

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Primary biliary cholangitis (PBC) is a chronic, progressive, cholestatic liver disease characterized by damage of the biliary epithelial cells and progressive destruction of the bile duct, leading to cirrhosis [12]. A systematic review revealed wide differences in its incidence and prevalence globally [345]. The presence of autoimmune features in patients with PBC has led to the general acceptance of an autoimmune pathogenesis for PBC [67]. In the sera of over 90% of patients, circulating antimitochondrial autoantibodies (AMAs) are found. The main antigens identified are the E-2 subunit of the puryvate dehydrogenase complex (PDH), the branched-chain 2-oxo-acid dehydrogenase complex (BCOADH), and the 2-oxo glutarate dehydrogenase complex (OGDH) [89]. Approximately 50% of PBC patients have antinuclear antibodies (ANAs), which can be detected by indirect immunofluorescence (IIF), line-blot assay, or ELISA [9101112131415].
Specific targets of ANA include the Sp100 protein, major components of nuclear bodies, and constituents of the nuclear envelope (NE) [1617]. Approximately one-third of PBC patients manifest anti-NE positivity, as determined by IIF using commercially available substrates, such as HE p-2 cells [18]. The nuclear pore complex (NPC), one of the components of the nuclear envelope is composed of over 100 proteins, including glycoprotein 210 (gp210), p62, and translocated promoter region (Tpr), which are identified as potential autoantigens. Part of the autoantibodies from PBC patients recognize gp210, an integral glycoprotein of the nuclear pore membrane [1920].
Sasaki et al. [21] immunohistochemically detected the expression of p62 in liver samples of patients with PBC, and concluded that the aggregation of p62 was specifically increased in the damaged bile ducts, which might reflect dysfunctional autophagy, followed by cellular senescence in the pathogenesis of bile duct lesions in PBC. The presence of anti-NPC antibodies can be used to confirm the diagnosis of PBC in atypical cases, especially when AMA are undetectable [22]. Anti-p62 antibodies (anti-p62) can be detected in the serum of PBC patients as well as in those with other autoimmune diseases in very rare cases, but the clinical significance of these antibodies is still poorly understood [23].
We used human recombinant p62 protein and developed a qualitative ELISA technique for the detection these autoantibodies in patients' sera. In the classic ELISA technique, microtiter plates are coated with pure, specific antigen reacting with autoantibodies in the sera. However, a pure human autoantigen is not always accessible, and thus, recombinant animal-derived antigen corresponding to the autoantigen or a peptide corresponding to part of the antigen can be used in such cases. Each of these approaches has its own drawbacks: animal antigens do not always resemble the autoantigen sufficiently for the test to be reliable, antigens obtained by recombination can have different conformations, and the peptide can correspond to a non-immunogenic part of the autoantigen. The difference in immunoreactivity largely depends on the status of the autoantigen. During immunoprecipitation, autoantibodies interact with a native antigen, and in western blotting, a denatured antigen immobilized on the membrane reacts with antibodies. Most clinical laboratories use IIF microscopy to detect antibodies directed against different nuclear components. Anti-p62 are typically tested by immunofluorescence, based on their perinuclear pattern.
We validated our in-house ELISA technique using a recombinant protein, determined the level of anti-p62 in the sera of PBC patients, and compared its diagnostic ability to that of other immunological and biochemical parameters.
