sciatic nerve injury and L5 VRT neuropathy, respectively [12,13]. However, in other studies [13,28], thalidomide was only effective when given preemptively, i.e., before manifestation of the pain related symptom. However, in our study intraperitoneal injection of thalidomide effectively attenuated mechanical allodynia when it was applied at day 10 after surgery. This discrepancy may be related to different animal models and experimental methods. Also, it has also been reported that when applied 7 days after surgery thalidomide was still capable of inhibiting upregulation of TNF-α in L5 VRT neuropathy [13]. Thus, it is most likely that the antinociceptive effect of thalidomide in this present study comes from the interruption of TNF-α production. The pharmacological properties of thalidomide aside from their immunomodulatory capacity could also explain the effects observed in our study. The sedative-hypnotic effect of thalidomide was suggested as mediated via interruption or modulation of serotonin's actions within the CNS. However, rats injected with thalidomide did not show any sedative state at the dose of maximum analgesic effect during the behavioral test.
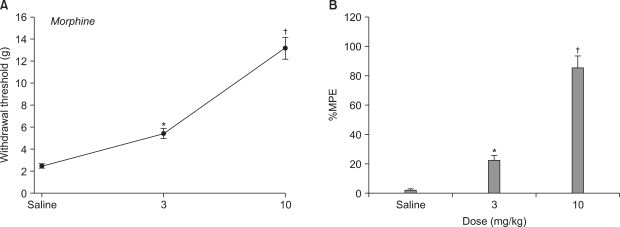
Various studies have reported reduced antinociceptive efficacy of morphine in animal models of peripheral or central nerve injury. However, conflicting results regarding the efficacy of opioids on neuropathic pain in different neuropathic animal models have been reported. While systemic administration of morphine attenuates allodynia and hyperalgesia in chronic constriction injury and spinal nerve ligation (SNL) models [29,30], intrathecal morphine is apparently ineffective [29,31]. In contrast, intrathecal morphine dose-dependently reversed mechanical allodynia in a rat model of central pain, whereas systemic morphine had little effect on this measure [32]. Recently, these findings have been challenged by Zhao et al. [33] who reported antiallodynic effects of both systemic and intrathecally administered morphine in the SNI, SNL and SCI animal models of neuropathic pain. These results indicate the efficacy of opioids in neuropathic pain is variable and seems to depend on several factors (e.g., the kind of nerve injury and the route of drug administration). In this study, the 3 and 10 mg/kg doses of systemic morphine significantly increased PWT compared to vehicle. Our study indicates that systemic morphine produces antiallodynic effects in SNL rats, which is consistent with previous reports [30,33]. Our results further support the efficacy of opioid receptor agonists in alleviating signs of neuropathic pain in animal models of peripheral nerve injury.
In this present study, intraperitoneal thalidomide and morphine significantly increased PWT compared to control and produced dose-responsiveness. However, similar studies on various animals are required to obtain a reliable oversight of the effect of thalidomide on peripheral and central nerve injury-induced neuropathic pain in a clinical setting.
In conclusion, systemic morphine and thalidomide have antiallodynic effects on neuropathic pain induced by SNL in rats. These results suggest that morphine and thalidomide may be an alternative therapeutic approach for neuropathic pain.
 XML Download
XML Download