

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Staphylococcus aureus is a major human pathogen, and methicillin-resistant S. aureus (MRSA) is a leading cause of the global threat of hospital-acquired (HA) multidrug-resistant (MDR) organisms [12]. HA-MRSA and community-acquired (CA)-MRSA clones are genetically distinct, and their distribution varies markedly in different regions [12]. MRSA is expected to become endemic in the community, similar to penicillin-resistant S. aureus [3]. Over the past decade, the spread of CA-MRSA in the community and subsequently in the healthcare setting has been associated with the dissemination of specific clones such as USA300-sequence type (ST)8, a highly prominent Panton-Valentine leukocidin (PVL)-positive CA-MRSA in the USA [124].
In Korea, MRSA is highly endemic, constituting 60–81% of clinical S. aureus isolates [56] and 58–64% of bacteremic isolates; ST5-SCCmec type II is the most prevalent HA-MRSA [78910]. HA-MRSA strains have spread to the community [12]. PVL-negative ST72 MRSA is a major CA-MRSA strain [79], which has also emerged as an important healthcare-associated pathogen [11121314]. As veterans' hospitals have long-term cohorts of veterans, they are well-established models for studying HA- and CA-MRSA epidemiology and infection control in the US [1516]. However, no study has examined the epidemiology of S. aureus bacteremia in Korean veterans' hospitals. The Korea Veterans Health Service (VHS), comprising a central hospital and five regional hospitals, provides medical services for veterans nationwide. We investigated the epidemiology and microbiological characterization of S. aureus bacteremia in patients with bacteremia in the central VHS hospital.
METHODS
Patients and bacterial isolates
This observational case-series study was conducted at the VHS Medical Center, Seoul, Korea, which serves half of the national population of veterans, including metropolitan Seoul. This hospital contains 1,000-bed acute- and 400-bed long-term-care facilities. All patients with S. aureus bacteremia were consecutively enrolled from February to August 2015, and S. aureus isolates were collected from their initial blood culture. Patient demographic and clinical findings were retrieved from electronic medical records. The Pitt bacteremia score was used to assess bacteremia severity [17]. The Medical Review Ethics Committee of the VHS Medical Center approved this study and waived the requirement for informed consent (Institutional Review Board number: BOHUN 2015-06-016).
Phenotypic and genotypic analyses
Species identification and antimicrobial susceptibility testing of S. aureus isolated from blood culture were performed using MicroScan Pos Breakpoint Combo panel type 28 (PBC28; Beckman Coulter, West Sacramento, CA, USA), which included antimicrobial wells for penicillin, amoxicillin/clavulanate, azithromycin, clindamycin, daptomycin, erythromycin, fosfomycin, ciprofloxacin, levofloxacin, fusidic acid, gentamicin, imipenem, linezolid, mupirocin, oxacillin, quinupristin/dalfopristin, rifampin, teicoplanin, tetracycline, trimethoprim-sulfamethoxazole, and vancomycin. Methicillin resistance was determined based on resistance to oxacillin or cefoxitin. For all study isolates, agr operon function was measured by δ-hemolysin expression assays using β-hemolysin-producing S. aureus strain RN4220 on blood agar plates, as previously described [18]. agr dysfunction was defined as no enhancement of the β-hemolytic zone. The biofilm assay was performed in polystyrene microtiter plates, as previously described [18]. PCR was conducted for agr polymorphism typing, staphylococcal cassette chromosome mec (SCCmec) typing, spa sequence typing, multilocus sequence typing (MLST), and detection of the lukS-PV and lukF-PV genes for PVL and tst gene for toxic shock syndrome toxin (TSST), as previously described [192021]. spa types were assigned using the RidomStaphType software version 2.2.1 (Ridom GmbH, Munster, Germany) and the SpaServer (http://www.spaserver.ridom.de). MLST allele name and STs were derived from the MLST database (http://www.mlst.net).
Epidemiological investigation and definitions
Bacteremia was classified as HA if blood cultures taken ≥48 hours after admission were positive and as CA if blood cultures taken in an outpatient setting or <48 hours of hospitalization were positive [22]. It was classified as community-onset healthcare-associated (COHA) if the positive cultures were obtained in the CA time frame, but the patient satisfied one or both of the following conditions: 1) a history of hospitalization, surgery, dialysis, or residence in a long-term care facility in the previous one year and 2) the presence of a central venous catheter (CVC) within two days prior to the positive blood culture for S. aureus. Persistent bacteremia was defined as a culture positive for S. aureus ≥72 hours after the onset of appropriate antimicrobial therapy such as glycopeptide antibiotics [23]. Central line-associated bloodstream infection (CLABSI) was designated when the source of bacteremia was assumed to be a CVC, according to the criteria of the US Centers for Disease Control and Prevention's National Healthcare Safety Network [24]. MDR was defined as the resistance to three or more classes of non-β-lactam antimicrobials based on susceptibility to gentamicin, erythromycin, clindamycin, ciprofloxacin, rifampicin, tetracycline, and trimethoprim/sulfamethoxazole.