METHODS
Study population
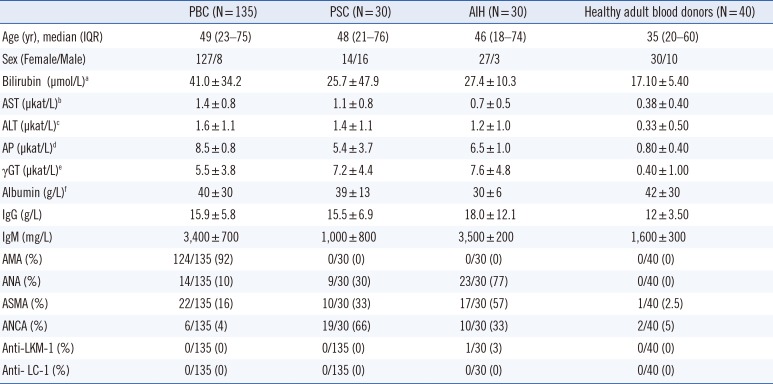
Our study was retrospective. Serum samples were collected from 135 PBC patients (127 women, eight men; median age: 49 years, range 23–75 years), 30 patients with primary sclerosing cholangitis (PSC, 14 women, 16 men; median age: 48 years, range 21–76 years), and 30 patients with autoimmune hepatitis (AIH, 27 women, three men; median age: 46 years, range 18–74 years) who were treated at the Department of Gastroenterology, Hepatology and Clinical Oncology of the Centre of Postgraduate Medical Education, Warsaw (Poland), between January 2003 and December 2014. Samples were frozen at -20℃ or lower. Tests were performed immediately or with archival samples. Sera tested immediately were checked again after storage. The latter two groups were considered pathological controls. Serum samples were also collected from 40 healthy adult blood donors at the Warsaw Blood Bank. The demographic, biochemical, and immunological characteristics of the PBC, PSC, and AIH patients and healthy controls are presented in Table 1.
PBC was diagnosed using the European Association for the Study of the Liver (EASL) guidelines [24]. Patients with abnormal liver function were examined by ultrasound as the first-line noninvasive imaging procedure, and serological screening for AMA and PBC-specific-ANA (presence of nuclear dots or perinuclear rims) was performed with immunofluorescence detection. Biochemical tests of all PBC patients suggested cholestatic liver disease. All patients had a liver biopsy. The main criteria composed of biochemical evidence of cholestasis with elevation of alkaline phosphatase (ALP) activity, presence of AMA and/or anti 2-oxoacid dehydrogenase complex and/or PBC-specific-ANA, histopathologic evidence of characteristic cholangitis, and destruction of small or medium-sized bile ducts. Patients who expressed negative AMA only and met all the other criteria of PBC diagnoses were included. Overall, 11 patients were classified as having AMA-negative PBC. Patients with signs of an overlap syndrome of autoimmune hepatitis (AIH and PBC) and those with a history of alcohol abuse were excluded. Patients with serum positivity for hepatitis B surface antigen (HBsAg), hepatitis A virus antibody (IgM), and hepatitis C virus antibodies were also excluded.
PSC was diagnosed using magnetic resonance cholangiopancreatography or endoscopic retrograde cholangiopancreatography. Liver biopsy was performed to make a diagnosis for patients with suspected small duct PSC or to exclude other conditions, such as suspected overlap with AIH. A positive AMA test helped exclude PBC and an overlap syndrome of PSC and PBC. Patients with PSC were further tested for elevated serum IgG4 levels. Among the 30 patients with PSC, 18 (60%) had inflammatory bowel diseases.
AIH was diagnosed when compatible clinical signs and symptoms, laboratory abnormalities (serum AST or ALT, and increased serum total IgG or c-globulin), serological (ANA, anti-smooth muscle antibodies, anti-liver-kidney microsomal antibody type 1, or anti-liver cytosol type 1) findings, and histological findings were detected. Other conditions that can cause chronic hepatitis were excluded, such as viral, hereditary, metabolic, cholestatic, and drug-induced diseases. Laboratory studies showed levels of AST and ALT<500 U/L, but sometimes ranged between 500 and 800 U/L. Some individuals had a higher level of bilirubin. The ALP generally remains less than two times normal. IgG was 1.2–3.0 times higher than normal. The biopsy sample of a patient with typical features of active AIH shows piecemeal necroses, interface hepatitis, rosette formation and plasma cell enrichment. We used the Revised Original Scoring System of the International Autoimmune Hepatitis Group for assessment [25]. Patients negative for conventional autoantibodies in whom AIH was suspected were further tested for the presence of anti-soluble liver antigen and atypical perinuclear antinuclear neutrophil cytoplasmic antibodies.
The study was approved by the ethics committee (decision 46/PW/2011) of the Medical Center for Postgraduate Education, Warsaw, Poland, and all patients and healthy controls provided written informed consent. The study protocol conforms to the ethical guidelines of the 2008 Declaration of Helsinki.
