

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hematopoietic stem cell (HSC) transplantation (HSCT) is most often performed in patients with hematologic disorders such as severe aplastic anemia, leukemia, and multiple myeloma [12]. The transplanted HSCs can be derived from bone marrow (BM), peripheral blood (PB), or cord blood. One of the most important factors affecting the outcome of HSCT is the quantity of progenitor cells infused [34]. Higher cell doses have been associated with lower transplant-related mortality rates, faster engraftment, and better survival [56]. The progenitor cell dose is generally measured in terms of the number of viable CD34-positive (CD34+) cells, because CD34 is the most commonly used marker for HSCs/progenitor cells in clinical hematology [567].
The use of peripheral blood stem cells (PBSCs) in HSCT has increased because of an advantage in the hematopoietic function recovery rate [8]. PBSCs can be collected from allogeneic or autologous donor and are usually harvested from PB using leukapheresis. Historically, flow cytometric enumeration of CD34+ cells is the most widely used tool for optimizing harvest timing and the harvest of HSCs for both BM transplantation and PBSC transplantation [9101112]. Ensuring a relatively acceptable turnaround time for flow cytometry is also important to assess the optimal timing and duration of the leukapheresis procedure and processing volume. However, the existing flow cytometric methods require large, complex equipment and skilled operators, and they cannot be performed as urgent or point-of-care tests (POCTs).
A previous study evaluated image based-immunofluorescence cell counter ADAMII (NanoEntek, Seoul, Korea) and showed acceptable analytical performance for enumerating CD34+ cells among total nucleated cells (TNCs); however, its enumeration of TNC was not very accurate because of the presence of dead cells and debris [13]. We evaluated the ability of an improved version of ADAMII (NanoEntek) to enumerate CD34+ cells, which simultaneously analyzed CD45 expression from PB and leukapheresis samples. We specifically considered analytical performance and efficacy as a POCT for determining mobilized stem cell collection time and predicting an adequate apheresis stem cell product.
METHODS
Samples
Nineteen PB samples were obtained from healthy HSC donors following mobilization with granulocyte colony-stimulating factor (G-CSF; 10 µg/kg/day subcutaneously for five days). The samples were collected into potassium EDTA tubes. Ninety-one leukaphersis samples were obtained from 78 donors. Leukapheresis was started on the fifth day of G-CSF administration, and each donor provided one (N=65) or two (N=13) leukapheresis samples. This study was approved by the Institutional Review Board (IRB) of Seoul St. Mary's Hospital, Seoul, Korea, which waived informed consent (IRB No. KC15DIS0369).
CD34+ cell enumeration
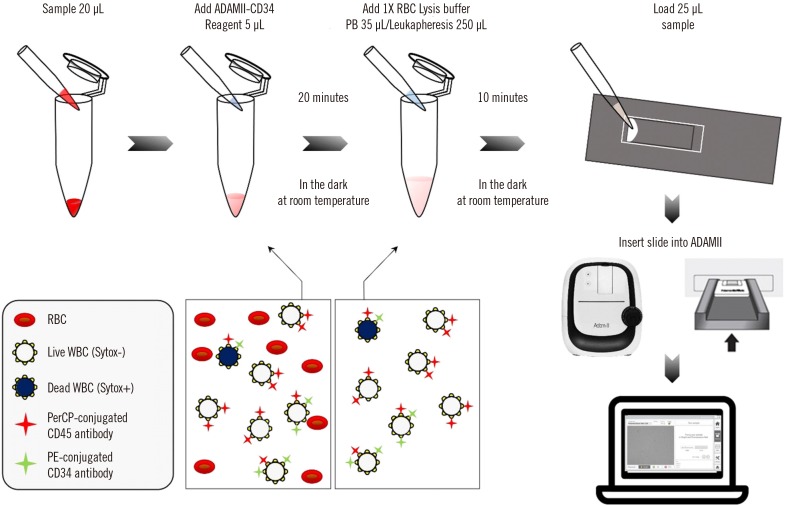
Once the leukocyte count was obtained using Coulter Ac·T diff (Beckman-Coulter, Brea, CA, USA), the PB and leukapheresis samples were diluted with phosphate-buffered serum (PBS) containing 0.5% albumin to a final cell concentration of <10,000 cells/µL and 150,000 cells/µL, respectively. All experiments were performed within 24 hours of sampling according to the manufacturer's instructions. ADAMII is a four-channel (bright field, cells/debris; green, fluorescein isothiocyanate [FITC]-live/dead marker; yellow, phycoerythrin [PE]-conjugated anti-CD34 antibody; and red, peridinin chlorophyll protein complex [PerCP]-conjugated anti-CD45 antibody) bench-top assay of an image-based fluorescence cell counter. Each sample (20 µL) was transferred into a single test tube (Eppendorf, Hamburg, Germany) and incubated with 5 µL of reagent solution containing fluorescence-labeled antibodies and a nucleic acid staining dye from the ADAMII-CD34 kit (NanoEntek). Dead cells were stained using the SYTOX Blue nucleic acid dye (Thermo Fisher Scientific, Waltham, MA, USA). After staining, the red blood cells (RBC) were lysed for adequate image capture; 500–900 signals (cells and debris) per frame. The 25-µL lysed sample was loaded into an ADAMII assay slide (NanoEntek), and the slide was placed on the slide holder of the ADAMII instrument. The ADAMII captured images through each fluorescence channel and analyzed the captured images (136 frames) to enumerate the total and fluorescence-labeled cells based on size, shape, viability, and surface marker (Fig. 1). The following measurements were determined: viable CD34+ cell count (vCD34, cells/µL), viable CD45+ cell count (vCD45, cells/µL), total CD34+ cell count (tCD34, cells/µL), total CD45+ cell count (tCD45, cells/µL), CD34+ cell viability, CD45+ cell viability, and percentage of vCD34+ cells among vCD45+ cells (CD34/CD45, %).