Statistical analysis
Continuous variables with normal distribution were summarized as mean±SD; variables with non-normal distribution were summarized as median and range or interquartile range (IQR). Categorical variables were expressed as N (%). Differences between MRSA and MSSA were calculated using the chi-square or Fisher's exact tests for categorical variables and Student t-test or Mann-Whitney test for continuous variables. Odds ratios and 95% confidence intervals (CIs) were calculated to measure the association between an S. aureus ST and HA/COHA/CA. P<0.05 (two-sided) was considered statistically significant. All statistical analyses were performed using MedCalc version 16.4.3 (MedCalc Software, Ostend, Belgium).
RESULTS
Patients and bacterial isolates
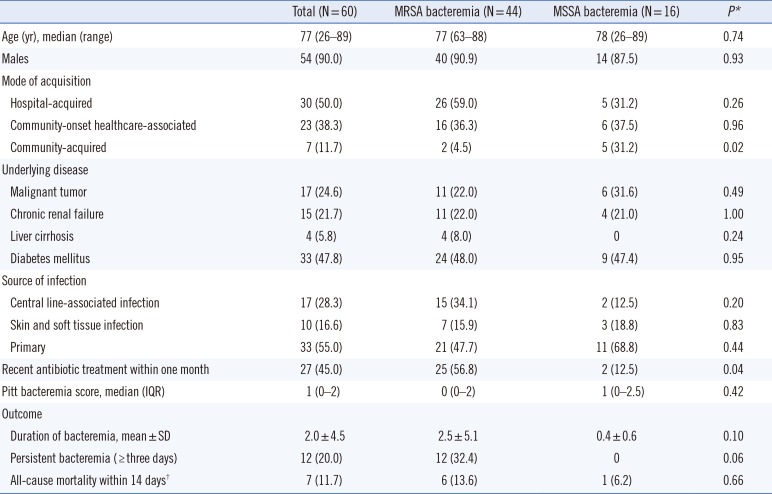
In total, 60 patients with S. aureus bacteremia were enrolled. They were categorized as having HA (30 patients), COHA (23 patients), and CA (seven patients) bacteremia (Table 1). All patients, except one, were aged >60 years, and 54 patients were males. Forty-four patients had one or more serious chronic illnesses, including diabetes, malignancy, chronic renal failure, and liver cirrhosis. The most frequent sources of bacteremia were an indwelling CVC (N=17, 28.3%) or skin and soft tissue infection (N=10, 16.6%) (Table 1). Forty-four (73.3%) patients had MRSA bacteremia. Fifteen (88.2%) of the 17 CLABSI cases and 12 persistent bacteremia cases were caused by MRSA. MRSA bacteremia was more frequent in patients who underwent antibiotic treatment within the past month (P<0.05).
