

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Severe Clostridium difficile infections (CDIs) associated with an emerging epidemic strain, PCR-ribotype 027, have increased in frequency and severity in the U.S., Canada, and the European countries since 2003 [1]. However, reports of ribotype 027 infections in East Asian countries remain rare [2]. One case each was reported from Japan [3] and Korea [4] in 2007 and 2009, respectively. A one-year surveillance study between 2007 and 2008 in Shanghai, China failed to detect any cases, although one case was reported in Hong Kong in 2009 [2]. These results may indicate the onset of spreading ribotype 027 infection in Asian countries.
Ribotype 027 strain had toxin A, toxin B and binary toxin with deletion of toxin regulator gene (tcdC) [1]. According to a previous study, the use of moxifloxacin is associated with ribotype 027 outbreaks, and the isolates obtained in that study were resistant to levofloxacin and moxifloxacin [5]. A Korean isolate was resistant, whereas 1 Japanese isolate was susceptible to moxifloxacin [3, 4]; this indicated a need for further testing of Korean isolates.
The aims of this study were to determine the prevalence of ribotype 027 among the stored C. difficile isolates, to characterize the ribotype 027 isolates, and to evaluate the clinical severity of CDI in patients infected with these strains.
MATERIALS AND METHODS
1. Bacterial isolates and antimicrobial susceptibility testing
A total of 1,251 C. difficile isolates were recovered from stool specimens of suspected CDI patients at two tertiary-care hospitals and one commercial laboratory between 2002 and 2009. The commercial laboratory processed the stool specimens collected from hospitals and clinics without in-house anaerobic microbiological testing facilities. C. difficile selective agar (CDSA; Becton, Dickinson and Company, Franklin Lakes, NJ, USA) was used to isolate C. difficile under anaerobic incubation. The isolates were identified using conventional tests and the ATB 32A system (bioMerieux, Marcy l'Etoile, France). Minimum inhibitory concentrations (MICs) of moxifloxacin for ribotype 027 isolates were determined using Etest strips (AB bioMérieux, Solna, Sweden).
2. Clinical characteristics of patients
We reviewed the patients' medical records, and according to the criteria proposed by Zar et al. [6], patients with ≥2 points were considered to have severe CDI. One point was given for each of the following criteria: age >60 yr, body temperature >38.3℃, serum albumin <2.5 mg/dL, and peripheral white blood cell count >15,000/µL. Two points were given if there was endoscopic evidence of pseudomembranous colitis (PMC) or if the patient was admitted to the intensive care unit.
3. PCR assay for toxin genes
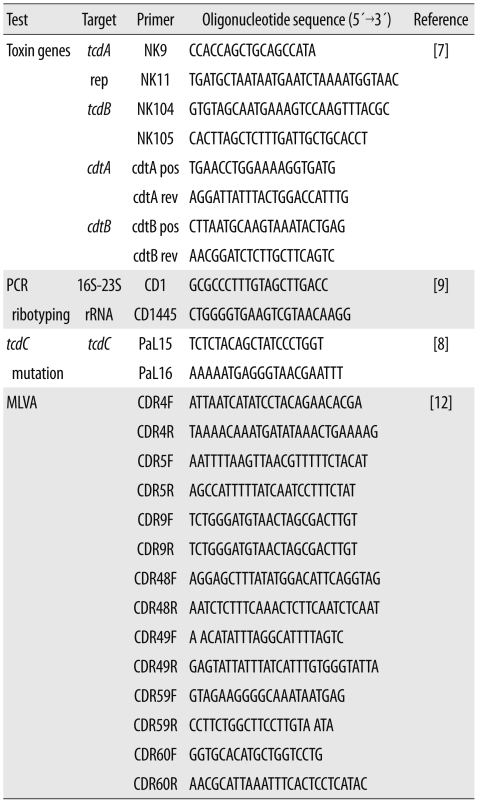
C. difficile toxin genes were detected by performing PCR as described in previous studies [7, 8]. Primer sequences used in this study are listed in Table 1. C. difficile VPI 10463 (A+ B+, CDT-), 3608/03 (A-B-, CDT-), SE844 (A+B+, CDT+), and 1470 (A-B+, CDT-) were used as controls for the PCR assays. The obtained amplicons were commercially sequenced (Macrogen, Seoul, Korea). The deduced amino acid sequences were compared to those of the strain VPI 10463.