Performance evaluation
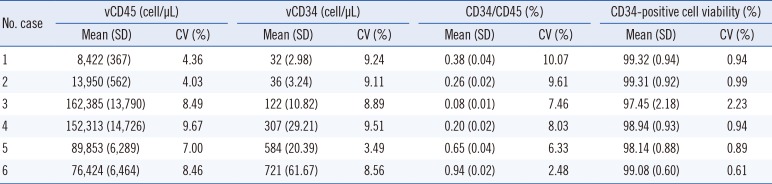
The precision of vCD34 was evaluated according to the CLSI EP5-A2 guidelines [13]. Within-run precision was evaluated using clinical samples with six different vCD34: low (34.4/µL and 37.8/µL), medium (133.3/µL and 360.6/µL), and high (582.9/µL and 773.8/µL). Each sample was analyzed 10 times a day for six days (60 times in total). Precision was assessed using the mean and CV of the analyses including vCD34, vCD45, CD34/CD45, and CD34+ cell viability.
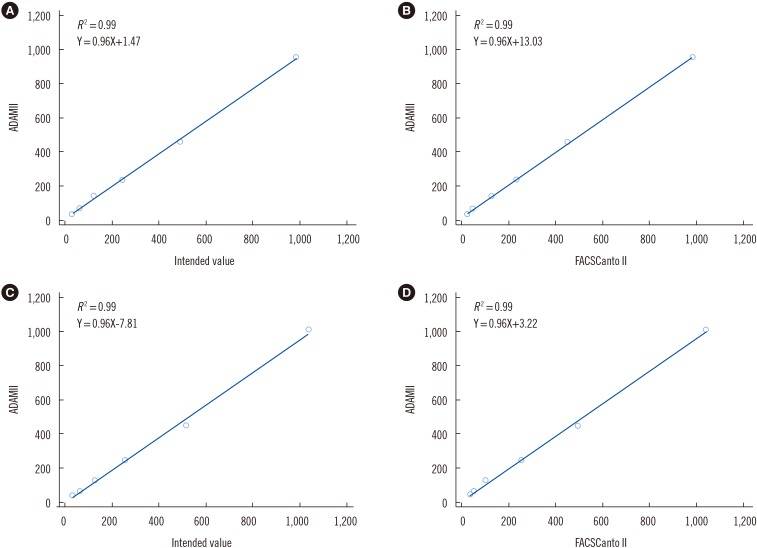
Linearity was evaluated according to the CLSI EP6-A guidelines [14]. Clinical samples with different vCD34 were selected as follows: low (0 cell/µL, non-mobilized PB) and high (985 cells/µL and 1,096 cells/µL). The samples with a high vCD34 were serially diluted five times to produce 12 preparations with ranges of 28–953 cells/µL and 35–1,007 cells/µL, respectively. The intended calculated values were 30.78, 61.56, 123.13, 246.25, 492.5, 985, 32.4, 64.81, 129.61, 259.22, 518.44, and 1,036.88 cells/µL, respectively. Each concentration was measured three times.