Phenotypic and genotypic characteristics
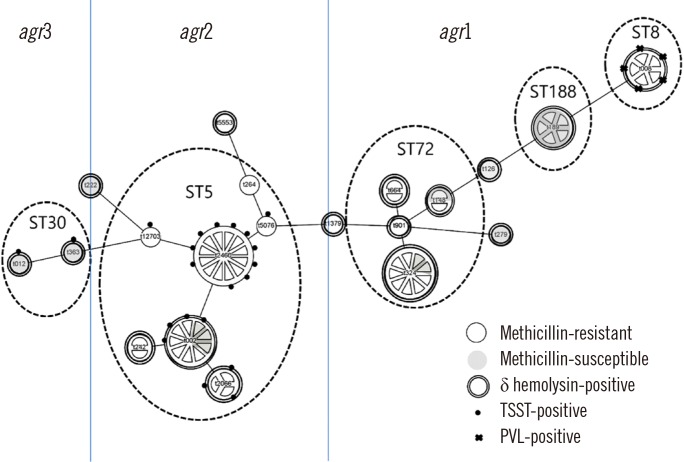
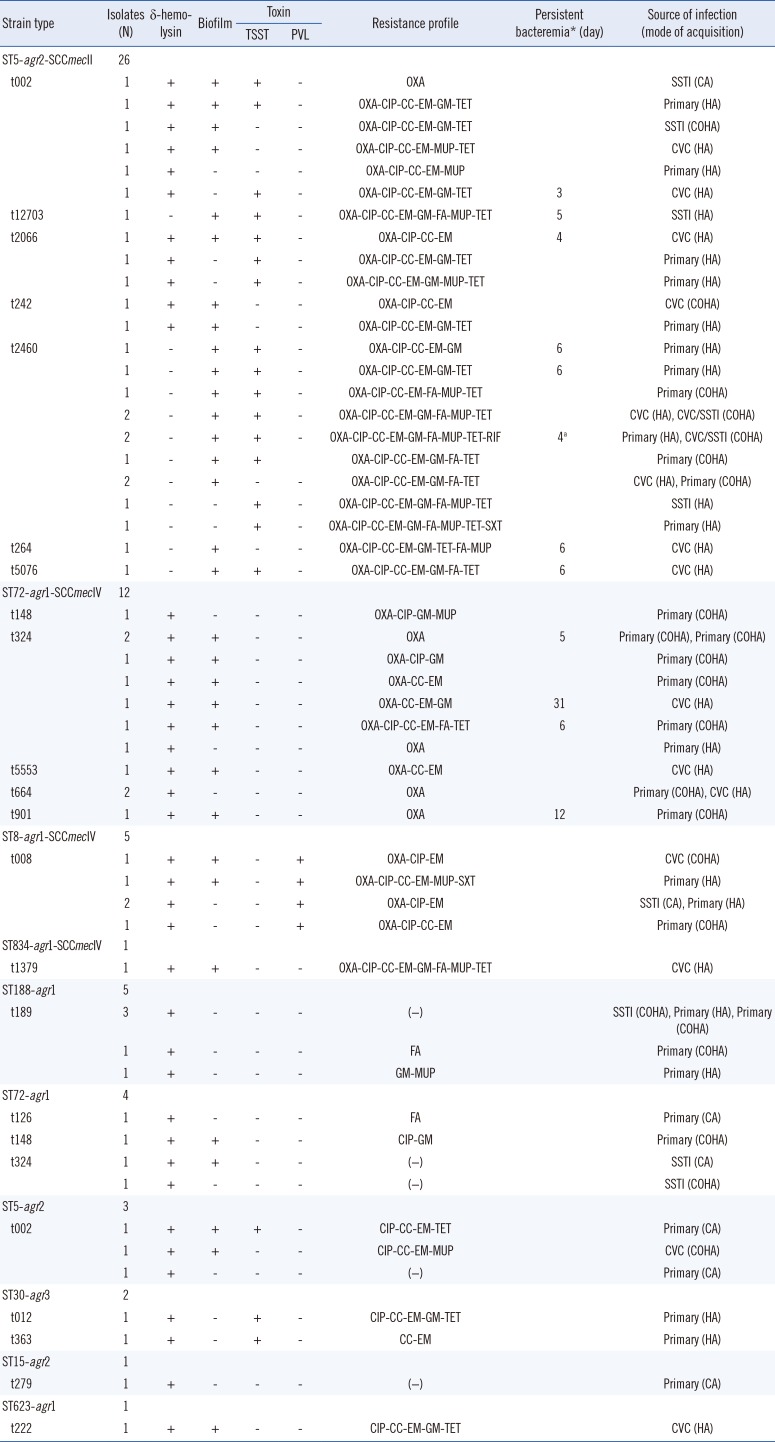
The characteristics of all 60 S. aureus strains are summarized in Table 2. MRSA were grouped into three ST groups: 26 (59%) ST5-agr2-SCCmecII strains comprising 12 t2460, six t002, three t2066, two t242, and three singular types; 12 (27%) ST72-agr1-SCCmecIVa strains (including seven t324, two t664, and two singular types); and five (11%) ST8-agr1 strains, all of which were t008 and SCCmecIV. Methicillin-susceptible S. aureus (MSSA) were heterogeneous, consisting of five ST188-t189-agr1 strains, four ST72-agr1 strains (two t324, one t126, and one t148), three ST5-t002-agr2 strains, two ST30-agr2 strains (t012 and t363), one ST15-t279-agr2 strain, and one ST623-t222-agr1 strain. ST5 MRSA was typically MDR, showing consistent resistance to erythromycin, clindamycin, and ciprofloxacin. ST5-t2460 MRSA was resistant to additional antimicrobials such as gentamicin, fusidic acid, mupirocin, and tetracycline. All strains were completely susceptible to vancomycin with a minimum inhibitory concentration of ≤1 µg/mL. agr1-SCCmecIV MRSA was unlikely to be MDR, and in particular, half of the ST72 MRSA strains were susceptible to all tested antimicrobials other than β-lactams. However, one ST834-agr1-SCCmecIV strain was highly MDR. All ST8-agr1 strains were resistant to ciprofloxacin, and one HA strain was resistant to high-level mupirocin and trimethoprim-sulfamethoxazole, as well as β-lactams.