4. PCR-ribotyping
PCR-ribotyping was performed according to a previously described method [9] with minor modification. We added 10 µL of crude nucleic acid as template to a 50-µL PCR mix-ture containing 10 mM Tris-HCl (pH 8.3) and 50 mM KCl (GeneAmp 1×PCR Buffer II; Applied Biosystems, Foster City, CA, USA), 4.0 mM MgCl2, 0.4 mM dNTP, 1.5 U Taq DNA polymerase (AmpliTaq Gold, Applied Biosystems), and 0.4 µM primers (CD1 and CD1445).
5. Pulsed-field gel electrophoresis and multilocus variable-number tandem-repeat analysis typing
Pulsed-field gel electrophoresis (PFGE) analysis was performed by modified method of Alonso et al. [10]. In brief, we prepared plugs of chromosomal DNA from fresh colonies cultured for 24 hr and treated them with high concentration of proteinase K (75 U/mL). Thiourea was added to the gel and running buffer used for PFGE [11].
Multilocus variable-number tandem-repeat analysis (ML-VA) was performed by PCR amplification and sequence analysis of 7 selected C. difficile repeat (CDR) loci; CDR4, CDR5, CDR9, CDR48, CDR49, CDR59, and CDR60. The primer sets used are listed in Table 1 [12]. The copy numbers of each of the 7 CDR loci were concatenated to generate an MLVA type for each isolate.
RESULTS
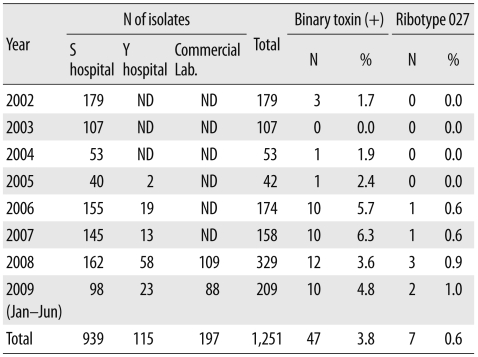
Of the 1,251 C. difficile isolates, 47 (3.8%) were PCR positive for the toxin A, toxin B, and binary toxin genes, and 7 (0.6%) were identified as ribotype 027 by PCR-ribotyping. The first isolate to be identified as ribotype 027 was from a sample obtained in 2006, and the prevalence of ribotype 027 was 0.6% in 2006 and 2007, 0.9% in 2008, and 1.0% in 2009 (Table 2).
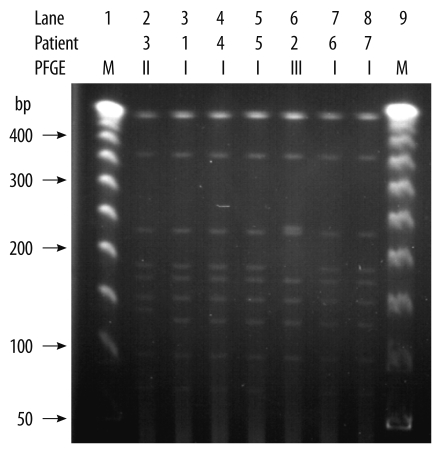
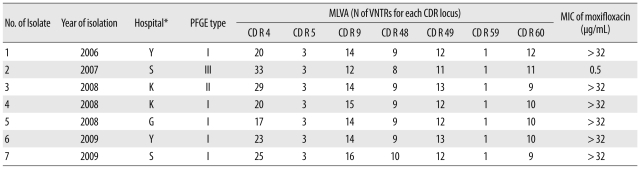
All the ribotype 027 isolates had an 18-bp deletion from position 330 to 347 and a 1-bp deletion at position 117 in the tcdC gene sequence. We observed identical PFGE patterns for 5 isolates (isolates 1, 4, 5, 6, and 7). However, the patterns for isolates 2 and 3 differed from those of the other isolates in 3 and 2 bands, respectively (Table 3, Fig. 1).
All the 7 isolates had different MLVA types. However, all the isolates had the same number of variable number tandem repeats (VNTRs) at the CDR5 and CDR59 loci (Table 3).
The MIC of moxifloxacin was >32 µg/mL for 6 of the 7 isolates and 0.5 µg/mL for the remaining 1 isolate (isolate 2).