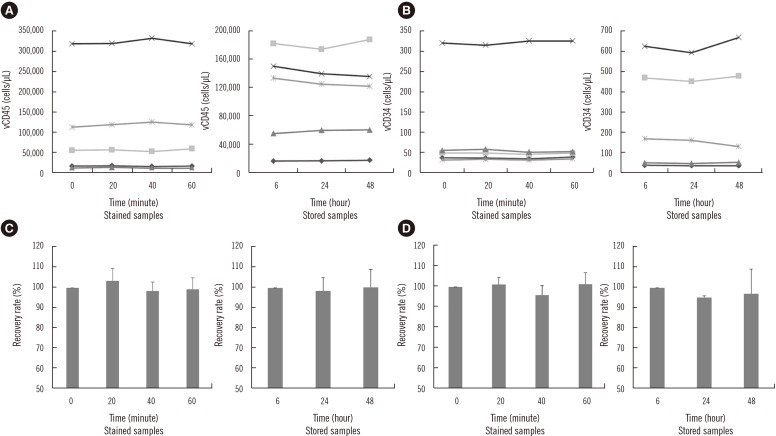
vCD34 and vCD45 stability was evaluated under stained and stored conditions. Two mobilized PB and three leukapheresis samples were stored for up to 48 hours at 4℃ in the refrigerator before staining. The stored samples were tested after six, 24, and 48 hours of storage. Additionally, the three mobilized PB and two leukapheresis stained samples, which underwent changes as a result of the time between staining and data acquisition, were maintained for up to one hour on ice before testing. The acquisition process was performed after the lysing end point at 0, 20, 40, and 60 minutes. The ADAMII assay results from the stored sample stability study were separately analyzed by calculating the percentage of recovery of each sample.
Method comparison
We compared data obtained by ADAMII with those from two flow cytometry instruments: BD FACSCanto II (BD Biosciences, San Jose, CA, USA) and BD FACSAria II (BD Biosciences). The BD Stem Cell Enumeration Kit (BD Biosciences) was used to enumerate CD34+ cells in flow cytometry. Two tubes were prepared for each flow cytometry instrument, and 100 µL of the sample was added into a BD Trucount tube (BD Biosciences) and stained with 20 µL of BD Stem Cell Enumeration reagents (CD45 FITC/CD34 PE) and 20 µL of 7-amino-actinomycin D (7-AAD) nucleic acid for viability. After 20 minutes of incubation at 20–25℃, 2 mL of ammonium chloride lysing solution was added and incubated for 10 minutes in the dark at 20–25℃. Next, 75,000 viable CD45+ cells were acquired to analyze at least 100 viable CD34+ cells. The acquisition process was continued for a maximum of 15 minutes to analyze accurate CD34+ cell enumeration when the sample contained low numbers of CD34+ cells. Acquired data were analyzed using BD FACSCanto clinical software for BD FACSCanto II and BD FACSDiva v6.1.1 software for BD FACSAria II according to the International Society of Hematotherapy and Graft Engineering (ISHAGE) with the 7-AAD protocol [11]. Specifically, vCD34, vCD45, and CD34/CD45 values were quantified.
Statistical analysis
vCD34, vCD45, CD34+ cell viability, and CD34/CD45 (%) were summarized as mean and CV with 95% confidence interval (CI). Normal distribution was determined using the Shapiro-Wilk test. A one-way ANOVA was used to evaluate stability. Linearity was analyzed using Spearman's correlation analysis, and the square of the coefficient of determination (R2) was calculated. Passing–Bablok regression was performed to determine the relationship between the results of the two methods (i.e., ADAMII vs FACSCanto II and ADAMII vs FACSAria II). All statistical analyses were performed using MedCalc version 17.5 (MedCalc, Ostend, Belgium). P<0.05 was considered statistically significant.
RESULTS
CVs of vCD34 ranged from 3.49% to 9.51% and those of CD34/45 ranged from 2.48% to 10.07% (Table 1). The CVs were within acceptable levels at ≤10%. R2 was 0.99 for vCD34 when analyzed with the intended count and flow cytometry data (Fig. 2). No significant changes were observed in vCD45 and vCD34 after sample storage at 4℃ for 48 hours prior to the experiment and storage on ice for one hour before acquisition (Fig. 3).