A schematic summary of the genotypic and phenotypic characteristics of all 60 strains is presented in Fig. 1 based on spa typing. Regardless of methicillin resistance, the ST5 strains were all PVL-negative and frequently tst-positive (65.5%), whereas the ST72 strains were negative for both PVL and tst. In addition, five ST8 MRSA strains were PVL-positive, all ST30 MSSA strains were tst-positive, and δ-hemolysin-negative agr dysfunction was identified in 15 (57.7%) of the ST5 MRSA strains, mainly t2460. All MSSA strains were δ-hemolysin-positive, and one ST30 strain and two ST5 strains were MDR.
In total, 36 (60.0%) isolates were biofilm-positive, including 20 (76.9%) ST5 MRSA, eight (66.7%) ST72 MRSA, and five (31.3%) MSSA. All non-biofilm-forming strains, except two, were δ-hemolysin-positive, and all biofilm-forming strains, except two ST5 MRSA strains, were δ-hemolysin-defective. However, 22 (50.0%) of the 44 δ-hemolysin-positive strains were also biofilm-forming.
Epidemiological characteristics
The HA/COHA/CA bacteremia distribution among the agrII-SCCmecII and agr1-SCCmecIV strains was 18 (69.2%)/six (26.9%)/one (3.8%) and seven (38.9%)/11 (55.6%)/one (5.6%), respectively, while in MSSA strains, it was five (31.3%)/six (37.5%)/five (31.3%). Eighteen (69.2%) and six (26.9%) ST5 MRSA strains were isolated from HA- and COHA bacteremia, respectively. One ST5 MRSA was resistant to only oxacillin and isolated from CA bacteremia. Of the five ST8 MRSA strains, four were healthcare-associated, including two HA and two COHA. agr1-SCCmecIV strains were more likely to be COHA than agr2-SCCmecII strains (odds ratio, 3.4; 95% CI, 0.95–12.09) or MSSA (odds ratio, 2.1; 95% CI, 0.52–8.23). In particular, two thirds of the ST72 MRSA strains were isolated from COHA-bacteremia.
All δ-hemolysin-defective strains were healthcare-associated, and 10 of the 15 δ-hemolysin-defective ST5 MRSA strains were HA (Table 2). All CLABSI-causing S. aureus strains, except one, were biofilm-positive and 11 (64.7%) of those were HA-MRSA. Nine (75.0%) of 12 persistent bacteremia cases were HA, seven of which were caused by TSST-producing ST5 MRSA. Six of the HA-CLABSI cases resulted in persistent bacteremia, caused by five ST5 MRSA strains and one ST72 MRSA strain. No cases of persistent bacteremia were caused by PVL-producing ST8 MRSA strains.
DISCUSSION
MRSA is highly endemic in Korea, regardless of hospital size or complexity; however, MRSA prevalence (73.3%) in this study is much higher than those reported in Korean hospitals previously (51.4–54.3%) [2829]. The patient population of the central VHS hospital is unique, comprising predominantly elderly males, with a high percentage of long-term repeat visitors and a high transfer rate from regional veterans' hospitals or long-term care facilities all over Korea. Therefore, more S. aureus bacteremia cases than usual are likely to be healthcare-associated. The proportions of MRSA in HA and COHA bacteremia were not significantly different as 83.3% and 73.9%, respectively, and were much higher than that of CA bacteremia (28.7%). HA or COHA MRSA accounted for 90% of S. aureus bacteremia cases, clearly contributing to the high prevalence of MRSA in this hospital. In addition, the high prevalence of COHA-MRSA bacteremia indicated the possibility of the spread of HA-MRSA into the community and subsequent re-emergence in the healthcare setting via COHA transfer.