ELISA for anti-p62 detection
Human recombinant protein p62, prepared using an in vitro wheat germ cell-free protein expression system expression was obtained from Abnova Corporation (Taipei, Taiwan). Wells of flat-bottom microtiter plates (Costar, Corning, NY USA) were coated overnight with 0.1 mL of a 1 µg/mL solution of recombinant 62 protein in 0.1M bicarbonate buffer (pH 9.9) at 4℃, and then saturated with 1.0% bovine serum albumin (BSA) in phosphate-buffered saline (PBS, pH 7.4), and washed with PBS-0.1% Tween (PBS-Tween). Sera from the test groups and controls were incubated in the coated plates for one hr at room temperature (20–22℃) at 1:100 dilution in PBS-Tween with 0.5% BSA. The plates were washed, incubated for one hr at room temperature with 0.1 mL of horseradish peroxidase-conjugated antibodies to human IgG (Daco A/S, Glostrup, Denmark, dilution 1:50,000 in PBS-Tween), and washed again. The color reaction was developed by adding 0.1 mL of tetramethylbenzidine (SERVA Electrophoresis GmbH, Heidelberg, Germany) for 15 minutes and stopped with 0.5 M H2SO4. Optical density (OD) was measured at 450 nm with an automatic plate reader (Multiscan RC, Labsystem, Vantaa, Finland). The final antibody levels were calculated with reference to a serum standard (prepared from pooled human PBC serum samples), which had been diluted to five different concentrations (5, 20, 50, 200, and 500 U/mL). The difference of 2SD corresponded to a cut-off value of OD 0.30 for serum diluted 1:100. Therefore, results below 10 U/mL (cut-off value=mean+2SD) of the levels of healthy donors were arbitrarily determined as negative. Results in the range of 10–20 U/mL were considered borderline or slightly positive. Results above 20 U/mL were considered positive. The intra-assay CV was assessed by running 21 samples. The inter-assay CV was determined by duplicate measurements of 21 serum samples for 10 days.
Detection of anti-pyruvate dehydrogenase (PDH), anti 2-oxoacid dehydrogenase complex, anti-Sp100, and anti-gp210
Anti-PDH and anti-Sp100 antibodies were detected using commercially available ELISA kits: IMTEC-AMA M2 (ITC60040) and IMTEC-Sp100-Antibodies (ITC 660040; IMTEC, Berlin, Germany), according to the manufacturer's instructions. The IMTEC-AMA kit uses PDH, and the IMTEC Sp100-Antibodies kit uses recombinant Sp100 protein.
Anti-2-oxoacid dehydrogenase complex and anti-gp210 antibodies levels were determined by commercially available ELISA kits: QUANTA Lite M2 EP (MIT3) and QUANTA Lite gp210 (Inova Diagnostics, San Diego, CA, USA), according to the manufacturer's instructions. The former kit utilizes an affinity-purified recombinant antigen (MIT3) containing immunodominant portions of PDH-E2, BCOADC-E2, and OGDH-E2, and the latter kit uses a highly purified peptide corresponding to an immunodominant portion of the gp210 protein.
Statistical analysis
Prevalence rates were compared between groups using the chi square test and Fisher's exact test. Continuous data were summarized as mean±SD, and categorical data were summarized as frequencies. Continuous variables were assessed using the Mann-Whitney test and were expressed as median±interquartile range (IQR). P<0.05 were considered statistically significant. All statistical analyses were performed using the Statistica 8.0 software (Stat-Soft, Cracow, Poland) and MedCalc for Windows, version 7.4.1.0 (MedCalc Software, Mariakerke, Belgium).
We calculated the sensitivity, specificity, positive and negative predictive values (PPV and NPV, respectively), and positive and negative likelihood ratio (LR+ and LR-) of our in-house ELISA for diagnosing PBC based on anti-p62 and odds ratio (OR) for the survival. The main outcome measures were time to death from liver failure or time to liver transplantation.