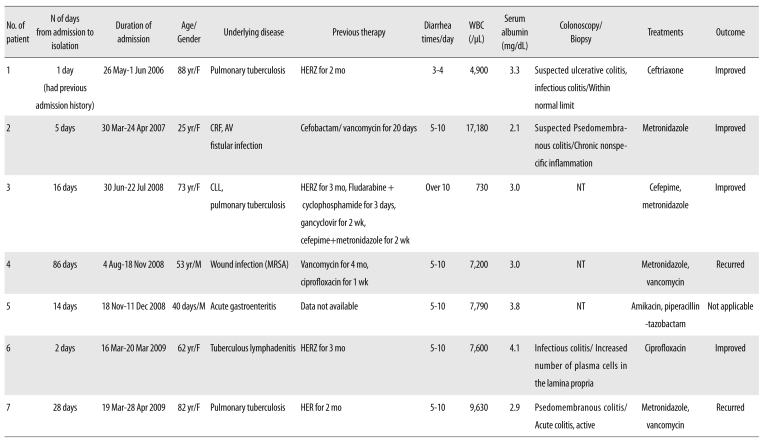
Brief histories of patients infected with ribotype 027 are summarized in Table 4. The ages of the 7 patients (2 men and 5 women) were in the range of 25 to 88 yr, except a clinically-irrelevant 40-day-old infant with acute gastroenteritis.
All patients had been hospitalized for some underlying diseases. Four patients had received anti-tuberculous medication 2-4 weeks before hospitalization. None of the patients had travelled overseas. Symptoms and their severity varied among the patients, ranging from mild colitis to severe PMC. Except for patient 2, none of the patients showed high fever (>38.0℃), increased leukocyte count (>15,000/µL), increased serum creatinine (>2.0 mg/dL), or decreased serum albumin (<2.5 mg/dL). Patient 2 showed high leukocyte count and serum creatinine level due to underlying chronic renal failure and an arteriovenous fistula infection.
Two (patient nos. 2 and 7) cases were diagnosed with suspected PMC and PMC by colonoscopic biopsy and considered probably severe (patient no. 2) or severe (patient no. 7) according to the criteria proposed by Zar FA et al. [6].
Metronidazole was administered to 4 patients (patient nos. 2, 3, 4, and 7) to treat CDI. Because of poor response, for patients 4 and 7, the regimen was changed to vancomycin, but the infection recurred. Two patients (patient nos. 1 and 6) recovered without CDI treatment.
DISCUSSION
Although the first case of ribotype 027 infection in Korea was reported in 2009 [4], we found that ribotype 027 was present in Korea as early as 2006. Since 2006, the prevalence of ribotype 027 isolates has been 0.8% (7/870). Except for patient no. 6, all the patients had most likely acquired the infection in a hospital. We recovered these isolates from 7 patients who had visited 4 different hospitals located in Seoul and Gyeonggi province; this indicated an early stage of dissemination to Korean hospitals. Two of these hospitals sent the samples to a commercial laboratory for culturing C. difficile, and the samples were redirected to the S hospital in Seoul where the tests were performed. The presence of ribotype 027 in an infant was clinically irrelevant; however, this finding suggested that the isolate was easily transmissible.
Severe diseases are more likely to be caused by ribotype 027 strains than by non-027 strains, because the ribotype 027 strains produces excessive amounts of toxins A and B as a result of tcdC deletion [5]. There is no consensus about the definition of severe CDI. However, as per the criteria proposed by Zar et al. [6], 2 of the 7 cases in this study, like the first case reported in Korea [4], were either probably severe (case no. 2) or severe (case no. 7). In North America, patients infected with the ribotype 027 isolates had severe symptoms more frequently; however, a study in England showed no such evidence [13].
Mortality due to ribotype 027 infection increases with the patient's age. In a Canadian study, 44.1% of the patients were older than 65 yr, and 8.1% of them died within 30 days after diagnosis [14]. In our study, 3 out of 7 patients (42.8%) were older than 65 yr, and none of them died from CDI.
Anti-tuberculous agents are rarely associated with CDI. Among these agents, only rifampin is considered a cause of CDIs because rifampin has an antibiotic effect on a wide range of bacteria, whereas isoniazid and ethambutol have little or no activity against anaerobes [15]. In our study, 4 patients had received rifampin.
In our study, 6 of the 7 isolates were resistant to moxifloxacin; this was also true for the recent epidemic-causing PCR-ribotype 027 strains isolated in other countries. In contrast, the PCR-ribotype 027 strains isolated prior to 2001 were su-sceptible to moxifloxacin [5].
PFGE patterns of 5 isolates (1, 4, 5, 6, and 7) were identical. Compared to the pattern of these 5 isolates, the pattern for isolates 2 and 3 differed in 3 and 2 bands, respectively (Fig. 1). All the isolates were categorized as different MLVA types. The VNTR loci used to discriminate these isolates were CDR4, CDR9, CD48, CDR49, and CDR60. MLVA typing indicated that these isolates were not clones. All the 7 cases had occurred sporadically.
For differentiating the isolates, MLVA was more useful than PFGE.
C. difficile ribotype 027 is uncommon, but it has emerged in Korea. The spread of this ribotype should be closely monitored in order to avoid an outbreak of CDI in Korea.
 XML Download
XML Download