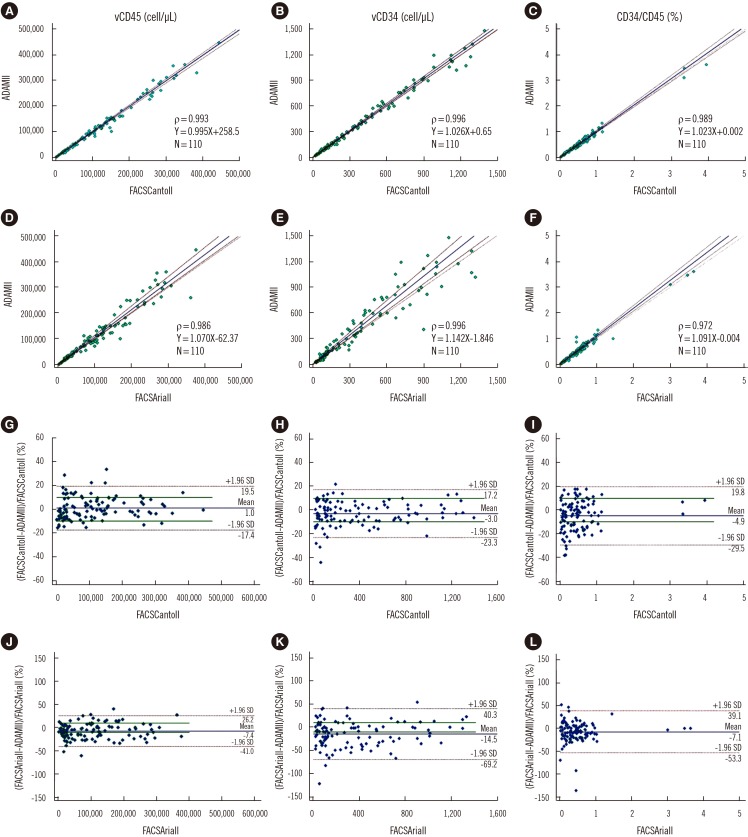
Regression analysis revealed a strong relationship between the ADAMII and FACSCanto II (Fig. 4). Spearman's rho for vCD45, vCD34, and CD34/CD45 between ADAMII and FACSCanto II were 0.993, 0.996, and 0.989, respectively (P<0.0001), and those between ADAMII and FACSAria II were 0.986, 0.979, and 0.972 (P<0.0001). The slope and intercept of the regression line did not significantly differ between the two methods. The Bland–Altman plot showed no significant bias between vCD45, vCD34, and CD34/CD45 of ADAMII and FACSCanto II (data are presented as mean [95% CI]: 2,303.92 [−8.09 to 4,615.92], −7.32 [−15.62 to 0.98], and −0.01 [−0.02 to 0.002], respectively) or between ADAMII and FACSAria II (−6,043.04 [−10,760.06 to −1,296.02], −38.15 [−61.29 to −15.01], and −0.03 [−0.05 to −0.01], respectively).
DISCUSSION
It is well-established that the absolute number of CD34+ cells correlates with in vitro colony-forming unit assay activity and with clinical engraftment of hematopoietic grafts prepared from PB, BM, and cord blood sources [215]. Enumeration of CD34+ cells is based on the staining of cells with a labeled monoclonal antibody against CD34, as well as flow cytometry. Commercial stem cell enumeration kits have been used for simultaneous enumeration of viable CD34+ and CD45+ cells in clinical samples [16]. In addition, a non-flow cytometry-based method, the microvolume fluorimetry-based STELLer CD34 assay, has demonstrated excellent analytical performance [1517]. ADAMII-CD34, an image-based fluorescence cell counter, is another alternative technology that can be used in conjunction with simpler instruments. We evaluated the improved version of the ADAMII, which includes enumerate viable CD45+ cells using a PerCP channel instead of bright channel. This change reduced false detection of CD34+ cells by simultaneously considering the CD45 expression of each cell (Supplemental Data Fig. S1). The vCD45 results obtained using the PerCP channel were slightly lower than TNC from bright channel and similar to vCD45 obtained using FACSCanto II.
The improved ADAMII-CD34 enumeration system showed excellent analytical performance including precision and linearity. A reproducibility of 10% of the mean between replicates is acceptable for routine clinical application of CD34+ cell enumeration [11]; our CVs of vCD34 were within the acceptable range. Comparison of the data showed no significant differences between the various instruments, and the results of ADAMII was strongly related to the results of both FACSCanto II and FACSAria II. We also found that the samples were stable in 4℃ for 48 hours and could be stored on ice for one hour after adding the RBC lysis solution before capturing images. Our results demonstrated that the ADAMII and two flow cytometry-based assays generated very similar data for a range of PB and leukapheresis samples.
A routine clinical CD34+ cell enumeration assay should possess simplicity, high sensitivity, accuracy, reproducibility, and speed [11]. ADAMII is not only satisfactory in terms of analytical performance but is also advantageous because it is a simple and cost-effective instrument. Additionally, this system is technically simple to use and can be used by less experienced laboratory personnel because of its built-in optics and analysis software. All procedures were finished within 40 minutes; hence, use of this system could reduce the waiting time prior to PBSC collection [18]. Intra-procedural CD34+ cell enumeration is also available to estimate the final stem cell yield and to set fixed-volume apheresis [192021]. Furthermore, CD34+ cell enumeration can be repeated on the same day if the precollection PB vCD34 is not sufficient to initiate collection.
In conclusion, ADAMII demonstrated excellent performance as a routine clinical assay with respect to CD34+ cell enumeration obtained from PB and leukapheresis samples. Moreover, it can be used as a POCT for determining optimal timing for mobilized PBSC collection and predicting an adequate apheresis stem cell yield. Our results should be further validated in terms of clinical utility, using a larger number of serial samples from each donor and the relationship of PB vCD34 with vCD34 in leukapheresis sample.
 XML Download
XML Download