The cut-off value for our ELISA test for anti-p62 detection, classifying cases as positive or negative, was determined utilizing statistical techniques in addition to clinical criteria. The value in which a result can be considered positive was determined by assessing the sensitivity and the specificity. The cut-off value was determined as the upper limit of the 95% confidence interval (CI); that is, an increase in the mean absorbance value for negative individuals by twice the SD (mean+2SD).
ROC curve analysis performed using Prism (GraphPad Software, La Jolla, CA, USA), was conducted to determine whether the cut-off value was a useful statistical tool for our analysis.
RESULTS
Occurrence and diagnostic accuracy for anti-p62 antibodies in primary biliary cholangitis
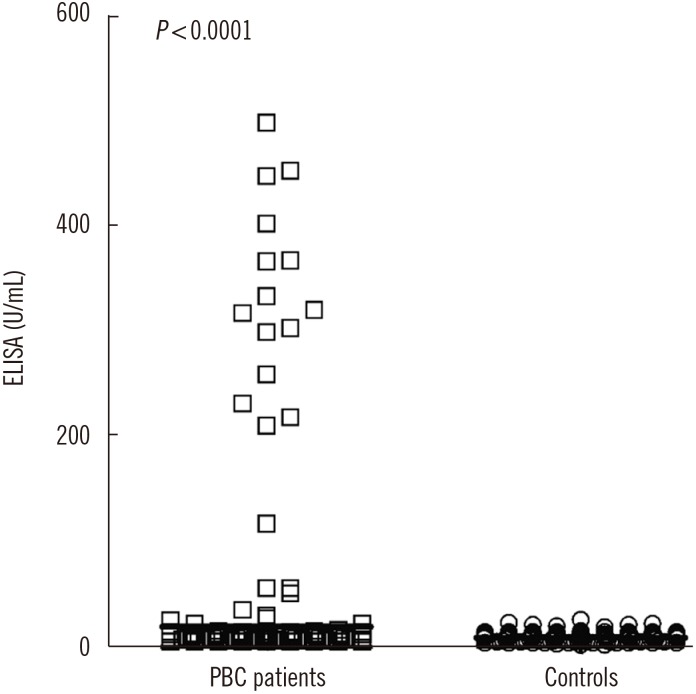
Anti-p62 was found in 32 of 135 (23.7%) PBC patients but in only one of the 30 (3.3%) AIH patients. None of the sera of PSC patients or healthy controls contained anti-p62. The difference between proportions of anti-p62-positive patients and both pathological and healthy controls was 0.23 (95% CI, 0.03–0.40; P<0.0001; Fig. 1).
Overall, 47% of the patients showed a high level of antibodies (101–500 U/mL), with a very high level (>500 U/mL) found in 3% of patients, a low level (21–100 U/mL) in 34% of the patients, and a very low level (10–20 U/mL) detected in 16% of the patients. The inter-assay and intra-assay CVs were 4.1% and 10.2%, respectively.
The specificity for these antibodies detected by ELISA was high, at 99%. The proportion of patients with positive (PPV) or negative (NPV) test results who were correctly diagnosed was 97% and 49%. The positive and negative LR were determined from the 24% sensitivity and 99% specificity at LR+=23.7 and LR−=0.8, respectively.