The major HA or COHA-MRSA strains in this study were ST5 MRSA, ST72 MRSA, and ST8 MRSA. ST239 was not detected in this study, although it had been previously considered as a representative HA-MRSA strain in Korea [128]. ST72, a typical CA-MRSA strain in Korea over the last decade, displayed CA-MRSA characteristics, such as non-MDR traits and the presence of SCCmecIV; however, all ST72 MRSA strains in this study were from healthcare-associated infections (75% COHA and 25% HA). ST72 MRSA seemed to play a major role in the spread of CA-MRSA to the hospital via COHA transfer. The prevalence of ST239 has recently decreased in Korea [6830], and ST72 MRSA has been found to be the most common clone in both CA- and HA-MRSA infections in Korean pediatric patients [1331]. The absence of ST239 and the presence of only a few major MRSA strains in this hospital provide evidence of the clonal spread of MRSA, indicating that a rapid change in MRSA clones is possible in a hospital.
The main ST5 MRSA was ST5-agr2-SCCmecII, which belongs to the New York–Japan clone and is known to be dominant in the adult Korean population [1013]. The ST5-t2460 strain is a well-known tst-positive MRSA clone in Korea [8914], and it was a main agr-defective strain in the present study. agr-defective strains are associated with high mortality, biofilm formation, prolonged bacteremia, and reduced susceptibility to vancomycin [814]. However, the minimum inhibitory concentration of vancomycin for all the isolates in this study was<2 µg/mL, in contrast to previous findings about the New York–Japan clone [32]. Therefore, to our knowledge, this is the first study to demonstrate that ST5-t2460-MRSA is a predominant and highly threatening pathogen in healthcare-associated bacteremia, with a high virulence in Korea.
ST72 MRSA in the present study was PVL-negative, harbored SCCmecIV, belonged to agr1, and was unlikely to be MDR. PVL-negative ST72-agr1-SCCmecIV, a major CA-MRSA over the last decade, has the advantage of fitness cost in the community because of the small size of SCCmec [33]. However, this clone has recently emerged as a healthcare-associated pathogen in Korea [11121314]. In our study, all of ST72 MRSA bacteremia cases were healthcare-associated, and the high prevalence of ST72 among MRSA bacteremia cases suggests that continuous introduction of COHA-MRSA has contributed to the high prevalence of MRSA bacteremia.
Notably, we revealed that the emergence of PVL-positive ST8-agr1-SCCmecIV strains was responsible for approximately 10% of MRSA bacteremia cases. This strain is likely to be USA300 clone, which first emerged as CA-MRSA with high virulence and then successfully spread into healthcare settings in the USA [27]. Cases of sporadic USA300 outbreaks have been reported since the first case was imported from Hawaii into Korea in 2007 [9252634]. This strain was both community- and healthcare-associated in our study, consistent with a recent multicenter study [35]; however, it exhibited increased resistance to antimicrobials. The spread and evolution of this PVL-positive strain should be closely monitored because of its high virulence and ability to spread to both community and healthcare settings.
Among the MSSA strains, ST188, ST72, ST5, and ST30 occurred most frequently, consistent with previous findings in Korea [836]. ST188-t198, ST72-t126, and -t324 were linked to agr1 and susceptible to antimicrobials, whereas ST5-t002 and ST30-t012 were linked to agr2 and agr3, respectively, and more likely to be MDR. One ST5-t002 harbored tst and was MDR, thus having a common trait with ST5 MRSA. These findings suggested cure of methicillin resistance by excision of the mecA gene from ST5-MRSA [37]. All MSSA strains had intact agr function. Although agr dysfunction in MSSA is rare, one study reported 12.5% agr dysfunction among MSSA blood isolates in Korea and very high agr dysfunction (89.4%) for ST5 MRSA [8].
This study has important limitations. Because this is the first epidemiological study on S. aureus in Korean VHS hospitals, more longitudinal studies are required to interpret the characteristics of high MRSA prevalence and MRSA clonality better. Furthermore, as this is an observational case-series study, clinical and laboratory evaluations were not regulated, and thus, outcome analyses were limited.
In conclusion, we identified the wide spread of ST5-agr2-SCCmecII, a typical agr-defective HA clone, from hospital to community and of ST72-agr1-SCCmecIV, a typical CA clone, from community to hospital in a Korean VHS hospital. We also confirmed that the PVL-positive ST8 MRSA strain was prevalent both in the community and the healthcare setting and acquired the MDR character. Clinicians and clinical microbiologists should note that COHA-MRSA is prevalent in S. aureus bacteremia.
 XML Download
XML Download