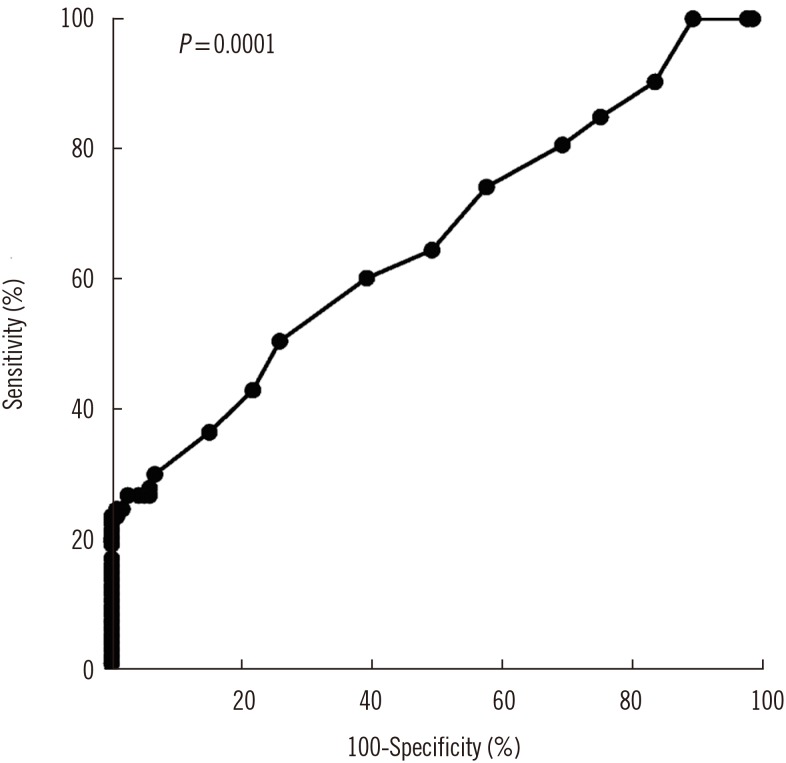
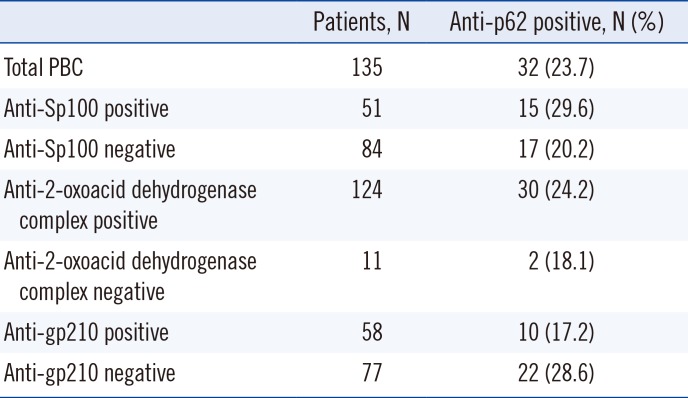
The ROC curve for anti-p62 detected by ELISA is shown in Fig. 2. The area under the ROC curve (AUC) was 0.6830 (95% CI, 0.5865–0.7352). The ROC curve analysis demonstrated that the highest sum of sensitivity and specificity was achieved at the cut-off point of 10.5 U/mL. The comparison of the prevalence of anti-p62 in the study population with that of other specific antibodies that are characteristic of PBC, including anti-2-oxoacid dehydrogenase complex, anti-gp210, and anti-Sp100, is summarized in Table 2.
The prevalence of anti-p62 was higher in patients who were gp210-negative. Among the 32 anti-p62-positive patients, 10 also had anti-gp210 antibodies. Two anti-2-oxoacid dehydrogenase complex-negative but anti-p62-positive patients were positive for only anti-p62.
Age and biochemical features in patients with PBC according to anti-p62 status
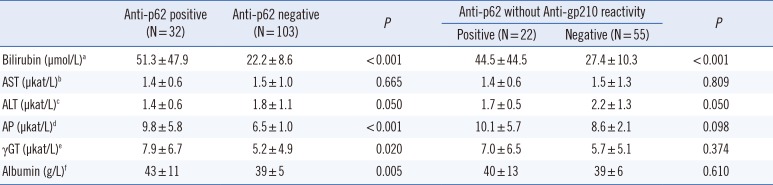
At diagnosis, AST and ALT levels were similar between patients who were positive and negative for anti-p62. However, the anti- p62-positive patients showed much higher levels of bilirubin and ALP (P<0.001; Table 3). Further analysis showed that only the patients who were p62-positive but without anti-gp210 reactivity, showed much higher levels of bilirubin (P<0.001). Among the 135 PBC patients, 56 had a poor outcome (i.e., transplantation or death due to liver disease). Of these 56, 18 were positive for anti-p62 (53%), and 38 were negative for anti-p62 (37%). The calculated OR for survival according to the presence of anti-p62 was 2.20 (95% CI, 0.98–4.92; P=0.055). Moreover, a poor outcome was found in 10/22 (45%) of anti-p62-positive patients without anti-gp210 reactivity and in 14/55 (25%) of patients negative for anti-p62 and anti-gp210 antibodies; the calculated OR for survival excluding anti-gp210 was 2.44 (95% CI, 0.87–6.87; P=0.091).
DISCUSSION
We used human recombinant p62 protein and developed a qualitative ELISA technique to detect these autoantibodies in patient sera. The presence of anti-p62 has also been examined by immunoblotting analysis using nuclear extracts from HeLa cells (HEp-2 cells) [26]. Wesierska-Gadek et al. [27] and Miyachi et al. [28] characterized the native p62 antigen from the NPC by immunofluorescence and immunoblotting.
Wesierska-Gadek et al. [2930] and Invernizzi et al. [31] further demonstrated that approximately 50% of the sera of PBC patients precipitated (35S)-labeled recombinant p62 nucleoporin, and nearly 40% recognized this recombinant antigen by immunoblotting using human recombinant p62 modified by N-acetylglucosamine residues. However, bacterially expressed recombinant proteins can lack native post-translational modifications, which are often linked to the protein's biological function. For example, binding of Wheat Germ Agglutinin (WGA) to N-acetylglucosamine (GlcNAc) residues of p62 protein in the nuclei inhibits the active nucleo-cytoplasmic transport, thereby demonstrating the importance of such post-translational modification on the regulation of protein function. Similar to a glycoprotein, the physiological functions of nucleoporin p62 strongly depend on the glucosamine modification. Under physiological conditions, p62 nucleoporin is modified by GlcNAc residues. In addition, the sugar component of p62 is important for autoantigen detection by circulating autoantibodies [30].
We used a human recombinant p62 protein that was post-translationally processed for our ELISA, which accurately detected anti-p62 in PBC patients. The described quantitative test for anti-p62 is easy to carry out and capable of detecting even small differences in the autoantibody titer among PBC patients, and possibly also detects lower-titer or low-avidity antibodies. This ELISA technique requires smaller amounts of antigen and sera for detection than immunoblotting. Immunoblot is labor-intensive but highly specific, allowing visualization of seroreactivity against specific individual antigens, and is less prone to false-positive results. In the ELISA technique, false negatives, where the amount of antibodies is too low to be measured, and false positives, where an unrelated antibody reacts with the antigen nonspecifically result, may occur. However, ELISA has several advantages, including automation, high-throughput, the ability to normalize autoantigen concentration in the assay, objective/quantitative readout and facile interlaboratory standardization. The availability of the antigen and simplicity of our ELISA technique are also of great clinical importance.
Moreover, the specificity and PPV of the anti-p62 ELISA for PBC patients were very high, at 99% and 97%, respectively. From our calculation of LR+, we determined that the positive test results for our patients would be about 24 times as likely to be obtained in an individual with PBC than in someone without the disorder. The very high LR+ observed (23.7) indicates that the test may be used for PBC diagnosis.
PBC diagnosis is based on precisely defined clinical criteria. However, the prognostic relevance of the presence of circulating autoantibodies against proteins of the NPC remains controversial. Thus, the ability of our ELISA technique to detect anti-p62 and other antinuclear antibodies was also evaluated in the light of actual clinical diagnosis, demonstrating that recombinant anti-p62 may be useful in future serum tests for PBC patients.
Our study was conducted on a group of PBC patients and confirmed a very high specificity of anti-p62. The presence of anti-p62 was also associated with higher levels of bilirubin. Bilirubin has been identified as an independent prognostic marker [3233]. Invernizzi et al. [31] and Wesierska-Gadek et al. [34] reported a correlation between the occurrence of antibodies against NPCs in the sera of PBC patients and clinical outcome. Similarly, Gatselis et al. [35] suggested that PBC-specific ANA was correlated with disease severity.
Although the presence of anti-p62 is fairly rare, a positive result in ELISA strongly supports the diagnosis of PBC. The high specificity of anti-p62 suggests that it may be regarded as a significant serological marker of PBC, even when AMA, anti-gp210, and anti-Sp100 are not detectable.
 XML Download
XML Download